Acute mountain sickness physiology
"acute mountain sickness" physiology
Acute Mountain Sickness (AMS) - Physiology
Definition & Epidemiology
- Harrison's Principles of Internal Medicine, 22E, p. 3798
The Primary Trigger: Hypobaric Hypoxia
- Medical Physiology (Boron & Boulpaep), p. 689
Pathophysiology - Central Mechanisms
1. Cerebral Vasodilation and Edema (Core Mechanism)

- Harrison's, p. 3799; Guyton & Hall, p. 554
2. Blood-Brain Barrier Disruption
-
VEGF (Vascular Endothelial Growth Factor) - first proposed in 1995, shown to promote capillary leakage; dexamethasone (an effective AMS treatment) blocks hypoxic VEGF upregulation
-
Histamine and arachidonic acid - inflammatory mediators
-
Nitric oxide - calcium-mediated; promotes cerebral vasodilation
-
Adenosine - neuronally mediated; contributes to cerebral vasodilation
-
Harrison's, p. 3799
3. Impaired Cerebral Autoregulation
4. Venous Outflow Obstruction
5. High-Altitude Headache - Trigeminovascular Activation
- Harrison's, p. 3799
Pathophysiology - Pulmonary Mechanisms (HAPE)
High-Altitude Pulmonary Edema (HAPE)
- Hypoxic Pulmonary Vasoconstriction (HPV) - hypoxia causes pulmonary arteriolar constriction, raising pulmonary vascular resistance
- Uneven vasoconstriction - HPV is non-uniform; some vessels constrict more than others, forcing blood through fewer remaining open capillaries
- Focal capillary hypertension - in the still-perfused segments, capillary pressure rises dramatically
- Capillary stress failure and transudation - the high pressure causes fluid leakage into alveolar spaces, producing pulmonary edema
- VEGF and inflammatory cytokines may further increase pulmonary capillary permeability
- Guyton & Hall, p. 554; Medical Physiology (Boron), p. 689
Risk Factors
| Factor | Details |
|---|---|
| Rate of ascent | Most important modifiable factor |
| Prior altitude illness | Strong predictor of recurrence |
| Exertion at altitude | Increases risk; physical fitness does NOT protect |
| Blunted hypoxic ventilatory response (HVR) | Less hyperventilation → worse hypoxemia → greater vasodilation |
| Low oxygen saturation on exercise | Independent predictor of severe illness |
| Patent foramen ovale (PFO) | Allows right-to-left shunting, worsening hypoxemia |
| Carotid body damage | Neck irradiation/surgery impairs chemoreception |
| Dehydration, respiratory infection | Additional risk factors |
| Age >50 | May be less susceptible than younger adults |
- Medical Physiology (Boron), p. 689; Harrison's, p. 3798
The "Tight Fit" Hypothesis
- Harrison's, p. 3798
Acclimatization vs. AMS (Why Most People Adapt)
- Immediate hyperventilation (raises PaO2, lowers PaCO2 → respiratory alkalosis)
- Renal bicarbonate excretion compensates for alkalosis over 2-3 days
- Gradual increase in erythropoietin → polycythemia over weeks
- Increased 2,3-DPG → rightward shift of O2-Hb curve
Treatment - Physiologic Rationale
| Condition | Treatment | Mechanism |
|---|---|---|
| All AMS/HACE | Descent | Removes hypobaric hypoxia - the root cause |
| All AMS/HACE | Supplemental O2 | Directly corrects hypoxemia |
| Mild/Moderate AMS | Acetazolamide (250 mg q12h) | Carbonic anhydrase inhibitor; forces renal bicarbonate excretion, mimicking acclimatization; stimulates ventilation |
| Moderate AMS / HACE | Dexamethasone (4-8 mg) | Reduces cerebral edema; blocks VEGF upregulation |
| HAPE | Nifedipine (30 mg ER q12h) | Pulmonary vasodilator; counteracts HPV |
| If descent impossible | Portable hyperbaric chamber | Simulates descent by increasing ambient pressure |
- Harrison's, Table 475-1, p. 3799
Summary of Pathophysiologic Cascade
High Altitude
↓
Hypobaric Hypoxia (↓ PiO2)
↓
↓ PaO2 → ↑ Hypoxic Ventilatory Response (HVR)
↓ ↓
Inadequate HVR Good HVR → Acclimatization
↓
Persistent Hypoxemia
↙ ↘
BRAIN LUNG
↑ CBF, vasodilation HPV → uneven vasoconstriction
↑ Capillary pressure ↑ Focal capillary pressure
↑ BBB permeability ↑ Pulmonary permeability
(VEGF, histamine, (VEGF, cytokines)
nitric oxide)
↓ ↓
Vasogenic cerebral edema Pulmonary edema
(AMS → HACE) (HAPE)
↓
Trigeminovascular activation → Headache
Raised ICP → Nausea, ataxia, altered consciousness
Generate flowcharts photo
A detailed medical flowchart showing the pathophysiology of Acute Mountain Sickness (AMS). The flowchart starts at the top with "High Altitude" flowing down through: Hypobaric Hypoxia → Reduced PaO2. Then it splits into two parallel branches. Left branch (Brain pathway): Cerebral Vasodilation → Increased Cerebral Blood Flow → Raised Capillary Pressure + BBB Disruption (VEGF, Histamine, Nitric Oxide) → Vasogenic Cerebral Edema → AMS symptoms (Headache, Nausea, Fatigue) → HACE (Ataxia, Altered Consciousness). Right branch (Lung pathway): Hypoxic Pulmonary Vasoconstriction → Uneven Vasoconstriction → Focal Capillary Hypertension → Pulmonary Edema → HAPE. At the bottom, both branches converge into a Treatment box showing: Descent, Oxygen, Acetazolamide, Dexamethasone, Nifedipine. Use clean medical diagram style with blue and red color coding for brain and lung pathways respectively, white background, clear arrows, bold headings, and professional typography.
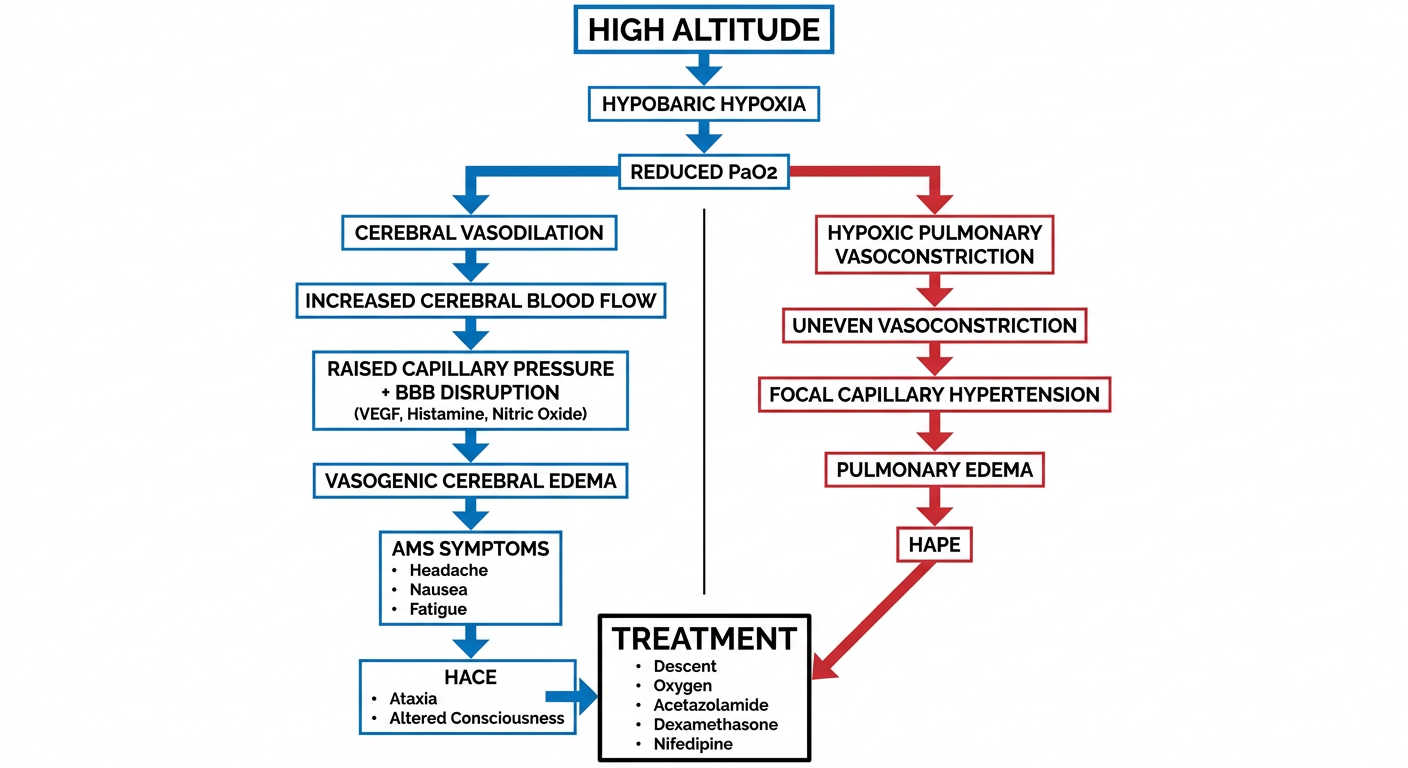
- Trigger - High altitude → Hypobaric Hypoxia → ↓ PaO2
- Brain pathway (blue) - Cerebral vasodilation → ↑ CBF → BBB disruption (VEGF, Histamine, NO) → Vasogenic cerebral edema → AMS → HACE
- Lung pathway (red) - Hypoxic pulmonary vasoconstriction → Uneven constriction → Focal capillary hypertension → HAPE
- Treatment box - Descent, O2, Acetazolamide, Dexamethasone, Nifedipine