Wound
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
I now have comprehensive information from multiple authoritative surgical textbooks. Here is a full overview of wound classification and types:
Wound Classification & Types
A wound is any disruption of the normal anatomy and function of tissues caused by physical, chemical, thermal, or biological agents. Wounds can be classified across several dimensions:
1. Classification by Aetiology (Mechanism)
| Type | Description |
|---|---|
| Incised (surgical/clean) | Made by a sharp instrument; clean edges; minimal tissue damage |
| Lacerated | Torn or irregular edges; caused by blunt trauma |
| Crush | Caused by compressive force; significant tissue disruption |
| Abrasion | Superficial scraping of skin; loss of epidermis/dermis |
| Puncture | Small entry point but deep track; high infection risk |
| Avulsion/Degloving | Skin and soft tissue torn away from underlying structures |
| Blast | High-energy explosion injury; complex contamination |
| Burn | Thermal, electrical, chemical, radiation, or mechanical |
| Cold injury | Frostbite; ischaemic tissue damage |
| Bite | Human or animal; high contamination risk |
- Bailey and Love's Short Practice of Surgery, 28th Ed.
2. Classification by Depth
| Level | Structures Involved |
|---|---|
| Epidermal | Epidermis only (e.g., superficial abrasion) |
| Dermal - superficial partial thickness | Extends into superficial dermis; pain fibres intact; heals without grafting |
| Dermal - deep partial thickness | Into deep dermis; may need grafting |
| Full thickness | Through entire dermis into fat/muscle/bone; requires grafting or closure |
For burns specifically, depth assessment uses:
-
History (duration and temperature of exposure)
-
Appearance (red, mottled, white/yellow/brown)
-
Pin-prick test - if sensation is retained, the wound is superficial; if insensate, deep dermal or full thickness
-
Pye's Surgical Handicraft, 22nd Ed.
3. Surgical Wound Classification (CDC/NRC System)
This is the most widely used classification in surgical practice:
| Class | Name | Definition | SSI Risk |
|---|---|---|---|
| I | Clean | No inflammation; respiratory, GI, GU, or genital tracts NOT entered; primarily closed | 1-5% (historical); 1.8-2.6% (2014 data) |
| II | Clean-contaminated | Respiratory, GI, GU, or genital tracts entered under controlled conditions; no major break in sterile technique | 3-11% / 4.8-6.7% |
| III | Contaminated | Open, fresh (< 4 hours), accidental wound; major break in sterile technique; gross GI spillage; acute non-purulent inflammation | 10-17% / 5.6-8.6% |
| IV | Dirty/Infected | Old wound (> 4 hours); devitalised tissue present; existing infection or perforated viscera | >27% / 8.5-11.8% |
Class I examples: Hernia repair, thyroidectomy, CABG, mastectomy, hip/knee replacement
Class II examples: Small bowel resection, hysterectomy, lobectomy, Whipple procedure
Class III examples: Acute cholecystitis, non-perforated appendicitis, bowel infarct
Class IV examples: Peritonitis, perforated appendicitis, perforated peptic ulcer, open fracture repair
- Current Surgical Therapy, 14th Ed. | Bailey and Love's, 28th Ed.
4. Classification by Complexity
| Category | Description |
|---|---|
| Simple | No significant tissue loss; clean; primary closure possible |
| Complex | Significant soft-tissue loss, open fracture/joint, or visceral involvement |
| Complicated | Wound with secondary pathology: infection, necrosis, haematoma, gas gangrene, or compartment syndrome |
5. Classification by Chronicity
| Type | Description |
|---|---|
| Acute | Traumatic or post-surgical; follows normal healing trajectory |
| Chronic | Fails to heal in expected timeframe; includes: |
| - Venous ulcers | Lower limb; associated with venous insufficiency |
| - Arterial ulcers | Ischaemic; punched-out; distal extremities |
| - Diabetic ulcers | Neuropathic/ischaemic; pressure points of feet |
| - Pressure ulcers | Over bony prominences; staged I-IV by depth |
6. Open vs. Closed Wounds
-
Open wounds heal by secondary intention - contraction, granulation tissue, and re-epithelialisation; more inflammation and scarring; risk of desiccation of exposed structures (tendons, bone, nerves)
-
Closed wounds heal by primary intention (edges approximated by sutures/staples/glue); less inflammation, narrower scar, faster healing
-
Delayed primary closure (tertiary intention) - contaminated wounds left open initially and closed at 3-5 days once infection risk decreases
-
Roberts and Hedges' Clinical Procedures in Emergency Medicine
Summary: Key Classification Axes
| Axis | Options |
|---|---|
| Aetiology | Incised, lacerated, crush, abrasion, puncture, avulsion, burn, bite, blast |
| Depth | Epidermal, superficial dermal, deep dermal, full thickness |
| Contamination | Clean (I), Clean-contaminated (II), Contaminated (III), Dirty (IV) |
| Complexity | Simple, complex, complicated |
| Chronicity | Acute vs. chronic |
| Healing method | Primary, secondary, tertiary intention |
Explain the phases of normal wound healing
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, authoritative content from Sabiston's and Schwartz's Surgery. Here is the full detailed explanation:
Phases of Normal Wound Healing
Wound healing is a dynamic, continuous process that unfolds over four overlapping phases. The phases do not simply stop and start - they exist as a continuum, and each phase must complete in an orderly, timely fashion for repair to succeed. Disruption of any phase - by diabetes, infection, ischaemia, or malnutrition - can lock a wound in a dysfunctional cycle.
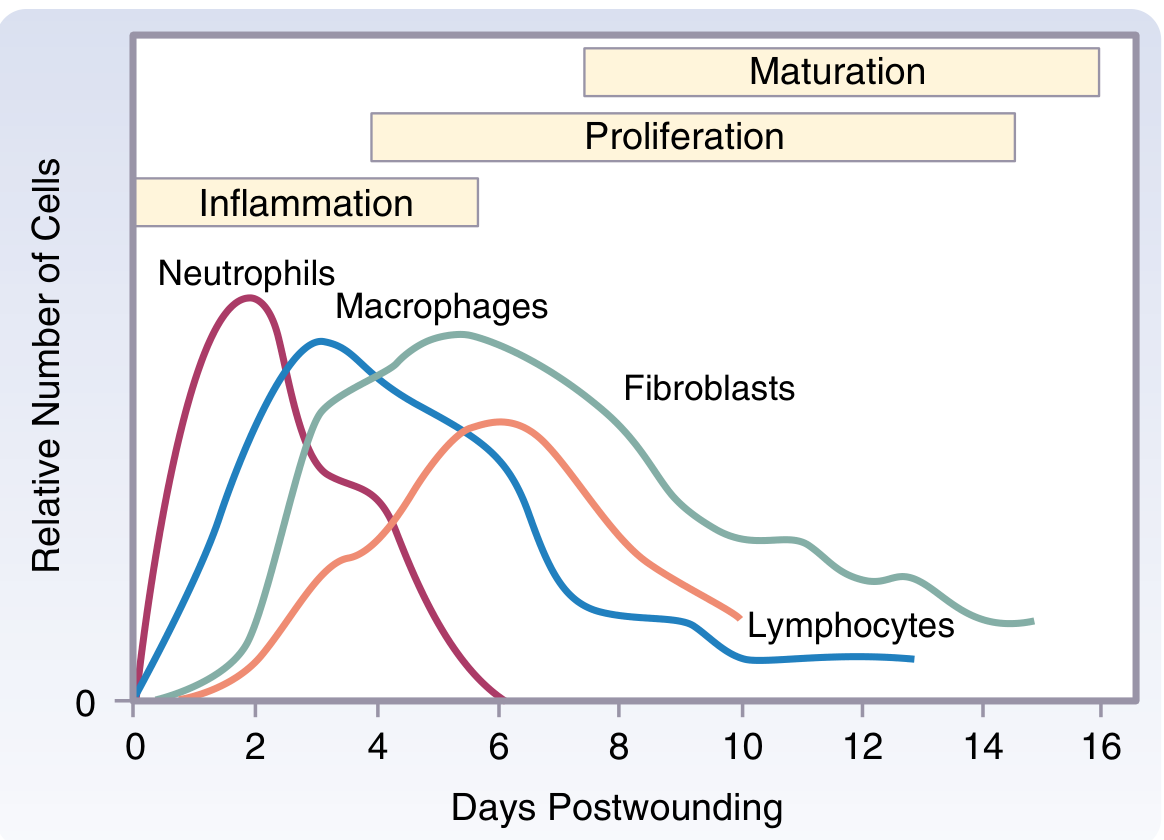
Cell kinetics across the phases of wound healing. Neutrophils dominate early inflammation; macrophages bridge inflammation to proliferation; fibroblasts dominate the proliferative phase.
Phase 1 - Haemostasis (Seconds to Hours)
Goal: Stop bleeding and seal the wound.
Key events:
-
Vascular injury triggers intense arteriolar vasoconstriction (mediated by catecholamines and prostaglandins), followed by vasodilatation and increased capillary permeability
-
Platelet adhesion to the damaged endothelium is mediated by glycoprotein receptors (GPIa/IIa) binding to exposed collagen, and GPIIb-IIIa binding fibronectin, vitronectin, and fibrinogen; von Willebrand factor (vWF) is essential for initial platelet-collagen contact
-
Platelet activation triggers release from two organelles:
- Alpha granules → PDGF, TGF-β, IGF-1, fibronectin, fibrinogen, thrombospondin, vWF
- Dense bodies → serotonin and vasoactive amines → vasodilation and increased permeability
-
Mast cells release histamine and serotonin, further increasing endothelial permeability
-
Platelet membrane-bound factor V + factor X generate prothrombinase, activating thrombin, which converts fibrinogen to fibrin clot (the provisional wound matrix)
-
The fibrin clot also acts as a scaffold for subsequent cell migration
-
Growth factors released (PDGF, TGF-β, VEGF, PF4, CD40L) create a chemotactic gradient that recruits inflammatory cells and initiates the next phase
-
Sabiston Textbook of Surgery | Schwartz's Principles of Surgery, 11th Ed.
Phase 2 - Inflammation (Days 1-4)
Goal: Clear debris, bacteria, and devitalised tissue; prepare the wound bed.
Vascular changes: The increased permeability established during haemostasis allows plasma proteins and leukocytes to flood the wound. Clinically: redness, warmth, swelling, pain, and loss of function (the cardinal signs of inflammation).
Neutrophils (PMNs) - first responders, peak day 1-2
- Arrive within hours of injury, peak at ~48 hours
- Primary functions: phagocytosis of bacteria and debris; release of reactive oxygen species (ROS) for bacterial killing; release of proteases (elastase, collagenase) to break down devitalised tissue
- Not essential for healing in clean wounds (animal models show healing can proceed without neutrophils if infection is controlled), but essential when contamination is present
- Apoptose and are cleared by macrophages as the wound becomes clean
Macrophages - the "master regulators," peak day 3-4
Macrophages are the most important cells in wound healing. They arrive shortly after neutrophils and persist into the proliferative phase. Their functions span 7 categories:
- Phagocytosis of apoptotic neutrophils, bacteria, and foreign material
- Reactive oxygen species - bacterial lysis
- Nitric oxide - kills antibiotic-resistant bacteria
- Cytokine secretion - IL-1, IL-2, IL-4, IL-12
- Angiogenesis - via VEGF, promoting capillary budding
- Cell recruitment - recruits fibroblasts and endothelial cells into the wound
- Homeostatic regulation - wound repair, follicle regeneration
Macrophage depletion before injury causes profound defects: failed re-epithelialisation, absent granulation tissue, no angiogenesis, and no myofibroblast-mediated wound contraction. Depletion at day 9 has no effect, confirming macrophages are dispensable later.
Two macrophage phenotypes exist:
- M1 (classically activated) - pro-inflammatory; dominant early; kills bacteria; secretes TNF-α, IL-6
- M2 (alternatively activated) - anti-inflammatory; dominant later; promotes tissue repair, collagen synthesis, angiogenesis
Lymphocytes - appear late, peak day 7
- Modulate the transition from inflammation to proliferation
- T-helper cells secrete cytokines that regulate fibroblast activity
What determines chronicity: The inflammatory phase is the fork in the road between acute and chronic wounds. In chronic wounds, persistent pro-inflammatory conditions trap the wound in a self-perpetuating cycle where PMNs and macrophages continually degrade newly formed matrix, preventing progression to proliferation.
- Sabiston Textbook of Surgery | Schwartz's Principles of Surgery, 11th Ed.
Phase 3 - Proliferation (Days 4-21)
Goal: Fill the wound defect with new tissue (granulation tissue) and resurface it with epithelium.
This phase has three concurrent subprocesses:
3a. Angiogenesis (new vessel formation)
- Activated endothelial cells degrade the basement membrane of post-capillary venules
- Endothelial cells migrate into the wound along the fibrin scaffold using integrin αvβ3 (binds fibrin, fibronectin, fibrinogen)
- PECAM-1 mediates cell-cell contacts as capillary tubes form
- Stimulated by: VEGF, FGF, PDGF, TGF-β
- Results in the formation of granulation tissue - a highly vascularised, red, moist tissue filling the wound
3b. Fibroplasia (collagen synthesis by fibroblasts)
- Fibroblasts migrate into the wound along the fibrin matrix from day 4, peaking ~day 7-10
- Driven by PDGF (the key fibroblast mitogen) and TGF-β
- Fibroblasts synthesise type III collagen initially (weaker, more flexible), and later convert to type I collagen (stronger)
- Normal skin: 80% type I / 20% type III
- Early wounds: increased type III collagen
- Collagen is secreted as procollagen, cleaved extracellularly to tropocollagen, and then assembled into collagen fibrils (10-300 nm) and fibers (micrometres)
- The wound matrix also contains fibronectin, hyaluronic acid, proteoglycans - forming the ECM scaffold
- MMPs (matrix metalloproteinases) regulate matrix remodelling; MMP-1 (collagenase) is induced by IL-1 and downregulated by TGF-β; plasmin activates procollagenase to collagenase
3c. Re-epithelialisation
- Keratinocytes at the wound edge flatten, lose their attachments, and migrate across the wound surface
- Stimulated by: EGF, KGF (FGF-7), TGF-α, IL-6
- Keratinocytes proliferate behind the migrating front and eventually restore the stratified squamous epithelium
- Wound contraction (in open wounds) - myofibroblasts (fibroblasts expressing α-smooth muscle actin) contract the wound edges together, reducing wound size
Granulation tissue = capillary bed + fibroblasts + macrophages + loose collagen III + fibronectin + hyaluronic acid. Its presence signals active, healthy proliferation.
- Sabiston Textbook of Surgery | Schwartz's Principles of Surgery, 11th Ed.
Phase 4 - Maturation / Remodelling (Day 21 - 2 years)
Goal: Reorganise the collagen scaffold to maximise tensile strength; prune excess vessels and cells.
Key events:
- Type III collagen is replaced by type I collagen - fibrils become larger, cross-linked, and oriented along lines of tension
- Tensile strength increases progressively:
- Day 7: ~10% of original skin strength
- Day 21: ~30%
- Day 60: ~80%
- Maximum: ~80% of original strength is never fully recovered
- MMPs and TIMPs (tissue inhibitors of metalloproteinases) regulate this balance - MMPs degrade old collagen; TIMPs prevent excess degradation
- Excess capillaries regress - the wound becomes less red and less raised over time
- Myofibroblasts undergo apoptosis once contraction is complete
- The final scar is acellular, avascular, and less elastic than original skin
Abnormal remodelling:
-
Insufficient remodelling → dehiscence or chronic wound
-
Excessive collagen deposition → hypertrophic scar (within wound margins) or keloid (beyond wound margins)
-
Sabiston Textbook of Surgery | Schwartz's Principles of Surgery, 11th Ed.
Summary Table
| Phase | Timing | Key Cells | Key Molecules | Output |
|---|---|---|---|---|
| Haemostasis | Seconds - hours | Platelets, endothelium | vWF, thrombin, PDGF, TGF-β, fibrin | Platelet plug + fibrin clot |
| Inflammation | Days 1-4 | Neutrophils (peak d2), Macrophages (peak d3), Lymphocytes (peak d7) | IL-1, IL-6, TNF-α, ROS, NO, VEGF | Clean wound bed; cytokine gradient |
| Proliferation | Days 4-21 | Fibroblasts, endothelial cells, keratinocytes, myofibroblasts | PDGF, TGF-β, VEGF, FGF, EGF, collagen III | Granulation tissue, new vessels, epithelial cover |
| Remodelling | Day 21 - 2 years | Fibroblasts, myofibroblasts (apoptose) | MMPs, TIMPs, collagen I | Mature scar; 80% tensile strength |
This is a shared conversation. Sign in to Orris to start your own chat.