Hemorrhoids ttreatment
Reading File
Finding Sources
Searching PubMed
hemorrhoids treatment management
Searching the Web
hemorrhoids treatment guidelines 2025
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive, evidence-based guide to hemorrhoid treatment.
Hemorrhoids: Classification & Treatment
Anatomy & Classification
Hemorrhoids are normal cushions of vascular tissue in the anal canal. They become pathological when they enlarge, bleed, or prolapse. They are classified by location and, for internal hemorrhoids, by degree of prolapse:
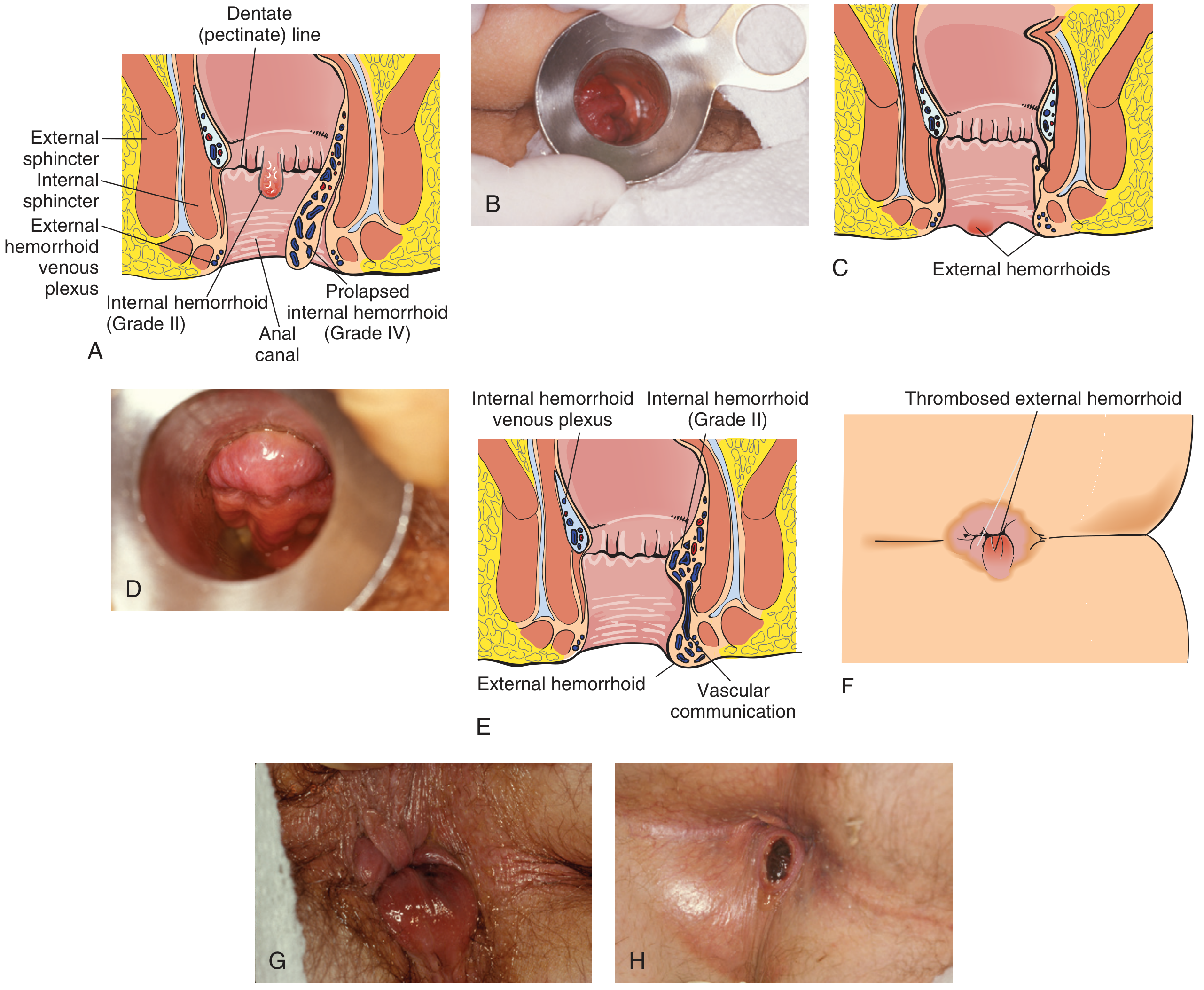
Internal Hemorrhoid Grading (above the dentate line - painless)
| Grade | Description |
|---|---|
| I | Bleed but do NOT prolapse |
| II | Prolapse on straining, reduce spontaneously |
| III | Prolapse, require manual reduction |
| IV | Irreducible prolapse (or acutely incarcerated) |
External Hemorrhoids (below the dentate line - painful)
- Present with acute onset of pain and swelling
- Pain peaks in the first 48 hours then gradually subsides
- Can thrombose, forming a firm, tender perianal lump
Step-by-Step Treatment Approach
1. Conservative (First-Line for All Grades)
Per the ASCRS 2024 guidelines and multiple textbooks, dietary and behavioral modifications are the primary first-line therapies:
- Dietary fiber - 25-35 g/day (psyllium, methylcellulose); reduces persistent symptoms by up to 53%
- Adequate fluid intake - 6-8 glasses of water per day
- Avoid straining and prolonged sitting on the toilet
- Sitz baths - warm water soaks for 10-15 minutes, 2-3x/day for comfort
- Stool softeners (docusate) if needed
- Topical agents - hydrocortisone creams, lidocaine, or witch hazel for symptom relief (itching, pain); do not resolve the underlying hemorrhoid
Indication: All grades; sufficient alone for mild Grade I-II.
2. Office-Based Procedures (Grade I-III)
The ASCRS gives a strong recommendation for office-based procedures for Grade I-II and selected Grade III hemorrhoids refractory to conservative therapy. These are performed for internal hemorrhoids only.
a) Rubber Band Ligation (RBL) - Most Effective Office Procedure
- A ligating device is passed through an anoscope; hemorrhoid tissue is drawn into the cylinder and two rubber bands are released at its base
- Causes ischemic necrosis; tissue sloughs over several days
- Effective in >80% of Grade I-III internal hemorrhoids
- Can band only one site per visit to reduce risk
- Complications: pain, bleeding (up to 1-2 weeks post-procedure), rare pelvic sepsis
b) Sclerotherapy
- Injection of 1-5 mL of 5% phenol in oil (most common) or hypertonic saline into the submucosa at the apex of the hemorrhoid column via anoscope
- Do NOT inject directly into the hemorrhoid - risk of thrombosis
- Best for Grade I-II hemorrhoids, or those too small to band
- More complications than RBL long-term
c) Infrared Coagulation (IRC)
- Infrared light applied 3-5 times at the hemorrhoid base through anoscope (1.5 sec each burst)
- Effective for Grade I-II internal hemorrhoids
- As effective as sclerotherapy; may need multiple sessions
- Advantages: minimal pain, fast recovery
d) Hemorrhoid Artery Ligation (HAL) / Doppler-Guided HAL + Mucopexy
- Uses Doppler to identify and ligate terminal hemorrhoidal arteries
- Can be combined with mucopexy (plication of prolapsing tissue)
- Effective for Grade II-III; less postoperative pain than hemorrhoidectomy
3. Surgical Treatment (Grade III-IV or Failed Office Procedures)
a) Excisional Hemorrhoidectomy - Gold Standard
- Most definitive treatment; performed as outpatient under MAC + local or spinal anesthesia
- Patient placed in prone jack-knife position
- Hemorrhoidal tissue dissected off the internal anal sphincter; wound may be left open or closed with absorbable suture
- Must leave ≥2 cm of normal anoderm between excision sites to prevent anal stenosis
- Must preserve the internal anal sphincter
- Post-op: multimodal analgesia (acetaminophen + NSAIDs + minimal opioids ± gabapentin); limit IV fluids to <700 mL to reduce urinary retention (~15% incidence)
- Limitation: significant postoperative pain
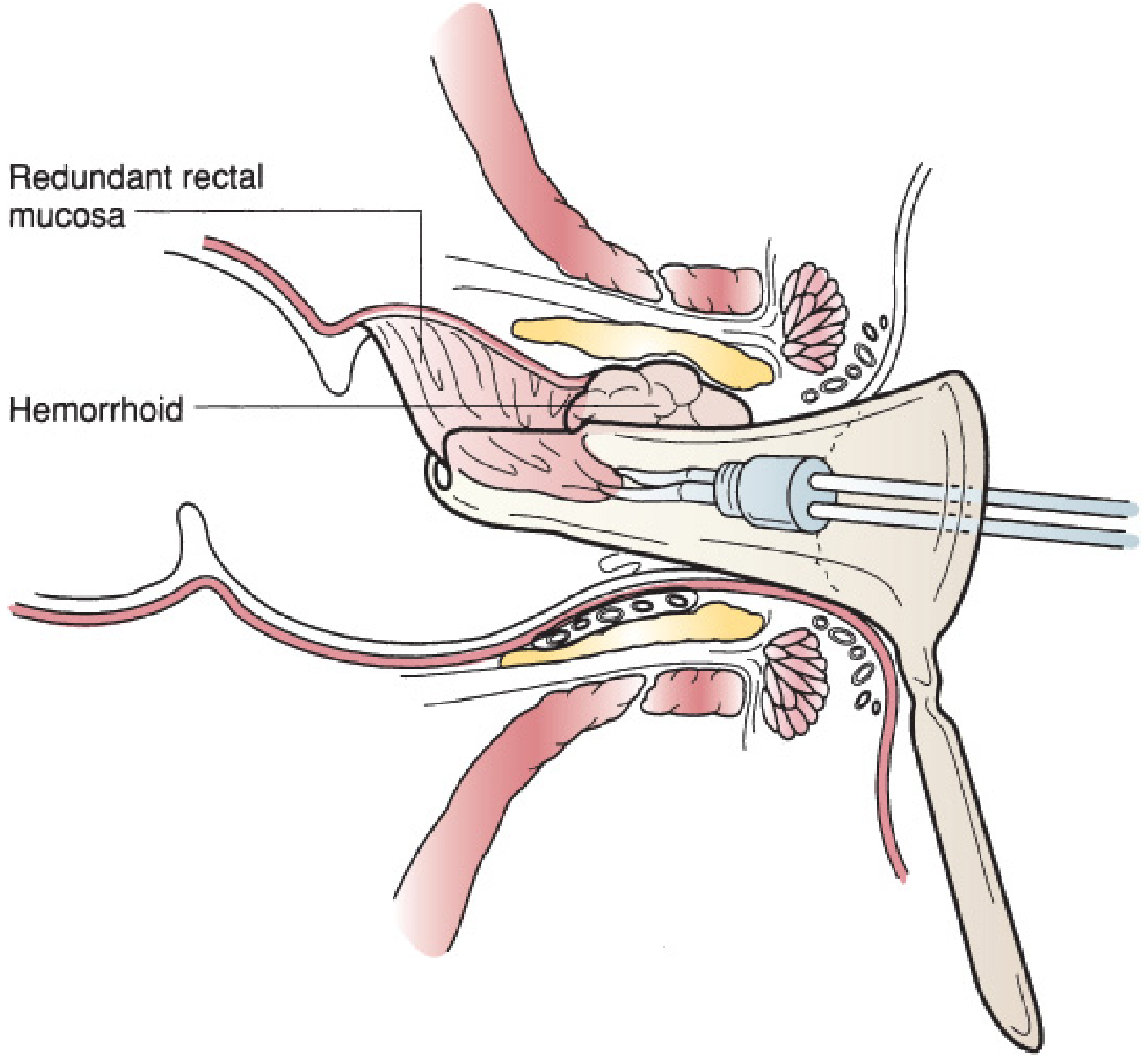
b) Stapled Hemorrhoidopexy (PPH - Procedure for Prolapse and Hemorrhoids)
- Excises a circumferential sleeve of mucosa/submucosa, interrupting hemorrhoidal vessels and pulling up prolapsed tissue
- Less postoperative pain than excisional hemorrhoidectomy
- Enthusiasm has waned due to rare but severe complications: rectovaginal fistula, chronic debilitating pain, pelvic sepsis
- Long-term recurrence rates similar to excisional hemorrhoidectomy
4. Special Situations
Thrombosed External Hemorrhoids
- If patient presents within 48-72 hours of onset, early surgical excision is beneficial (pain relief is dramatic)
- After 72 hours, pain is usually subsiding - conservative management preferred (sitz baths, stool softeners, topical agents)
- Excision: elliptical incision under local anesthesia, clot removed, wound usually left open
Hemorrhoids in Pregnancy
- Conservative management is mainstay (fiber, fluids, sitz baths, topical agents)
- Office procedures can be considered in refractory cases; surgery deferred until postpartum if possible
- Many hemorrhoids regress after delivery
Anticoagulated Patients
- Monitor closely - hemorrhoidal bleeding rarely leads to anemia but is of increased concern
- Office procedures can be used cautiously; post-banding bleeding risk is higher
Treatment Algorithm Summary
Symptomatic Hemorrhoids
|
↓
Conservative (all grades): fiber, fluids, sitz baths, topical agents
|
├── Grade I-II (+ selected III): Office procedures
│ → RBL (most effective) > IRC > Sclerotherapy > HAL
|
└── Grade III-IV or failed office Rx: Surgery
→ Excisional hemorrhoidectomy (gold standard)
→ Stapled hemorrhoidopexy (selected cases, with caution)
Special: Thrombosed external hemorrhoid <72h → Excision
Recent Evidence (2025)
A 2025 meta-analysis (PMID: 40596934) comparing surgical vs. conservative treatments confirmed surgical approaches achieve superior complete remission rates, while conservative management carries lower complication risk - consistent with a stepwise approach.
Sources: Mulholland & Greenfield's Surgery 7e; Textbook of Family Medicine 9e; Sleisenger & Fordtran's GI & Liver Disease; Pfenninger & Fowler's Procedures for Primary Care; ASCRS Clinical Practice Guidelines 2024.
Note: This is educational content. Clinical decisions should be individualized based on patient grade, symptoms, comorbidities, and preference.
This is a shared conversation. Sign in to Orris to start your own chat.