Dobutamine in low flow gradient AS
Reading File
Finding Sources
Finding Sources
Searching PubMed
"low flow low gradient" "aortic stenosis" AND dobutamine
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
I now have all the information needed for a comprehensive, well-structured answer. Let me compile it.
Dobutamine Stress Echocardiography in Low-Flow, Low-Gradient Aortic Stenosis
Background: Why This Is a Problem
Aortic stenosis severity is assessed by valve area (AVA), mean gradient, and peak jet velocity. The classic "high-gradient" pattern (AVA <1.0 cm², mean gradient ≥40 mmHg, Vmax ≥4 m/s) is straightforward. The diagnostic challenge arises when AVA is <1.0 cm² but the gradient is low (<40 mmHg) - the low-flow, low-gradient (LFLG) pattern.
Classification of LFLG AS (AHA/ACC staging):
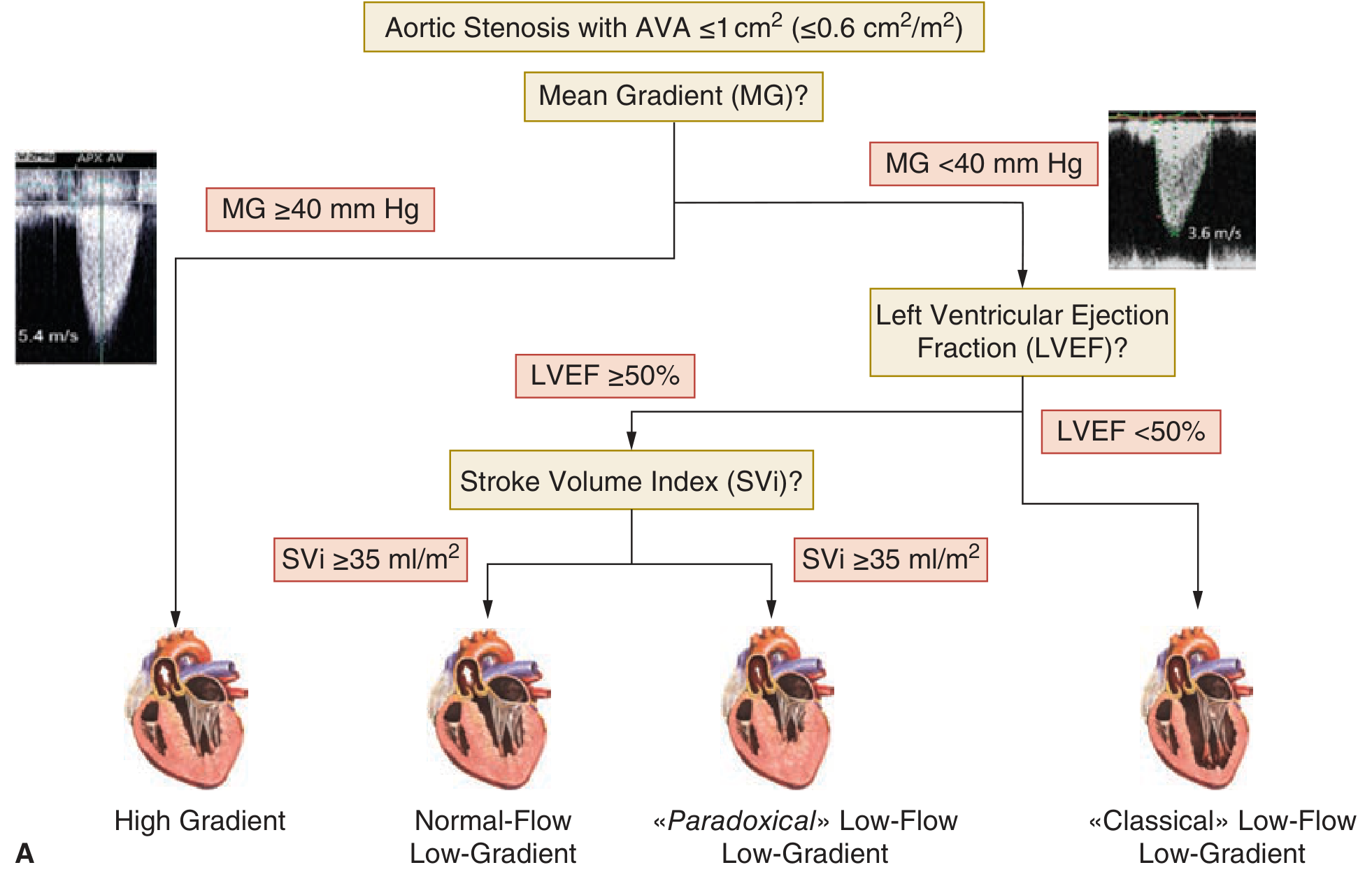
| Stage | Name | LVEF | Stroke Volume Index | Key Feature |
|---|---|---|---|---|
| D1 | High-gradient severe AS | Any | Normal | Mean gradient ≥40 mmHg |
| D2 | Classic LFLG | <50% | <35 mL/m² | Reduced LVEF, low flow |
| D3 | Paradoxical LFLG | ≥50% | <35 mL/m² | Normal LVEF, small hypertrophied LV |
| - | Normal-flow, LG | ≥50% | ≥35 mL/m² | Discordant grading |
The Core Diagnostic Dilemma
In Stage D2 (reduced LVEF), the low gradient could mean either:
- True severe AS - stiff, heavily calcified leaflets cannot open further regardless of flow; the LV is failing because of the severe obstruction
- Pseudosevere AS - the valve is only mildly/moderately stenotic, but low cardiac output from primary cardiomyopathy limits flow through the valve, making a relatively normal valve appear "stenotic"
This distinction is critical because AVR will help in true severe AS but may not benefit (and carries procedural risk) in pseudosevere AS. - Textbook of Clinical Echocardiography
Mechanism of Dobutamine in This Setting
Dobutamine is a beta-1 adrenergic agonist that:
- Increases myocardial contractility (positive inotropy)
- Increases heart rate (chronotropy)
- Increases cardiac output and transvalvular flow rate
By transiently augmenting flow across the aortic valve, dobutamine unmasks the valve's true hemodynamic behavior.
Protocol: Low-Dose Dobutamine Stress Echo (DSE)
- Performed under direct physician supervision
- Starting dose: 2.5-5 μg/kg/min, titrated upward
- Maximum dose: 20 μg/kg/min (low-dose protocol - much lower than standard ischemia testing)
- Measurements at each stage: aortic jet velocity, mean gradient, LVOT VTI, continuity equation AVA
- Endpoint: achieve ≥20% increase in stroke volume OR reach 20 μg/kg/min
Interpreting DSE Results
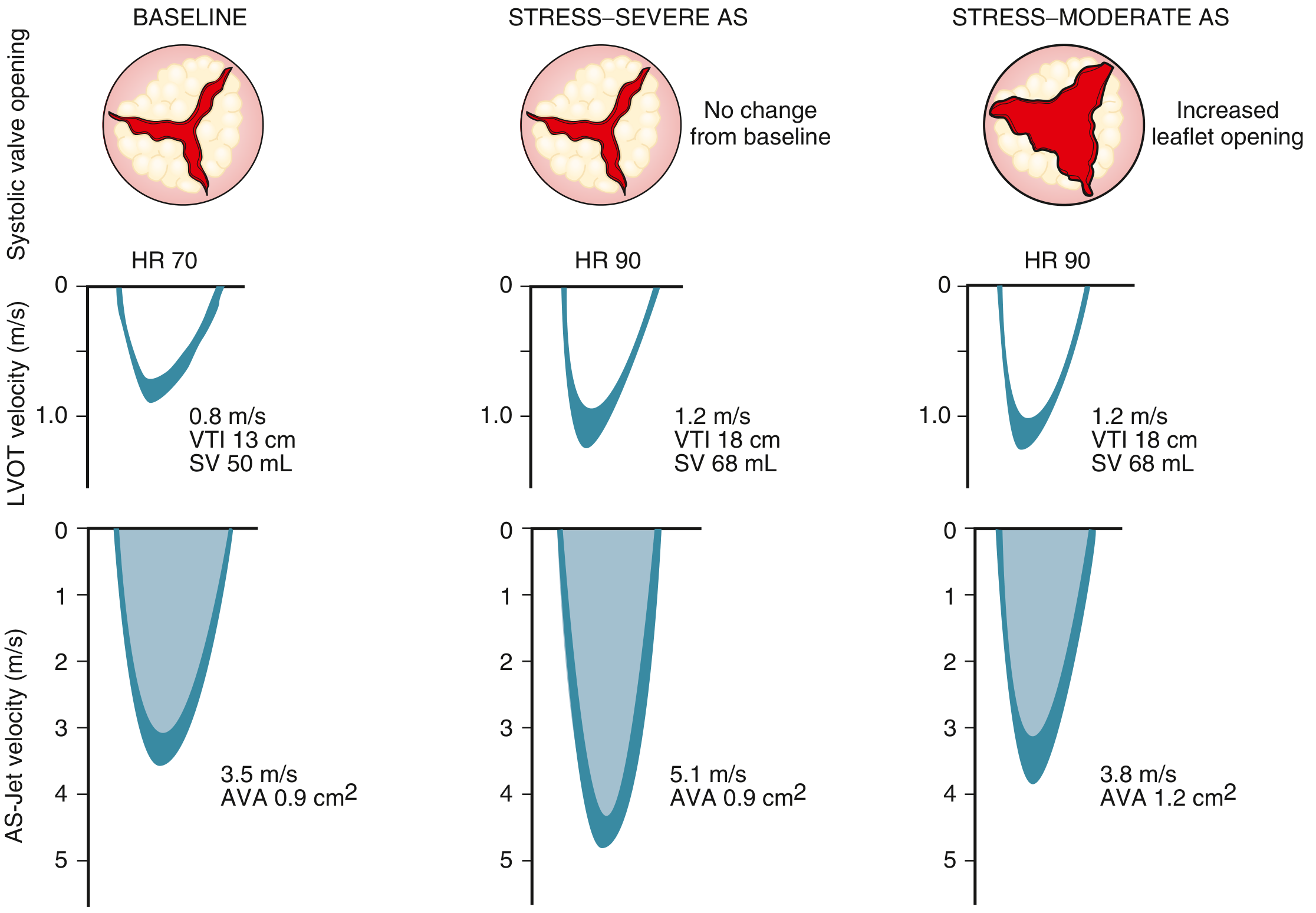
True Severe AS (Stage D2 confirmed):
- As flow rate increases with dobutamine, the valve area remains fixed (<1.0 cm²) because the stiff leaflets cannot open further
- The aortic jet velocity and mean gradient rise markedly
- Criteria: Vmax ≥4.0 m/s or mean gradient ≥40 mmHg at any flow rate, with AVA still <1.0 cm²
- → AVR/TAVR is indicated
Pseudosevere AS:
- As flow increases, the leaflets open more (they were just underloaded, not truly fixed)
- AVA increases (e.g., from 0.9 to 1.2+ cm²)
- Gradient increases modestly; velocity stays <4 m/s
- → AS is not truly severe; manage underlying cardiomyopathy first
Contractile Reserve
A key secondary assessment from DSE:
- Contractile reserve present: Stroke volume or LVEF increases by ≥20% from baseline
- Contractile reserve absent: Failure to augment flow/EF - this is a poor prognostic sign
However, importantly - even patients without contractile reserve who undergo AVR/SAVR still have better survival (~50% at 5 years) than those treated medically. More recent TAVR data show equivalent LVEF improvement and survival in patients with and without contractile reserve. - Braunwald's Heart Disease
Stage D3 (Paradoxical Low-Flow, Normal EF): Special Considerations
- DSE is generally not recommended in this group
- Rationale: the LV is small, hypertrophied, with marked diastolic dysfunction - there is very limited ability to augment stroke volume with dobutamine
- Preferred alternative: CT calcium scoring of the aortic valve (AVC) - a calcium score ≥2000 AU (men) or ≥1200 AU (women) supports truly severe AS
- Also: normalize blood pressure first and reassess gradients
Summary Decision Framework
Low AVA (<1 cm²) + Low Gradient (<40 mmHg)
↓
LVEF < 50%?
/ \
Yes (D2) No (D3)
↓ ↓
DSE (low-dose CT calcium score
dobutamine) preferred
↓
True AS? → Yes: Vmax ≥4 m/s at any flow + AVA fixed
→ No: AVA increases with flow (pseudosevere)
↓
Assess contractile reserve (ΔSV or ΔLVEF ≥20%)
Key Numbers to Remember
| Parameter | Value |
|---|---|
| Max dobutamine dose | 20 μg/kg/min |
| Criteria for true severe AS on DSE | Vmax ≥4 m/s AND AVA <1 cm² at any flow |
| Contractile reserve threshold | ≥20% increase in SV or EF |
| Stage D2 definition | AVA <1 cm², mean gradient <40 mmHg, LVEF <50% |
| Stage D3 definition | AVA <1 cm², mean gradient <40 mmHg, LVEF ≥50%, SVi <35 mL/m² |
Sources: Textbook of Clinical Echocardiography, p. 344-345 | Braunwald's Heart Disease, p. 709 | Harrison's Principles of Internal Medicine 22E, p. 1934
Recent reviews confirm this framework remains current: Stress Echo in Valvular Heart Disease (Citro et al., 2022) and ABCDEG Stress Echo in AS (Ciampi et al., 2023) both endorse DSE for D2 AS while noting CT calcium scoring as a complementary tool especially in D3.
This is a shared conversation. Sign in to Orris to start your own chat.