Hernia like swelling in infant when crying
Reading File
Finding Sources
Finding Sources
Searching PubMed
"inguinal hernia" infant pediatric
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough clinical overview:
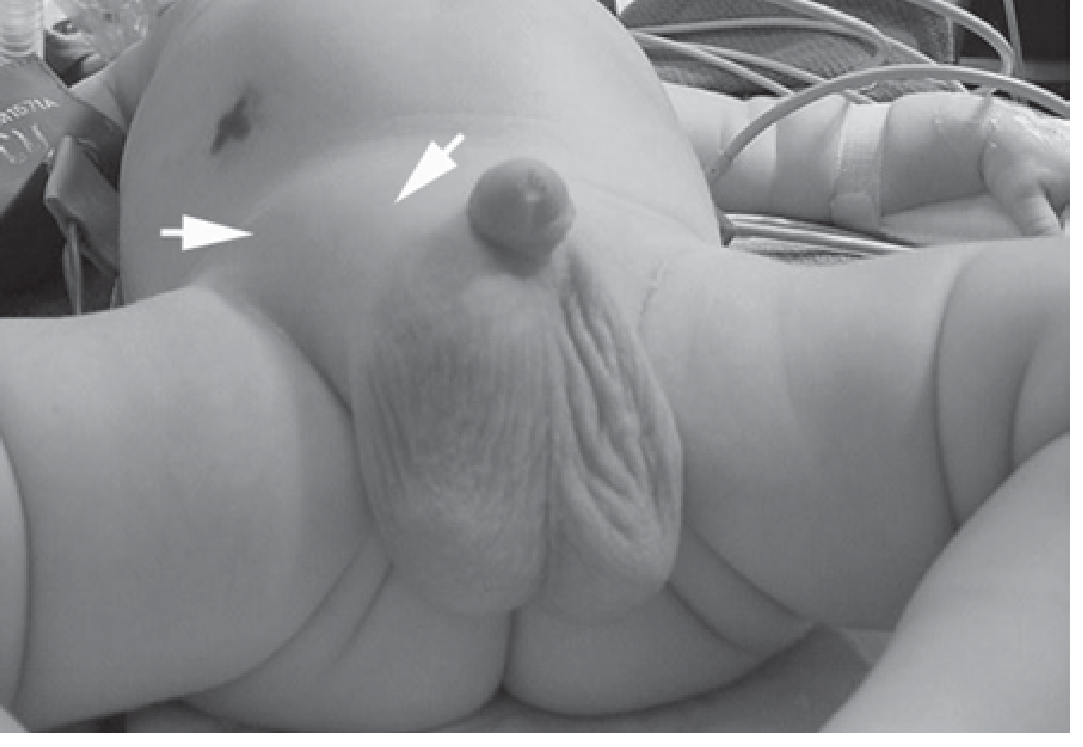
Hernia-Like Swelling in an Infant That Increases with Crying
The two most common causes are indirect inguinal hernia and umbilical hernia - both characteristically enlarge with crying due to increased intra-abdominal pressure.
1. Indirect Inguinal Hernia
Pathophysiology
All congenital hernias in children are indirect inguinal hernias by definition. They result from failure of closure of the processus vaginalis - a finger-like peritoneal projection that accompanies the testis during its descent into the scrotum. Closure normally occurs a few months before birth, which explains the very high incidence in premature infants. When the processus vaginalis remains completely patent, a communication persists between the peritoneal cavity and the groin.
Parents commonly believe the hernia was caused by crying or their child's activity level - this is a misconception; the underlying defect is congenital.
Key Features
- Sex ratio: Males >> females (10:1)
- Side: More common on the right
- Presentation: A groin bulge noticed during diaper changes; increases in size with crying, straining, or coughing and may disappear at rest
- On exam: the spermatic cord on the affected side feels thicker; pressure on the lower abdomen can reproduce the bulge
Complications - Incarceration and Strangulation
Infants are at high risk for incarceration because the inguinal ring is narrow. Signs of incarceration:
- Firm, non-reducing bulge in the groin
- Fussiness and irritability
- Progresses to: intestinal obstruction, peritonitis, systemic toxicity
If incarceration is present without overlying erythema or peritonitis, attempt manual reduction - place the infant in Trendelenburg + frog-leg position, administer an opioid for analgesia, then apply gentle pressure from below in the direction of the internal inguinal ring.
If reduction fails, or strangulation is present, emergency surgery is needed (may require laparotomy and bowel resection).
Treatment
- Every inguinal hernia in a child is an indication for surgical repair - spontaneous resolution does not occur.
- In neonates and infants: laparoscopic-assisted ligation of the internal inguinal ring (now favored by many pediatric surgeons) OR open high ligation of the hernia sac.
- Mesh is rarely needed before adolescence (no direct/femoral hernias in young children, and mesh does not grow with the child).
- Premature infants under 60 weeks corrected gestational age: overnight apnea monitoring required after repair under general anesthesia.
2. Umbilical Hernia
Key Features
- Occurs in up to 10% of infants, higher in premature babies and black infants (up to 8x higher incidence)
- Appears within a few weeks of birth; usually symptomless
- Increases in size on crying and assumes a classic conical shape
- Sexes equally affected
- Obstruction/strangulation is extremely uncommon below age 3 years
Treatment
- Conservative management under age 2 if symptomless - 95% resolve spontaneously - reassure parents
- Surgical repair if hernia persists beyond age 2 years
- Surgery: curved incision below the umbilicus, define the neck of the sac, reduce contents, close the defect in the linea alba with interrupted absorbable sutures
Quick Differential Summary
| Feature | Inguinal Hernia | Umbilical Hernia |
|---|---|---|
| Location | Groin / scrotum / labia | Umbilicus |
| Incarceration risk | High (especially infants) | Very low (<3 yrs) |
| Spontaneous resolution | No | Yes (95% by age 2) |
| Treatment | Always surgery | Watch-and-wait; surgery if persists >2 yrs |
| Male predominance | Yes (10:1) | No (equal) |
When to Seek Emergency Care
Take the infant to emergency immediately if:
- The swelling is hard, tender, or does not reduce when the infant relaxes
- Overlying skin redness or discoloration
- Infant is inconsolably crying, vomiting, or lethargic
- Signs of bowel obstruction (abdominal distension, bilious vomiting)
These signs suggest incarcerated or strangulated hernia, which is a surgical emergency.
Sources: Schwartz's Principles of Surgery 11th Ed.; Current Surgical Therapy 14th Ed.; Bailey and Love's Short Practice of Surgery 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.