Explain capillary exchange.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
I now have comprehensive content from multiple authoritative sources. Here is the full explanation:
Capillary Exchange
Capillary exchange refers to the movement of gases, solutes, and fluid between the blood inside capillaries and the surrounding interstitial fluid. It is the fundamental process by which tissues receive nutrients and O2 and dispose of metabolic waste. Two broad mechanisms operate: diffusion (for gases and small solutes) and convection/osmosis (for bulk fluid movement, governed by Starling forces).
1. Structure of the Capillary Wall
Capillaries are the thinnest vessels in the body - a single layer of endothelial cells with water-filled clefts (interendothelial junctions) between them. This thin wall is critical to exchange:
-
Lipid-soluble substances (O2, CO2, steroid hormones) cross directly through endothelial cell membranes by simple diffusion.
-
Water-soluble, lipid-insoluble substances (glucose, ions, amino acids, water) can only pass through the aqueous clefts between endothelial cells, so they have far less available surface area.
-
Proteins (e.g., albumin) are generally too large to cross via clefts; they are retained in the vascular compartment. Tiny amounts leak via pinocytotic vesicles (transcytosis). In fenestrated capillaries (kidney, intestine), slightly more protein can escape.
-
Costanzo Physiology, p. 176
2. Exchange of Gases and Small Solutes (Diffusion)
Gases: O2 and CO2
O2 and CO2 are highly lipid-soluble and diffuse freely through the endothelial cell membrane by transcellular diffusion. The driving force is the partial pressure gradient. In systemic capillaries, O2 diffuses out into tissues; CO2 diffuses in the opposite direction.
The Krogh tissue cylinder model describes this: each capillary is surrounded by a concentric cylinder of tissue it supplies. The PO2 within the capillary falls along its length as O2 exits, determined by:
- Arterial PO2 feeding the capillary
- O2 content of blood (bound to hemoglobin + dissolved)
- Capillary blood flow
- Radial diffusion coefficient (Dx)
- Capillary and tissue cylinder radii
- O2 consumption by the tissue (QO2)
At rest, only ~20% of skeletal muscle capillaries are perfused. During exercise, precapillary sphincters and arterioles dilate, increasing both blood flow and the number of open capillaries - reducing the Krogh cylinder radius and shortening diffusion distances.
- Medical Physiology, p. 678
Small Water-Soluble Solutes (Fick's Law)
For hydrophilic solutes (glucose, electrolytes, urea), diffusion is paracellular - through clefts and fenestrae. The governing equation is:
Q̇ = S · Px · ([X]c - [X]if)
Where:
- Q̇ = mass flow (moles/s)
- S = functional capillary surface area (cm²)
- Px = permeability coefficient (Dx/a, where Dx is diffusion coefficient and a is wall thickness) - "expresses the ease with which the solute crosses a capillary by diffusion"
- [X]c and [X]if = solute concentrations in capillary and interstitial fluid
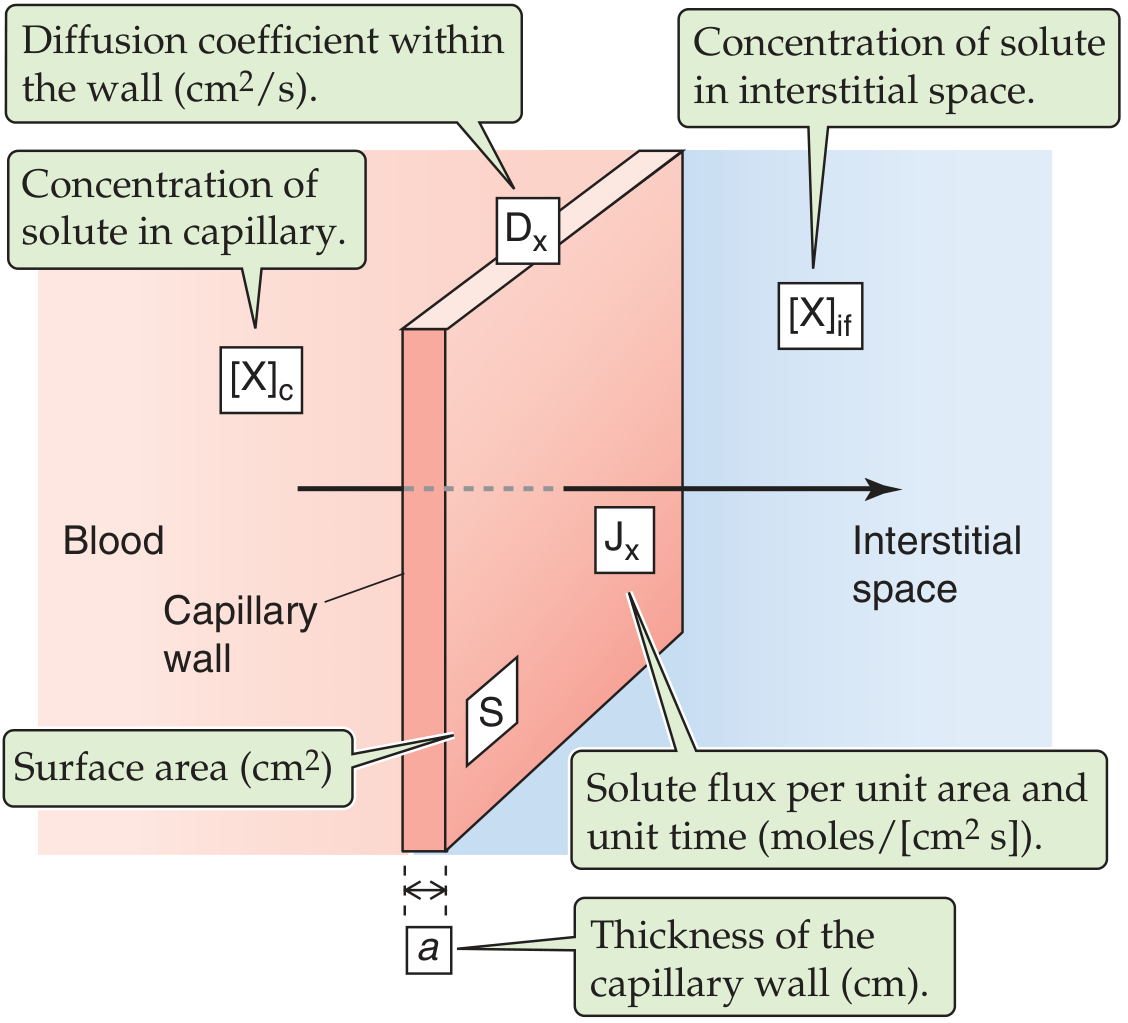
Figure: Diffusion of a solute across the capillary wall (Medical Physiology, Fig. 20-5)
- Medical Physiology, p. 679
3. Fluid Exchange: The Starling Forces
The most important mechanism for bulk fluid transfer across the capillary wall is convection driven by hydrostatic and colloid osmotic (oncotic) pressures - collectively called the Starling forces. First described by Ernest Starling in 1896.
The Four Starling Pressures
| Pressure | Location | Effect on Fluid |
|---|---|---|
| Capillary hydrostatic pressure (Pc) | Inside capillary | Pushes fluid out |
| Interstitial fluid hydrostatic pressure (Pif) | Outside capillary | Usually slightly negative; assists filtration outward |
| Plasma colloid osmotic pressure (πc) | Inside capillary (from plasma proteins) | Pulls fluid in |
| Interstitial colloid osmotic pressure (πif) | Outside capillary (from interstitial proteins) | Pulls fluid out |
Only protein contributes meaningfully to colloid osmotic pressure at the capillary wall because it is the only solute with a reflection coefficient ≈ 1.0 (i.e., it cannot cross the membrane and thus exerts its full osmotic pressure). This is called oncotic pressure.
- Costanzo Physiology, p. 176
The Starling Equation
$$J_V = L_P \left[ (P_c - P_{if}) - \sigma(\pi_c - \pi_{if}) \right]$$
Where:
-
Jv = volume flux across the capillary wall (cm³/cm²/s)
-
Lp = hydraulic conductivity of the wall
-
σ = reflection coefficient for proteins (0 to 1; ≈1 for most capillaries)
-
Positive Jv = net filtration (outward); negative Jv = net absorption (inward)
-
Medical Physiology, p. 685-687
4. Forces at the Arterial vs. Venous End
Capillary hydrostatic pressure (Pc) is much higher at the arterial end (~30 mm Hg) than the venous end (~10 mm Hg), while plasma oncotic pressure (~28 mm Hg) remains nearly constant throughout. This produces a net shift in the balance of forces:
Arterial End - Net Filtration
| Force | mm Hg | Direction |
|---|---|---|
| Capillary hydrostatic pressure | 30 | Outward |
| Negative interstitial hydrostatic pressure | 3 | Outward |
| Interstitial colloid osmotic pressure | 8 | Outward |
| Total Outward | 41 | |
| Plasma colloid osmotic pressure | 28 | Inward |
| Total Inward | 28 | |
| Net Outward (filtration pressure) | +13 | Filtration |
Venous End - Net Reabsorption
| Force | mm Hg | Direction |
|---|---|---|
| Capillary hydrostatic pressure | 10 | Outward |
| Negative interstitial hydrostatic pressure | 3 | Outward |
| Interstitial colloid osmotic pressure | 8 | Outward |
| Total Outward | 21 | |
| Plasma colloid osmotic pressure | 28 | Inward |
| Total Inward | 28 | |
| Net Inward (reabsorption pressure) | -7 | Reabsorption |
- Guyton & Hall Medical Physiology, p. 204
5. The Starling Equilibrium
Averaging forces over the entire capillary length gives a mean capillary pressure of ~17.3 mm Hg:
| Mean Force | mm Hg |
|---|---|
| Mean capillary pressure | 17.3 |
| Negative interstitial hydrostatic pressure | 3.0 |
| Interstitial colloid osmotic pressure | 8.0 |
| Total Outward | 28.3 |
| Plasma colloid osmotic pressure | 28.0 |
| Net Outward (mean) | 0.3 |
This net filtration of 0.3 mm Hg means slightly more fluid filters into the interstitial space than is reabsorbed. About 90% of filtered fluid is reabsorbed at the venous end of capillaries; the remaining 10% (~2 mL/min whole body) is returned to circulation via the lymphatics. This is a near-equilibrium state, not a perfect balance.
- Guyton & Hall Medical Physiology, p. 204-205
6. Capillary Filtration Coefficient (Kf)
The filtration coefficient (Kf) quantifies the ease of fluid filtration:
Net filtration rate = Kf × Net filtration pressure
For the whole body, Kf ≈ 6.67 mL/min per mm Hg. Expressed per tissue mass, it is ~0.01 mL/min/mm Hg/100 g, but varies >100-fold across different organs depending on capillary permeability and surface area (e.g., renal capillaries are far more permeable than muscle capillaries).
- Guyton & Hall Medical Physiology, p. 205
7. Routes Across the Capillary Wall
| Route | Substances | Mechanism |
|---|---|---|
| Through endothelial cells (transcellular) | O2, CO2, lipid-soluble molecules, water (via AQP1) | Simple diffusion; aquaporin 1 |
| Between endothelial cells (paracellular, clefts) | Water, ions, glucose, small solutes | Diffusion (concentration gradient), osmosis |
| Fenestrae | Limited protein (kidney, intestine) | Bulk flow |
| Transcytosis (vesicles) | Small amounts of macromolecules | Pinocytosis / exocytosis |
In the brain, clefts are especially "tight," restricting solute passage (the blood-brain barrier). In the kidney and intestine, fenestrated capillaries permit greater permeability.
- Costanzo Physiology, p. 176
8. Clinical Relevance
Disruption of any Starling force leads to edema (excess fluid in the interstitium):
| Cause | Mechanism | Example |
|---|---|---|
| Increased Pc | Elevated hydrostatic pressure → more filtration | Heart failure, venous obstruction |
| Decreased πc | Less oncotic pull → more filtration | Hypoalbuminemia (liver failure, nephrotic syndrome, malnutrition) |
| Increased capillary permeability | Proteins leak out → πif rises, πc falls | Sepsis, burns, anaphylaxis |
| Lymphatic obstruction | Filtrate not returned | Filariasis, post-mastectomy |
In hemorrhage, compensatory Starling changes favor reabsorption into capillaries: sympathetic arteriolar constriction lowers Pc, causing fluid to shift from interstitium back into the circulation.
- Medical Physiology, p. 243; Guyton & Hall Medical Physiology, p. 205
What do you mean by Starling forces?
The Starling forces are the four pressures that determine whether fluid moves out of or into a capillary:
- Capillary hydrostatic pressure (Pc) - the blood pressure inside the capillary, pushes fluid outward into the interstitium.
- Interstitial fluid hydrostatic pressure (Pif) - the pressure of fluid in the tissue space; normally slightly negative, so it also draws fluid outward.
- Plasma colloid osmotic pressure (πc) - also called oncotic pressure; generated by plasma proteins (mainly albumin) that cannot cross the capillary wall, pulls fluid inward.
- Interstitial colloid osmotic pressure (πif) - generated by the small amount of protein that leaks into the interstitium, pulls fluid outward.
The net filtration pressure is simply the sum:
NFP = (Pc + Pif + πif) - πc
When NFP is positive, fluid filters out (as at the arterial end). When negative, fluid is reabsorbed (as at the venous end).
The key insight Ernest Starling provided is that only proteins contribute meaningfully to osmotic pressure at the capillary wall - because small solutes like Na⁺, glucose, and Cl⁻ pass freely through the clefts and quickly equilibrate on both sides, so they exert no net osmotic effect. Proteins, by contrast, cannot cross (reflection coefficient ≈ 1), so they retain their full osmotic pulling power. That is why the relevant osmotic pressure is called colloid osmotic pressure (or oncotic pressure) - referring specifically to colloids (large molecules like proteins), not small solutes.
In short: hydrostatic pressures act like a pump pushing fluid out, while oncotic pressure acts like a sponge pulling fluid in. The balance between them determines the direction and rate of fluid movement across every capillary in the body.
This is a shared conversation. Sign in to Orris to start your own chat.