What is hospital acquired infection, what are the causes, Retention and management of ventilator associated pneumonia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ventilator-associated pneumonia" management prevention
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Hospital-Acquired Infection (Nosocomial Infection) and Ventilator-Associated Pneumonia
1. HOSPITAL-ACQUIRED INFECTION (HAI)
Definition
A hospital-acquired infection (HAI), also called a nosocomial infection, is an infection acquired during hospital care that was not present or incubating at the time of admission. Infections appearing more than 48 hours after admission are classified as nosocomial. They may be endemic (constant background level) or epidemic (outbreak above baseline).
"A high frequency of nosocomial infection is evidence of a poor quality of health service delivery." - Park's Textbook of Preventive and Social Medicine
HAIs are not limited to inpatients - infections in staff, visitors, and patients receiving outpatient care in a health care setting may also be considered nosocomial.
Causes / Sources of HAI
HAI can be analyzed from three angles: Sources, Routes of Spread, and Recipients.
A. Sources
| Source | Examples |
|---|---|
| Patients | Infectious diseases (measles, influenza, hepatitis), skin infections (infected wounds, boils, bed sores), respiratory infections (TB, chest infections), UTIs |
| Hospital Staff | Doctors, nurses, ward staff - carry S. aureus in the nose/skin, haemolytic streptococci in the throat, salmonella in the gut |
| Environment | Hospital dust, linen, bedclothes, furniture, sinks, basins, door handles, and air - all laden with microorganisms |
B. Routes of Spread
- Direct contact - organisms transferred directly from the hands of nurses/doctors to a susceptible patient
- Droplet infection - droplets released from the nose and throat via coughing or sneezing
- Airborne particles
- Hospital dust released into the air during sweeping, dusting, or bed making
- Hospital procedures - catheterization, intravenous procedures, infected catgut, dressings, sputum cups, bedpans, urinals
C. Recipients (Susceptible Patients)
All hospitalized patients are potential recipients. High-risk groups include:
- Severely ill patients
- Immunocompromised individuals
- Patients on corticosteroid therapy
- Those in ICUs, urological wards, geriatric wards, and special baby care units
Most Common Sites of Nosocomial Infection
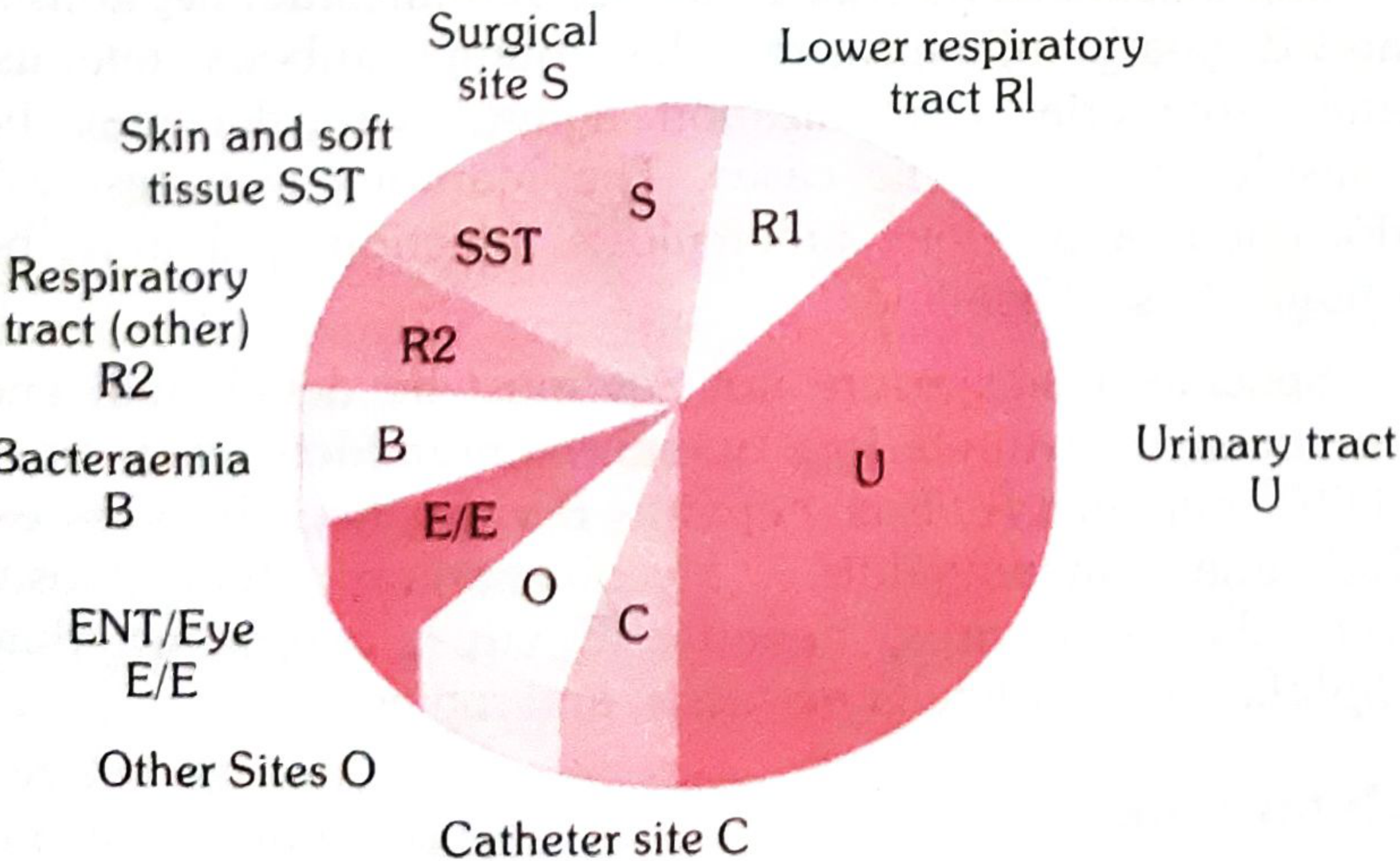
The four most common nosocomial infections are:
- Urinary tract infections (largest proportion - associated with urinary catheters)
- Surgical wound infections
- Pneumonia (lower respiratory tract)
- Primary bloodstream infections (catheter-related)
Each is associated with an invasive device or invasive procedure.
Simplified Diagnostic Criteria for Common HAIs
| Type | Simplified Criterion |
|---|---|
| Surgical site infection | Purulent discharge, abscess, or spreading cellulitis at surgical site within 1 month |
| Urinary infection | Positive urine culture (≥10⁵ bacteria/mL), with or without symptoms |
| Respiratory infection | Respiratory symptoms + ≥2 of: cough, purulent sputum, new chest X-ray infiltrate |
| Vascular catheter infection | Inflammation, lymphangitis, or purulent discharge at catheter insertion site |
| Septicaemia | Fever or rigors + at least one positive blood culture |
Prevention of HAI (General Measures)
| Measure | Details |
|---|---|
| Isolation | Isolate infectious patients; separate susceptible patients from source patients |
| Staff health | Staff with skin disease, sore throat, diarrhoea, etc. excluded from work until cured |
| Hand hygiene | Most important - thorough soap and water washing; alcohol-based disinfectant when needed. WHO 2009 "Clean Care is Safer Care" guidelines |
| Dust control | Wet dusting and vacuum cleaning; suppress dust during bed-making |
| Disinfection | Proper sterilization of instruments; disinfection of patient articles and bodily fluids |
| Droplet control | Face masks, adequate bed spacing, prevention of overcrowding, good ventilation |
| Barrier nursing | Minimize cross-infection through technique |
| Administration | Hospital Infection Control Committee to set policies on isolation, disinfection, and compliance |
| Standard precautions | Gloves for all contacts with secretions/body fluids; gown, mask, eye protection as needed |
(Park's Textbook of Preventive and Social Medicine)
2. VENTILATOR-ASSOCIATED PNEUMONIA (VAP)
Definition
VAP is defined as the new onset of a lower respiratory tract infection in a patient requiring mechanical ventilation for more than 48 hours after endotracheal intubation.
Epidemiology
- VAP occurs in up to 40% of intubated patients - it is the most frequent ventilator-associated complication and the most common ICU-acquired infection
- Peak incidence: 5 to 9 days after intubation; cumulative risk increases with duration of ventilation
- Overall mortality rate: 30%-70% (attributable mortality may be lower in recent data due to improved prevention)
- Compared to non-VAP patients: 2.4% vs 10.5% mortality in one landmark study
(Frameworks for Internal Medicine; Miller's Anesthesia; Barash's Clinical Anesthesia)
Classification: Early vs. Late-Onset VAP
| Feature | Early-Onset VAP | Late-Onset VAP |
|---|---|---|
| Timing | Within 48-72 hours of intubation | After 72 hours of intubation |
| Organisms | H. influenzae, S. pneumoniae, MSSA, sensitive oral flora | MRSA, Pseudomonas aeruginosa, Acinetobacter baumannii |
| Severity | Lower/zero attributable mortality | Higher mortality (especially Pseudomonas, Acinetobacter) |
Causative Organisms
| Organism | Frequency in US |
|---|---|
| Enteric gram-negative bacilli (with ESBL-producing strains) | Up to 40% |
| Staphylococcus aureus (main gram-positive pathogen) | Up to 30% |
| Pseudomonas aeruginosa (frequently MDR) | Up to 20% |
| Acinetobacter baumannii (MDR; may only respond to polymyxins) | Up to 10% |
Diagnostic Criteria
Clinical diagnosis requires a new chest X-ray infiltrate PLUS at least two of:
- Fever or temperature instability
- Elevated or low WBC count
- Purulent respiratory secretions / positive respiratory culture
Microbiological methods:
- Non-invasive (preferred): Endotracheal aspiration (quantitative culture ≥10⁵ CFU/mL), blood cultures (positive in ~15%)
- Invasive: Bronchoscopy with BAL (threshold ≥10⁴ CFU/mL) or protected brush specimens (≥10³ CFU/mL); VAP confirmed when bacteria are seen intracellularly in BAL cells
(IDSA guidelines prefer tracheal aspirate specimens as first-line; BAL reserved for selected cases)
Management of VAP
Step 1 - Start Empiric Antibiotics Promptly
Treatment must not be delayed pending full diagnostic workup. Send cultures first, then start antibiotics if clinical suspicion is high.
Step 2 - Empiric Antibiotic Selection
| VAP Type | Empiric Regimen |
|---|---|
| Early-onset (<72 hours) | Narrow-spectrum single agent - Ceftriaxone + Azithromycin; add vancomycin/linezolid if known MRSA history |
| Late-onset (>72 hours) | Broad-spectrum, 2-drug regimen covering MDR gram-negatives + MRSA: Vancomycin OR Linezolid + Cefepime ± ciprofloxacin if high MDR gram-negative risk |
When to Add MRSA Coverage
Add vancomycin or linezolid if any of:
- Prior IV antibiotics within 90 days
- Unit where >10-20% of S. aureus isolates are MRSA
- Unit where MRSA prevalence is unknown
- Known MRSA carrier
- Severely ill patient with high mortality risk
MDR Pathogen Risk Factors (Especially for Pseudomonas):
- Prior IV antibiotics within 90 days (strongest risk factor)
- Septic shock at time of VAP
- ARDS before VAP
- ≥5 days of hospitalization before VAP
- Acute renal replacement therapy before VAP
- History of underlying chronic lung disease (COPD, bronchiectasis)
Acinetobacter baumannii Treatment:
- Susceptible strains: carbapenem or ampicillin-sulbactam (first-line)
- Pan-resistant strains: polymyxins (polymyxin B or colistin), with inhaled colistin added for augmentation
Step 3 - De-escalation Therapy (48-72 hours)
After culture results return:
- Narrow antibiotic spectrum or discontinue entirely based on quantitative culture results
- Goal: ensure adequate initial treatment while avoiding long-term antibiotic overuse
- Antibiotic selection should always reflect local hospital resistance patterns
Prevention of VAP (VAP Bundle)
The IHI VAP Bundle (Institute for Healthcare Improvement, 2005) consists of evidence-based interventions implemented collectively. Bundle compliance has reduced VAP from 11.6 to 0.3 per 1000 ventilator days in some studies.
| Bundle Element | Details |
|---|---|
| Head-of-bed elevation | Maintain ≥30 degrees to reduce passive drainage of secretions into ETT |
| Oral hygiene | Chlorhexidine mouth rinse every 2-4 hours to reduce oral bacterial colonization |
| Subglottic suctioning | Suction oropharynx BEFORE suctioning ETT or deflating ETT cuff |
| Ventilator tubing drainage | Drain condensation every 2-4 hours and before repositioning; do NOT disconnect circuit |
| Inline suction catheters | Allows ETT suctioning without disconnecting the ventilator circuit |
| Hand hygiene | Strict handwashing between patients (simplest and cheapest intervention) |
| Minimize ventilation days | Daily sedation vacation and spontaneous breathing trials to enable extubation as soon as safe |
| Avoid unnecessary acid suppression | Acid suppression allows gastric bacterial overgrowth; reserve for high-risk patients only; consider sucralfate as alternative |
| Selective decontamination (SDD) | Non-absorbable antimicrobial agents to reduce gut/oropharyngeal colonization (controversial but growing evidence) |
| Specialized ETT | Subglottic suctioning port ETTs shown to reduce VAP and shorten ICU stay (meta-analysis supported) |
Summary: Prevention vs. Treatment
| Approach | Goal |
|---|---|
| VAP Bundle | Reduce incidence through infection control practices |
| Empiric antibiotics | Ensure adequate early coverage while awaiting cultures |
| De-escalation | Minimize antibiotic resistance and side effects once cultures are known |
| Invasive diagnostics | More accurate than clinical criteria alone; guides targeted therapy |
Sources: Park's Textbook of Preventive and Social Medicine | Frameworks for Internal Medicine | Barash, Cullen & Stoelting's Clinical Anesthesia, 9e | Miller's Anesthesia, 10e | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.