Anti hypertensive drugs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content. Let me compile the full, detailed answer:
Antihypertensive Drugs
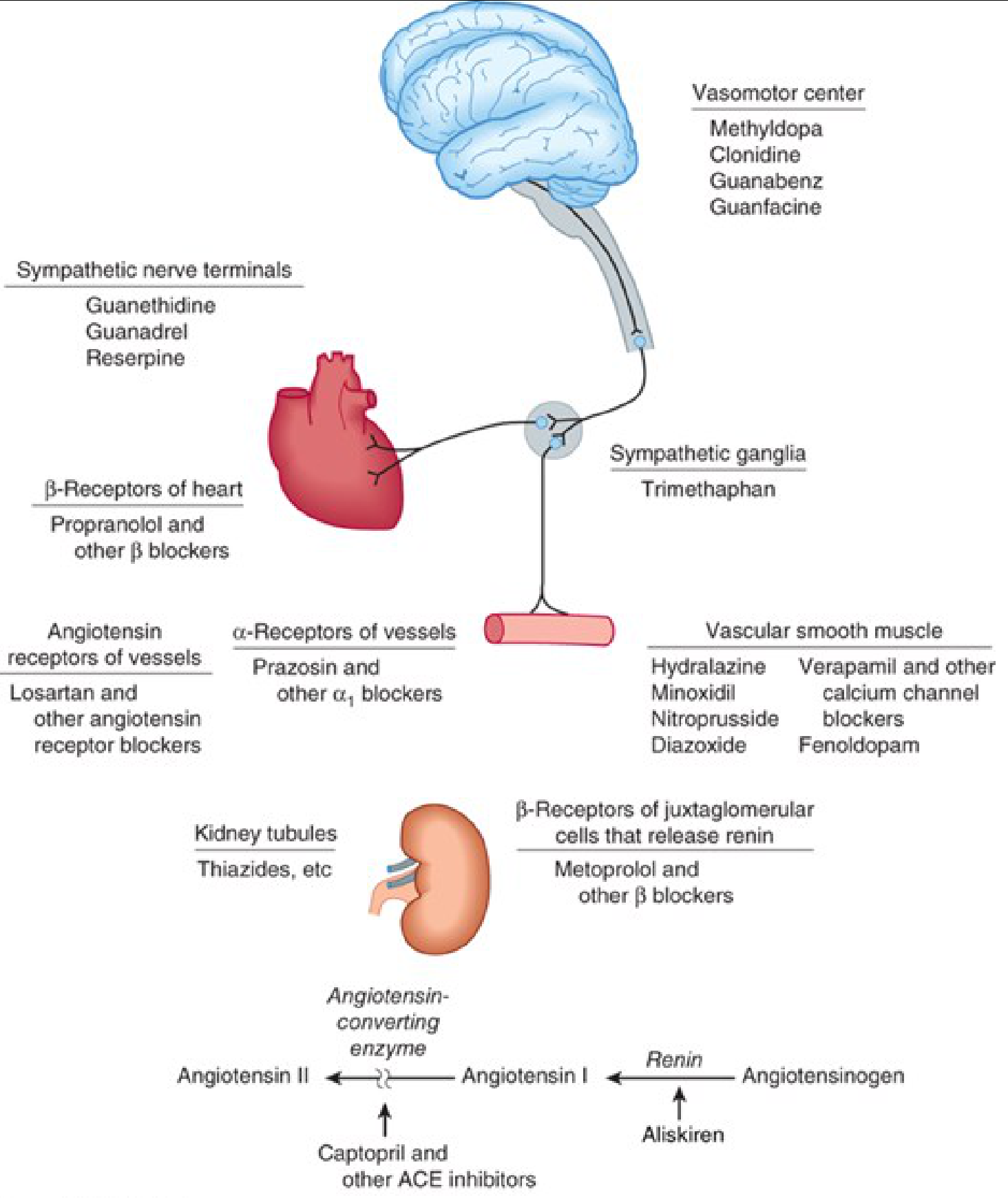
Figure: Sites of action of antihypertensive drugs across the cardiovascular and autonomic systems (Katzung's Basic and Clinical Pharmacology, 16th Ed.)
Overview & Classification
All antihypertensive agents act at one or more anatomic control sites and interfere with normal blood pressure regulation. They are classified by their principal site or mechanism of action into four broad groups:
- Diuretics - deplete sodium, reduce blood volume
- Renin-Angiotensin System (RAS) Blockers - reduce peripheral vascular resistance and blood volume
- Direct Vasodilators - relax vascular smooth muscle
- Sympathoplegic Agents - reduce PVR, inhibit cardiac function, increase venous pooling
1. Diuretics
Mechanism
Diuretics lower BP primarily by depleting body sodium. Initially, they reduce BP by decreasing blood volume and cardiac output. After 6-8 weeks, cardiac output returns toward normal while peripheral vascular resistance declines. Sodium is also thought to increase vessel stiffness and neural reactivity via altered sodium-calcium exchange.
Effective at lowering BP by 10-15 mmHg in most patients.
Types & Uses
| Type | Drugs | Use |
|---|---|---|
| Thiazides | Hydrochlorothiazide, Chlorthalidone | First-line in mild-moderate HTN with normal renal/cardiac function |
| Loop diuretics | Furosemide, Bumetanide, Torsemide | Severe HTN, renal insufficiency (GFR <30-40 mL/min), heart failure, cirrhosis |
| Potassium-sparing | Spironolactone, Eplerenone (MRAs) | Resistant HTN, heart failure |
- Chlorthalidone has a longer duration of action than HCTZ, though both show comparable cardiovascular outcomes in elderly patients.
- In severe hypertension on multiple drugs, blood pressure becomes very sensitive to volume because vascular responsiveness is blunted.
Adverse Effects
- Hypokalemia, hyperglycemia, hyperuricemia (thiazides) - particularly significant in elderly due to higher prevalence of arrhythmias, diabetes, and gout
- MRAs contraindicated if creatinine >2.5 mg/dL (men) or >2.0 mg/dL (women), or hyperkalemia
2. Renin-Angiotensin System (RAS) Blockers
A. ACE Inhibitors (ACEi)
Mechanism: Block conversion of Angiotensin I to Angiotensin II, reducing peripheral vascular resistance. No reflex sympathetic activation or tachycardia (due to baroreceptor resetting or enhanced parasympathetic tone). Also prevent bradykinin breakdown.
Key drugs:
- Captopril (prototype), Enalapril (prodrug → enalaprilat), Lisinopril (lysine derivative; not a prodrug), Ramipril, Perindopril, Benazepril, Fosinopril, Quinapril, Trandolapril
Special benefits:
- Reduce proteinuria and stabilize renal function in CKD and diabetes (by reducing efferent arteriolar resistance and intraglomerular capillary pressure)
- Beneficial in heart failure and post-MI
- Reduce incidence of new-onset diabetes in high cardiovascular risk patients
Adverse Effects:
- Dry cough (due to bradykinin/substance P accumulation) - class effect
- Angioedema - rare but serious
- Hyperkalemia (especially in renal insufficiency or diabetes)
- Acute renal failure in bilateral renal artery stenosis
- Contraindicated in pregnancy (2nd and 3rd trimesters - fetal hypotension, anuria, renal failure, malformations)
- First-dose hypotension in hypovolemic patients
B. Angiotensin Receptor Blockers (ARBs)
Mechanism: Block AT₁ receptors directly; do not inhibit bradykinin breakdown, so no cough - major advantage over ACEi.
Key drugs: Losartan, Valsartan, Irbesartan, Olmesartan, Candesartan, Telmisartan, Azilsartan
Contraindications (same as ACEi): Pregnancy, bilateral renal artery stenosis, hyperkalemia
C. Direct Renin Inhibitor
- Aliskiren - inhibits renin directly, blocking the first step of the RAS cascade. Generally used as add-on therapy; avoid combining with ACEi/ARBs especially in diabetes or renal disease.
3. Calcium Channel Blockers (CCBs)
Mechanism
Block voltage-gated L-type calcium channels in vascular smooth muscle and myocardium, causing relaxation and decreased peripheral resistance.
Classification
| Subclass | Drugs | Key Properties |
|---|---|---|
| Dihydropyridines (DHP) | Amlodipine, Nifedipine, Felodipine, Nicardipine | Primarily vascular; minimal cardiac effect; can cause reflex tachycardia |
| Non-DHPs (Phenylalkylamines) | Verapamil | Cardiac > vascular; negative inotrope, chronotrope; used for rate control in AF |
| Non-DHPs (Benzothiazepines) | Diltiazem | Intermediate cardiac/vascular effect; used in rate control |
Special uses:
- Effective in elderly and in isolated systolic hypertension
- DHPs especially useful in angina with atherosclerosis
- Non-DHPs (Verapamil, Diltiazem) for AF rate control
Contraindications:
- Verapamil/Diltiazem: AV block grade 2-3, severe LV dysfunction, heart failure
- DHPs: Use with caution in tachycardia/arrhythmia
4. Sympathoplegic (Adrenergic) Agents
A. Beta-Blockers (β-Blockers)
Mechanism: Block β₁-adrenergic receptors → decrease heart rate, cardiac output, and renin release from juxtaglomerular cells.
Key drugs:
- Non-selective: Propranolol, Nadolol, Timolol
- Cardioselective (β₁): Metoprolol, Atenolol, Bisoprolol
- With vasodilating properties: Carvedilol (α+β block), Labetalol (α+β), Nebivolol (NO-mediated vasodilation)
Special uses:
- Post-MI, stable angina, heart failure (Carvedilol, Bisoprolol, Metoprolol succinate)
- Aortic aneurysm (Propranolol)
- AF rate control
- Prevention of AF recurrence
Adverse Effects/Contraindications:
- Asthma - absolute contraindication (bronchoconstriction)
- AV block grade 2-3
- Mask hypoglycemia symptoms in diabetics
- Metabolic syndrome, glucose intolerance (precaution)
- Depression, psoriasis (relative)
- Athletes and physically active patients (reduces exercise tolerance)
B. Alpha-1 Blockers
Mechanism: Block α₁ receptors on vascular smooth muscle → vasodilation.
Key drugs: Prazosin, Doxazosin, Terazosin
Special use: Useful in men with benign prostatic hypertrophy (BPH) - relaxes prostatic smooth muscle simultaneously.
Adverse Effects:
- First-dose orthostatic hypotension (particularly with Prazosin)
- Contraindicated in heart failure (ALLHAT trial showed worse outcomes)
C. Central Alpha-2 Agonists (Centrally Acting)
Mechanism: Stimulate α₂ receptors in the vasomotor center of the brainstem → reduce sympathetic outflow → decrease HR, CO, and PVR.
Key drugs:
- Methyldopa - drug of choice in pregnancy hypertension
- Clonidine - also used for opioid/nicotine withdrawal; patch formulation available
- Guanabenz, Guanfacine
Adverse Effects: Sedation, dry mouth (xerostomia), bradycardia. Rebound hypertension on abrupt withdrawal (especially clonidine). Contraindicated in depression, AV block grade 2-3.
D. Postganglionic Sympathetic Blockers
Mechanism: Deplete norepinephrine from nerve terminals.
Key drugs:
- Reserpine - depletes catecholamines from vesicles; very inexpensive
- Guanethidine, Guanadrel - block NE release from terminals; rarely used now due to side effects (severe orthostatic hypotension)
5. Direct Vasodilators
A. Hydralazine
- Mechanism: Dilates arterioles (not veins) by unclear mechanism (possible NO-related); causes marked reflex sympathetic activation and sodium retention - must be combined with β-blocker + diuretic.
- Dose: 40-200 mg/day (higher dose increases lupus risk)
- Adverse Effects: Headache, tachycardia, flushing. At ≥400 mg/day: drug-induced lupus (arthralgia, myalgia, skin rash, fever) in ~10-20%, especially in slow acetylators. Peripheral neuropathy (rare).
- Safe in pregnancy (used IV for hypertensive emergencies in pregnancy)
B. Minoxidil
- Mechanism: Opens K⁺ channels in smooth muscle via active metabolite (minoxidil sulfate) → membrane stabilization → reduced contraction. More potent than hydralazine.
- Use: Severe/resistant hypertension, especially in renal failure patients who don't respond to hydralazine. Must be combined with β-blocker + loop diuretic.
- Adverse Effects: Severe fluid retention, tachycardia, hypertrichosis (hair growth - forms basis for topical Rogaine). Pericardial effusion with long-term use.
C. Sodium Nitroprusside
- Mechanism: Releases NO → dilates both arteries and veins → reduces preload and afterload.
- Use: Hypertensive emergencies (IV only); also used in acute heart failure.
- Adverse Effects: Cyanide toxicity with prolonged use (especially renal failure). Requires continuous BP monitoring.
D. Fenoldopam
- Mechanism: D₁-receptor agonist → renal and peripheral vasodilation; increases renal blood flow and sodium excretion.
- Use: Hypertensive emergencies, particularly when renal preservation is desired.
Drug Selection by Compelling Indication
(Source: Goodman & Gilman's Pharmacological Basis of Therapeutics, Katzung, 16th Ed.)
| Condition | Preferred Agents |
|---|---|
| Heart failure | ACEi/ARB, BB (carvedilol, bisoprolol, metoprolol), diuretics, MRA |
| Post-MI | ACEi/ARB, BB |
| Coronary artery disease / Angina | BB, CCB, ACEi/ARB |
| CKD / Proteinuria / Diabetes | ACEi (preferred), ARB |
| Isolated systolic hypertension | Thiazide, CCB (DHP), ACEi/ARB |
| LV hypertrophy | ACEi, ARB, CCB |
| AF rate control | BB, non-DHP CCB (Verapamil, Diltiazem) |
| Atrial fibrillation prevention | ACEi, ARB, BB |
| Aortic aneurysm | BB |
| Peripheral artery disease | ACEi, CCB |
| BPH (men) | Alpha-1 blockers |
| Pregnancy | Methyldopa, Labetalol, Nifedipine; avoid ACEi/ARBs |
| Previous stroke | ACEi/ARB, thiazides |
| Asymptomatic atherosclerosis | CCB |
| Microalbuminuria | ACEi, ARB |
Contraindications Summary
| Drug | Key Contraindications |
|---|---|
| ACEi/ARBs | Pregnancy, bilateral renal artery stenosis, hyperkalemia, angioedema (ACEi history) |
| Thiazides | Gout; caution in metabolic syndrome, hypokalemia |
| Beta-blockers | Asthma, AV block (grade 2-3); caution in COPD, diabetes |
| Verapamil/Diltiazem | AV block, severe LV dysfunction, heart failure |
| Alpha-1 blockers | Heart failure (ALLHAT trial) |
| MRA | Hyperkalemia, significant renal failure |
| Central sympatholytics | Depression, AV block |
Polypharmacy in Resistant Hypertension
Up to 40% of hypertensive patients require 3 or more drugs. The rationale for combination therapy:
- Most drugs evoke compensatory mechanisms that limit their effect (e.g., vasodilators cause reflex tachycardia + sodium retention)
- Adding a β-blocker prevents tachycardia; adding a diuretic prevents sodium retention
- The classic triple combination: vasodilator + β-blocker + diuretic
- Preferred combination: RAS inhibitor + CCB + thiazide (based on RAAS and ACCOMPLISH trial data)
Sources: Katzung's Basic and Clinical Pharmacology, 16th Edition, p. 271-285; Goodman & Gilman's The Pharmacological Basis of Therapeutics, Table 32-4/32-5; Brenner and Rector's The Kidney; Goodman & Gilman, 2018 guidelines (Whelton et al.).
Drugs for chf according to k d tripathi
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have all the content needed for a comprehensive answer structured in the K.D. Tripathi style. Let me compile the complete response:
Note: K.D. Tripathi's Essentials of Medical Pharmacology is not available in the textbook library. The answer below is drawn from Katzung's Basic & Clinical Pharmacology (16th Ed.) and Goodman & Gilman's Pharmacological Basis of Therapeutics - the standard references that cover the same content as Tripathi, often with identical drug classifications and mechanisms. The structure follows the Tripathi-style organization (positive inotropic / non-inotropic; chronic / acute CHF).
Drugs for Congestive Heart Failure (CHF)
CHF occurs when cardiac output is inadequate for the body's needs. Treatment targets: (1) symptom relief and slowing progression in stable CHF, and (2) managing acute decompensation.
Classification of Drugs Used in CHF
DRUGS FOR CHF
│
├── A. POSITIVE INOTROPIC DRUGS
│ ├── 1. Cardiac Glycosides (Digitalis) — Digoxin
│ ├── 2. Beta-Adrenoceptor Agonists — Dobutamine, Dopamine
│ ├── 3. Phosphodiesterase Inhibitors (Bipyridines) — Milrinone, Inamrinone
│ └── 4. Calcium Sensitizers — Levosimendan
│
└── B. NON-INOTROPIC DRUGS (First-line in chronic CHF)
├── 1. Diuretics — Furosemide, Spironolactone, Eplerenone
├── 2. ACE Inhibitors — Captopril, Enalapril, Ramipril
├── 3. Angiotensin Receptor Blockers — Losartan, Valsartan
├── 4. ARNI — Sacubitril/Valsartan (Entresto)
├── 5. Beta-Blockers — Carvedilol, Bisoprolol, Metoprolol succinate
├── 6. Vasodilators — Hydralazine + Isosorbide dinitrate, Nesiritide
├── 7. SGLT2 Inhibitors — Empagliflozin, Dapagliflozin
└── 8. HCN Channel Blocker — Ivabradine
A. POSITIVE INOTROPIC DRUGS
1. Cardiac Glycosides - Digoxin (Digitalis)
Source: Digitalis lanata (digoxin), Digitalis purpurea (digitoxin). Digoxin is the drug in clinical use.
Mechanism:
- Inhibits Na⁺/K⁺-ATPase (the sodium pump) → intracellular Na⁺ accumulates
- ↑ intracellular Na⁺ reduces Ca²⁺ expulsion via Na⁺/Ca²⁺ exchanger (NCX)
- ↑ intracellular Ca²⁺ is stored in SR → released during systole → positive inotropy
Cardiac Effects:
- Mechanical: Increased contractility (positive inotropy)
- Electrical/Electrophysiological:
- Decreased automaticity of SA node (negative chronotropy)
- Decreased AV conduction velocity (negative dromotropy) - useful in AF
- At toxic doses: increased automaticity → arrhythmias
- Indirect (vagal): Bradycardia, decreased AV conduction - mediated via vagus nerve stimulation
Pharmacokinetics (Digoxin):
- Oral bioavailability: ~70-80%
- Protein binding: ~25% (low)
- Half-life: 36-48 hours (prolonged in renal failure)
- Elimination: primarily renal (dose reduction needed in renal insufficiency)
- Narrow therapeutic index: therapeutic level 0.5-2 ng/mL
Uses:
- CHF with atrial fibrillation (drug of choice - slows ventricular rate + improves contractility)
- Systolic CHF (HFrEF) - reduces hospitalizations but does not reduce mortality (DIG trial)
- Atrial flutter/fibrillation for rate control
Toxicity (Digitalis Toxicity):
| System | Manifestations |
|---|---|
| Cardiac | Bradycardia, heart block, ventricular ectopics, bigeminy, VT, VF |
| GI | Anorexia, nausea, vomiting, diarrhea (earliest signs) |
| CNS | Visual disturbances (yellow-green halos - xanthopsia), confusion, headache |
Precipitating factors for toxicity:
- Hypokalemia (most important - K⁺ competes with digoxin at Na⁺/K⁺-ATPase)
- Hypomagnesemia, hypercalcemia, hypothyroidism
- Renal failure, old age, quinidine co-administration (displaces digoxin)
Treatment of Digoxin Toxicity:
- Withhold digoxin
- Correct hypokalemia (KCl IV - if K⁺ is low and no AV block)
- Lignocaine / Phenytoin for ventricular arrhythmias
- Atropine for bradycardia
- Digoxin-specific antibody fragments (Digibind/DigiFab) - definitive antidote for severe toxicity
Contraindications: Hypertrophic obstructive cardiomyopathy (HOCM), WPW syndrome with AF, ventricular tachycardia
2. Beta-Adrenoceptor Agonists
Used only in acute decompensated heart failure (not chronic CHF - worsen long-term outcomes).
| Drug | Receptor | Use |
|---|---|---|
| Dobutamine | β₁ selective | Drug of choice in acute decompensated CHF; increases CO, reduces filling pressure |
| Dopamine | D₁, β₁ (low-moderate dose); α₁ (high dose) | Acute CHF with hypotension; low dose preserves renal blood flow |
Adverse effects: Tachycardia, arrhythmias, myocardial ischemia (increase O₂ demand), tachyphylaxis with continued use.
3. Phosphodiesterase Inhibitors (Bipyridines)
Drugs: Milrinone (IV only), Inamrinone (historical)
Mechanism: Inhibit PDE-3 → ↑ cAMP → ↑ intracellular Ca²⁺ → positive inotropy + vasodilation ("inodilators")
Use: Acute decompensated CHF or severe exacerbation of chronic CHF (IV only)
Adverse effects: Arrhythmias, hypotension, thrombocytopenia (inamrinone). Long-term oral use increases mortality - so IV short-term only.
4. Calcium Sensitizers
Levosimendan:
- Sensitizes troponin complex to Ca²⁺ → enhanced contractility without increasing intracellular Ca²⁺
- Also inhibits PDE and causes vasodilation
- Approved in several countries (not USA) for acute HF
- Advantage: less arrhythmogenic than digitalis
B. NON-INOTROPIC DRUGS (First-line for Chronic CHF)
These are the cornerstone of CHF management and improve survival.
1. Diuretics
Drug of choice for symptomatic relief in CHF.
Furosemide (Loop diuretic) - first choice:
- Reduces preload by reducing venous return and blood volume
- Rapid IV action in acute pulmonary edema
- Also causes venodilation (independent of diuresis)
Spironolactone / Eplerenone (Aldosterone antagonists / MRA):
- Block aldosterone receptors → reduce Na⁺ retention, prevent myocardial fibrosis, reduce baroreceptor dysfunction
- Reduce morbidity and mortality in severe CHF (RALES trial for spironolactone, EPHESUS for eplerenone)
- Use in NYHA class II-IV when CrCl >30 mL/min and K⁺ <5 mmol/L
- Finerenone - newer non-steroidal MRA with lower hyperkalemia risk
Thiazides: Used in mild CHF or as add-on; less effective when GFR is reduced.
2. ACE Inhibitors (First-line, All Stages of CHF)
Drugs: Captopril, Enalapril, Ramipril, Lisinopril, Perindopril
Mechanism in CHF:
- ↓ peripheral resistance → ↓ afterload (easier for failing heart to pump)
- ↓ aldosterone → ↓ Na⁺/water retention → ↓ preload
- ↓ sympathetic activity (AngII promotes NE release presynaptically)
- Prevent and reverse cardiac remodeling (key long-term benefit)
- Reduce mortality, hospitalizations, and slow progression (CONSENSUS, SOLVD trials)
Key point: Started at low dose and uptitrated; all patients with HFrEF should receive unless contraindicated.
Contraindications: Bilateral renal artery stenosis, pregnancy, hyperkalemia, angioedema history.
3. Angiotensin Receptor Blockers (ARBs)
Drugs: Losartan, Valsartan, Candesartan
- Used when patients cannot tolerate ACEi (due to cough)
- Similar benefits to ACEi in reducing mortality and hospitalization
- Do not cause cough (no bradykinin effect)
- Do not combine ACEi + ARB in CHF (increased renal adverse effects without added mortality benefit)
4. ARNI - Sacubitril/Valsartan (Entresto) ★ New Standard of Care
Mechanism: Sacubitril inhibits neprilysin (enzyme that degrades natriuretic peptides BNP, ANP) → ↑ natriuretic peptide levels → vasodilation + diuresis; combined with valsartan (ARB) to prevent unopposed AngII effects.
Evidence: PARADIGM-HF trial - superior to enalapril in reducing CV death and HF hospitalization in HFrEF.
Use: Replace ACEi/ARB with sacubitril/valsartan in NYHA II-III with adequate BP and no contraindications to ARB.
Note: Do NOT combine with ACEi (angioedema risk); wash out ACEi for 36 hours before starting.
5. Beta-Blockers (Paradoxically Beneficial in Chronic CHF)
Drugs approved for CHF: Carvedilol (α₁+β₁+β₂), Bisoprolol (β₁ selective), Metoprolol succinate (β₁ selective)
Rationale: In CHF, chronic SNS activation is initially compensatory but chronically harmful (promotes hypertrophy, apoptosis, arrhythmias, remodeling). Beta-blockers counteract this.
Mechanism benefits:
- Prevent catecholamine-mediated myocardial toxicity and remodeling
- Reduce heart rate → more diastolic filling time
- Anti-arrhythmic (reduce sudden death)
- Reduce wall stress
Evidence: Reduce mortality by ~30-35% in HFrEF (MERIT-HF, COPERNICUS, CIBIS-II trials)
Important: Start at very low dose, uptitrate slowly. Acutely reduce cardiac output (patient may feel worse initially), but long-term benefit is substantial.
Contraindications in CHF: Decompensated/acute heart failure (wait till stable), asthma, severe bradycardia, AV block.
6. Vasodilators
Hydralazine + Isosorbide Dinitrate (H-ISDN):
- Hydralazine: arteriolar dilator → ↓ afterload
- ISDN: venodilator → ↓ preload
- Used particularly in African-American patients with NYHA III-IV on standard therapy (A-HeFT trial)
- Also used when ACEi/ARBs are contraindicated (e.g., renal failure, pregnancy)
Nesiritide (BNP analogue):
- Recombinant BNP → vasodilation + diuresis via ↑ cGMP
- IV use in acute CHF; reduces filling pressures
- Large trials (ASCEND-HF) failed to show mortality reduction; risk of hypotension and renal toxicity - used with caution
7. SGLT2 Inhibitors ★ (Newest Addition)
Drugs: Empagliflozin (EMPEROR-Reduced), Dapagliflozin (DAPA-HF)
Mechanism in CHF: Not fully understood - reduces cardiac preload/afterload via osmotic diuresis, improves myocardial energetics, reduces inflammation and fibrosis, possible direct myocardial effects.
Key finding: Reduce CV death and HF hospitalization in both diabetic AND non-diabetic CHF patients. Now part of standard quadruple therapy.
8. Ivabradine
Mechanism: Blocks HCN (If) channels in SA node → reduces heart rate without affecting contractility or blood pressure.
Use: NYHA II-III, sinus rhythm, HR >70 bpm despite maximally tolerated beta-blocker dose (SHIFT trial - reduces HF hospitalization).
Not used in AF (no SA node to inhibit).
Treatment Algorithm for HFrEF (Chronic Systolic CHF)
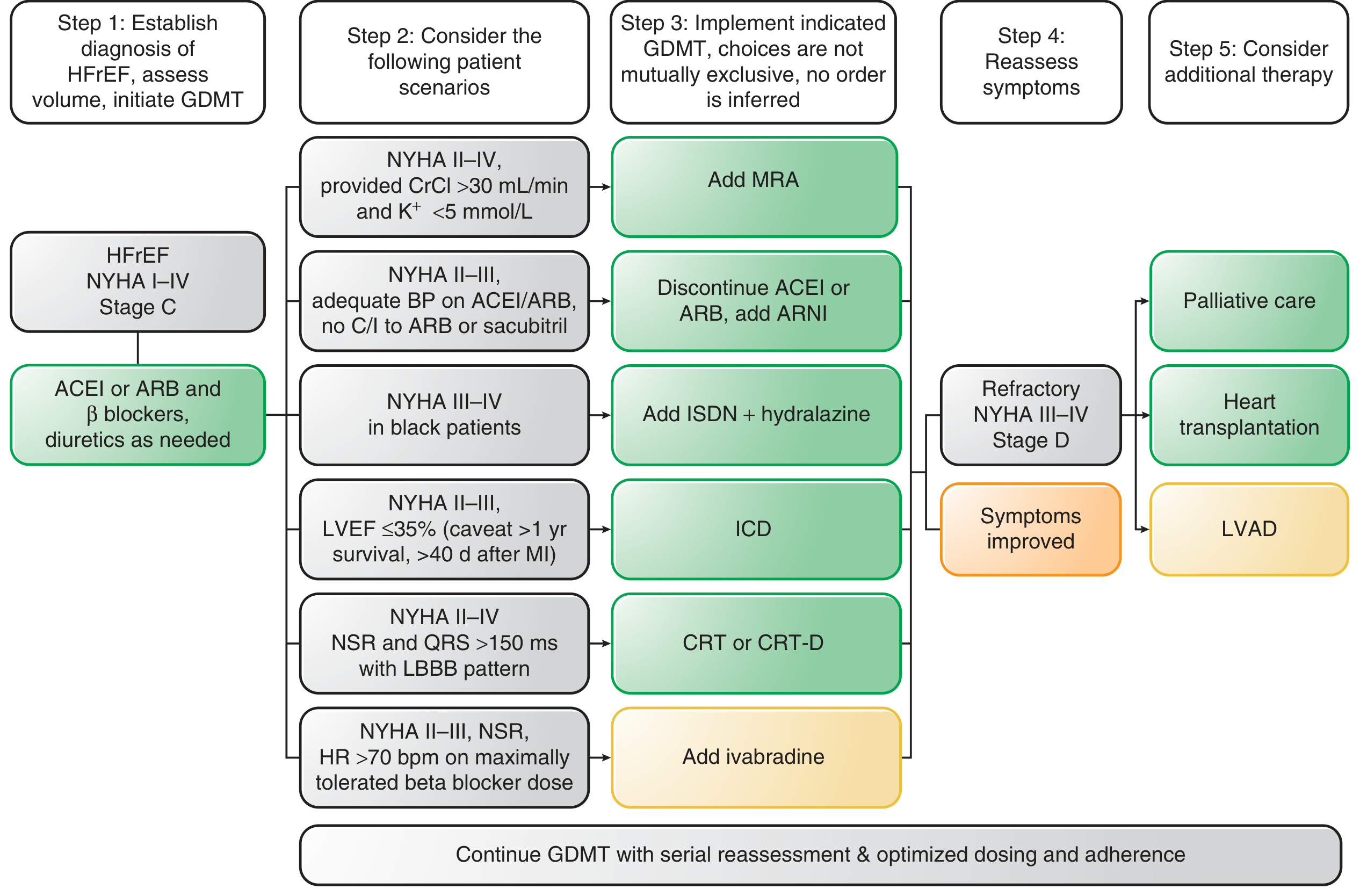
Standard Quadruple Therapy (Modern Pillar):
- ACEi / ARB or ARNI (Sacubitril/Valsartan)
- Beta-blocker (Carvedilol / Bisoprolol / Metoprolol succinate)
- MRA (Spironolactone / Eplerenone)
- SGLT2 inhibitor (Empagliflozin / Dapagliflozin)
Add diuretics (Furosemide) for symptom relief as needed. Digoxin for rate control in AF or persistent symptoms despite above.
Drugs for Acute Decompensated CHF (Acute Pulmonary Edema)
| Drug | Role |
|---|---|
| IV Furosemide | First-line - rapid diuresis and venodilation |
| IV Morphine | Venodilation + anxiolysis (reduces anxiety/dyspnea) |
| Oxygen | Correct hypoxia |
| Dobutamine | If low CO and hypoperfusion |
| Dopamine | If hypotension + low CO |
| IV Nitrates (NTG) | Venodilation in acute pulmonary edema |
| Milrinone | Severe exacerbation, refractory to above |
| Nesiritide | IV vasodilation (second-line) |
| Digoxin | CHF + rapid AF |
Summary Table: Drugs Improving Survival in CHF
| Drug Class | Key Drugs | Survival Benefit |
|---|---|---|
| ACEi | Enalapril, Captopril | ✅ Yes (CONSENSUS, SOLVD) |
| ARB | Valsartan, Candesartan | ✅ Yes |
| ARNI | Sacubitril/Valsartan | ✅ Yes (superior to ACEi) |
| Beta-blockers | Carvedilol, Bisoprolol, Metoprolol | ✅ Yes (~35% ↓ mortality) |
| MRA | Spironolactone, Eplerenone | ✅ Yes (RALES, EPHESUS) |
| SGLT2 inhibitors | Empagliflozin, Dapagliflozin | ✅ Yes |
| Digoxin | Digoxin | ❌ No mortality benefit (reduces hospitalization only) |
| Diuretics | Furosemide | ❌ Symptom relief only |
| Vasodilators | H-ISDN | ✅ Modest (in African-Americans) |
| Beta-agonists | Dobutamine | ❌ Acute use only; chronic use harmful |
Sources: Katzung's Basic and Clinical Pharmacology, 16th Edition, Chapter 13 (Drugs Used in Heart Failure); Goodman & Gilman's Pharmacological Basis of Therapeutics, Chapter 33 (Drug Treatment of Chronic Systolic Heart Failure).
This is a shared conversation. Sign in to Orris to start your own chat.