Paraganglioma point wise
Reading File
Finding Sources
Finding Sources
Searching PubMed
paraganglioma
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a comprehensive, point-wise answer. Let me compile it:
Paraganglioma - Point Wise
1. Definition & Origin
- Paragangliomas (PGLs) are neoplasms arising from neuroendocrine cells (chromaffin/chief cells) associated with the sympathetic and parasympathetic nervous systems
- They originate from neural crest-derived paraganglionic cells distributed throughout the body
- The adrenal medullary pheochromocytoma is the most common paraganglioma, accounting for 80-85% of all cases
- Extra-adrenal paragangliomas represent the remaining 15-20%; approximately 70% of these occur in the head and neck
- Robbins, Cotran & Kumar Pathologic Basis of Disease
2. Classification by Location
A. Paravertebral (Sympathetic) Paragangliomas
- Arise from paravertebral sympathetic ganglia and the organ of Zückerkandl (near the aortic bifurcation)
- Have sympathetic connections
- Stain positively for chromaffin - indicating catecholamine production
- More likely to be functionally active (secrete catecholamines)
B. Head & Neck (Parasympathetic) Paragangliomas
| Site | Name | Key Feature |
|---|---|---|
| Carotid bifurcation | Carotid body tumor | Most common H&N paraganglioma |
| Jugular bulb | Glomus jugulare | Cranial nerve deficits |
| Cochlear promontory | Glomus tympanicum | Pulsatile tinnitus |
| Vagus nerve | Vagal paraganglioma | Cervical mass, voice change |
| Aortic bodies | Aortico-pulmonary chain | - |
| Larynx | Laryngeal paraganglioma | Supraglottic, 3rd most common neuroendocrine tumor of larynx |
- These are innervated by the parasympathetic system
- Only rarely produce catecholamines (up to 5% in H&N)
- Scott-Brown's Otorhinolaryngology; Robbins
3. Epidemiology
- Rare, slow-growing, painless masses
- Peak incidence: 5th and 6th decades of life
- Laryngeal paragangliomas: 3x more common in women
- Incidence is higher at high altitudes (possible hypoxic stimulus)
- Usually solitary and sporadic, but ~10% are multifocal
- Robbins; Cummings Otolaryngology
4. Genetics & Hereditary Syndromes
- 30-40% of all pheochromocytomas/paragangliomas harbor an oncogenic germline mutation
- Hereditary cases are typically younger at presentation and more often bilateral
Key Genetic Associations:
| Syndrome | Gene | Associated Tumor | Other Features |
|---|---|---|---|
| MEN-2A | RET | Pheo/PGL | Medullary thyroid Ca, parathyroid hyperplasia |
| MEN-2B | RET | Pheo/PGL | Medullary thyroid Ca, marfanoid habitus, mucosal GNs |
| NF-1 | NF1 | Pheochromocytoma | Neurofibromas, café-au-lait spots |
| von Hippel-Lindau | VHL | Pheo/PGL | RCC, hemangioblastoma, pancreatic NET |
| Hereditary PGL-1 | SDHD | Pheo + PGL | GIST |
| Hereditary PGL-3 | SDHC | PGL only | GIST |
| Hereditary PGL-4 | SDHB | Pheo + PGL | GIST |
| Polycythemia-PGL syndrome | EPAS1 (HIF-2α) | Pheo/PGL | Polycythemia |
- SDH mutations are the most frequent cause of hereditary PGL; loss-of-function mutations in SDH subunits alter cellular metabolism ("pseudohypoxia" phenotype)
- SDHB mutation carries the highest metastatic risk (30-50%)
- PGL types 1-4 (SDH gene syndromes) typically involve head and neck paragangliomas
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Table 24.10
5. Pathology / Morphology
Gross
- Carotid body tumor: rarely exceeds 6 cm, arises at or envelops the carotid bifurcation
- Red-pink to brown, well-circumscribed
- Highly vascular - embolization targets
Microscopy
- Characteristic Zellballen pattern: nests of round-to-oval chief cells surrounded by delicate vascular septae
- Chief cells: neuroectodermal origin; abundant clear or granular eosinophilic cytoplasm; uniform nuclei; few mitoses
- Sustentacular cells: spindle-shaped supporting stromal cells around nest periphery
Immunohistochemistry
| Marker | Cell | Result |
|---|---|---|
| Chromogranin | Chief cells | Positive |
| Synaptophysin | Chief cells | Positive |
| INSM1 | Chief cells | Positive |
| CD56 | Chief cells | Positive |
| S-100 | Sustentacular cells | Positive |
- Electron microscopy: well-demarcated neuroendocrine granules in paravertebral tumors (scant in non-functioning tumors)
- Robbins
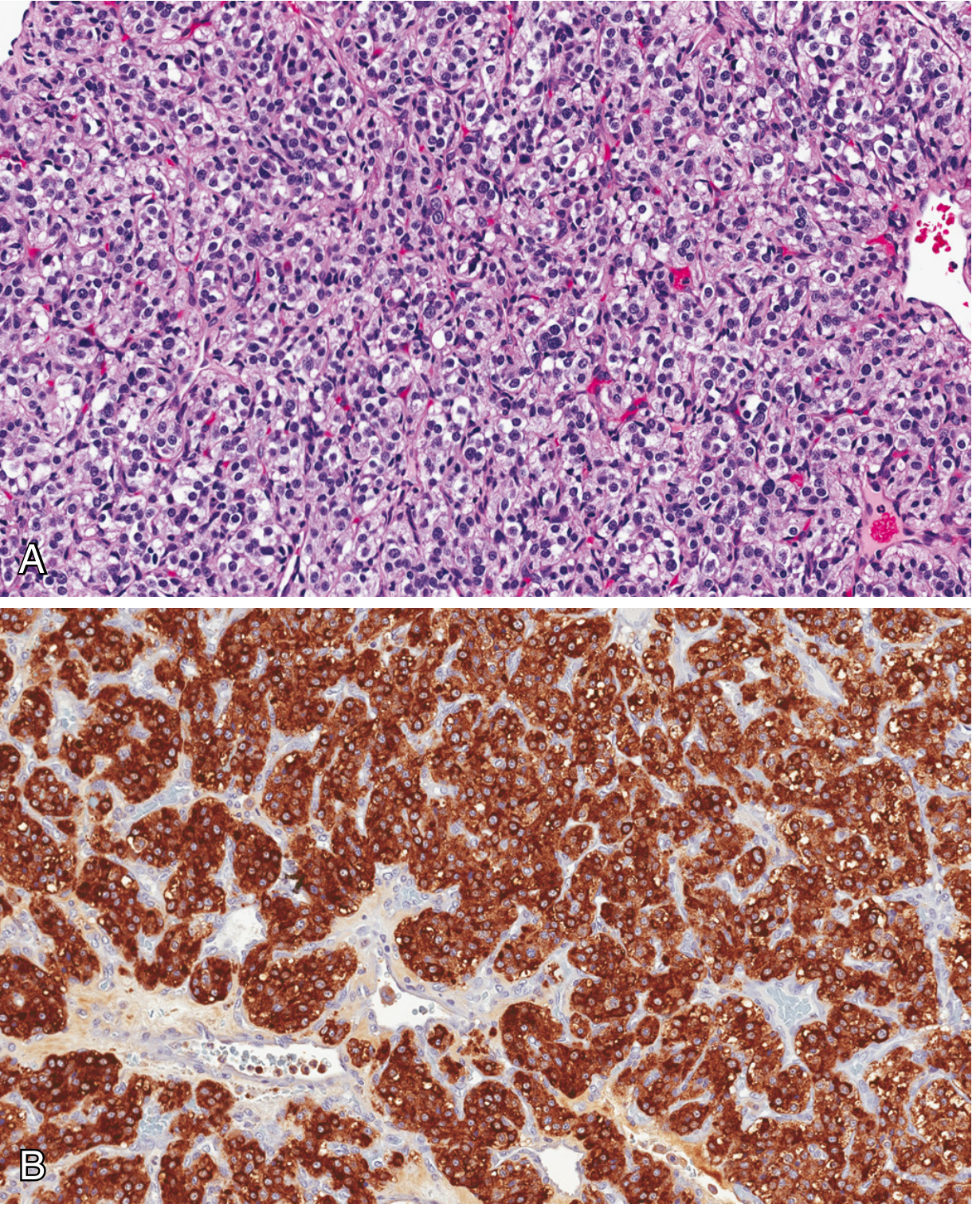
Fig. 16.17 - Carotid body tumor: (A) Zellballen pattern with fibrovascular septa, (B) Chromogranin IHC (Robbins)
6. Clinical Features
By Location:
- Glomus tympanicum: pulsatile tinnitus, conductive hearing loss, red pulsatile mass behind tympanic membrane
- Glomus jugulare: cranial nerve palsies (CN IX-XII), pulsatile tinnitus
- Carotid body tumor: painless lateral neck mass at carotid bifurcation ("lyre sign" on angiography); splays the carotid vessels
- Vagal paraganglioma: high cervical mass, CN X palsy, hoarseness
- Functional tumors: hypertension (paroxysmal or sustained), palpitations, headache, diaphoresis (due to catecholamine secretion)
General:
- Most are painless and slow-growing
- Symptoms mainly arise from compression of adjacent structures
- ~1-3% of glomus jugulare tumors secrete catecholamines
- Cummings; Scott-Brown's
7. Malignancy
- All PGLs should be considered potentially malignant - the terms "benign" and "malignant" are no longer recommended per current classification
- The term "metastatic paraganglioma" is used when metastatic disease is present
- Histologic features (mitoses, pleomorphism, vascular invasion) do NOT reliably predict metastatic behavior
- SDHB mutations = highest metastatic risk (30-50%)
- Metastatic behavior is more common in extra-adrenal PGLs (20-40%)
- Up to 50% of metastatic paragangliomas are ultimately fatal, mainly due to infiltrative growth
- Carotid body tumors may metastasize to regional lymph nodes and distant sites despite benign histology
- Robbins
8. Imaging
| Modality | Role |
|---|---|
| CT (high-resolution) | Best for bony involvement, temporal bone erosion |
| MRI | Best for soft tissue extent, intracranial invasion; "salt and pepper" appearance on T2 |
| Intra-arterial angiography | Very specific - shows enlarged feeding arteries, early intense blush, centripetally oriented arterioles; done as pre-embolization evaluation |
| Octreotide scan | Useful pre-op to confirm diagnosis, avoid biopsy |
| MIBG scan | For functional tumors; catecholamine-secreting PGLs |
- Carotid artery involvement and intracranial invasion must be specifically sought
- Angiography reveals multi-compartment blood supply with arteriovenous shunts
- Avoid biopsy of vascular lesions - diagnose preoperatively on imaging + octreotide scan to avoid hemorrhage
- Scott-Brown's; Cummings
9. Treatment
Surgery
- Surgical excision is the definitive treatment for most PGLs
- Carotid body tumors: resection with vascular control
- Laryngeal PGLs: lateral thyrotomy or lateral pharyngotomy (open approach preferred for hemostasis); transoral CO2 laser not recommended due to hemostasis difficulty
- Neck dissection NOT indicated for laryngeal paragangliomas (they do not metastasize to cervical nodes)
- Pre-operative embolization is used as an adjuvant to reduce intraoperative blood loss
Radiation Therapy
- Glomus jugulare (Fisch class C/D): stereotactic radiosurgery (SRS) is the preferred method - better cranial nerve preservation vs. surgery, similar/better local control
- Fisch class A/B (middle ear confined): surgery preferred
- PGLs respond to RT but incompletely; RT is mainly for growth control, not cure
Embolization
- Pre-operative embolization due to highly vascular nature
- Particles sized to penetrate peripheral arteries (~90 microns); multiple injections needed due to multi-compartment supply
- Percutaneous/intra-operative direct puncture with liquid embolic agent may be used where AV shunts present
- Embolization alone (without surgery/RT) can provide symptomatic relief and stabilize growth
Functional Tumors
- Pre-operative alpha-adrenergic blockade (phenoxybenzamine) + beta-blockade to prevent hypertensive crisis
10. Key Concepts Summary
| Feature | Detail |
|---|---|
| Origin | Neural crest, neuroendocrine cells |
| Most common | Adrenal pheochromocytoma (80-85%) |
| Histology hallmark | Zellballen pattern |
| IHC markers | Chromogranin, synaptophysin (chief cells); S-100 (sustentacular cells) |
| Most common germline mutations | SDH subunits (SDHB, SDHC, SDHD) |
| Highest malignancy risk | SDHB mutation (30-50% metastatic) |
| H&N most common site | Carotid body (35%), temporal bone (50%) |
| Functional secretion in H&N | ~5% secrete catecholamines |
| Malignancy assessment | Based on metastasis ONLY (not histology) |
| Preferred imaging | CT (bone) + MRI (soft tissue) |
| Laryngeal PGL | 3x more in women; supraglottic; avoid biopsy |
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (Chapters 16 & 24)
- Cummings Otolaryngology Head and Neck Surgery
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Recent evidence note: A 2024 systematic review (PMID 38605204) on SDHB pathogenic variant carriers confirms the high metastatic risk associated with SDHB mutations. A 2024 meta-analysis (PMID 38942141) on preoperative embolization in jugular paraganglioma surgery provides updated evidence on its role as a surgical adjuvant.
Make pdf
Reading File
Running Command
Writing File
Running Command
Your PDF is ready:
Paraganglioma
PDF Document · PDF
The PDF includes all 10 sections from the notes:
- Definition & Origin
- Classification by Location (with table)
- Epidemiology
- Genetics & Hereditary Syndromes (full gene table + highlighted SDHB warning)
- Pathology / Morphology (gross, microscopy, IHC table)
- Clinical Features (by-location table)
- Malignancy (with red alert box on current classification)
- Imaging (modality table)
- Treatment (surgery, SRS, embolization, functional tumors)
- Key Concepts Summary table
Formatted with a navy color scheme, highlighted warning boxes, and source citations at the footer.
This is a shared conversation. Sign in to Orris to start your own chat.