Hepatic hemangioma: introduction, causes, pathophysiology, symptoms and management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hepatic hemangioma"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information. Let me compile the full, well-structured answer.
Hepatic Hemangioma
Introduction
Hepatic hemangioma is the most common benign liver lesion, occurring in 5-20% of the general population. Most are discovered incidentally during abdominal imaging performed for unrelated reasons. They are true vascular malformations - not neoplasms - and carry no risk of malignant transformation. The vast majority remain asymptomatic throughout a patient's lifetime and require no treatment.
Current Surgical Therapy 14e defines them as "congenital malformations comprising blood-filled cavernous spaces lined by a single layer of endothelial cells and separated by fibrous tissue." They are round, well-encapsulated, and may contain thrombi or calcifications.
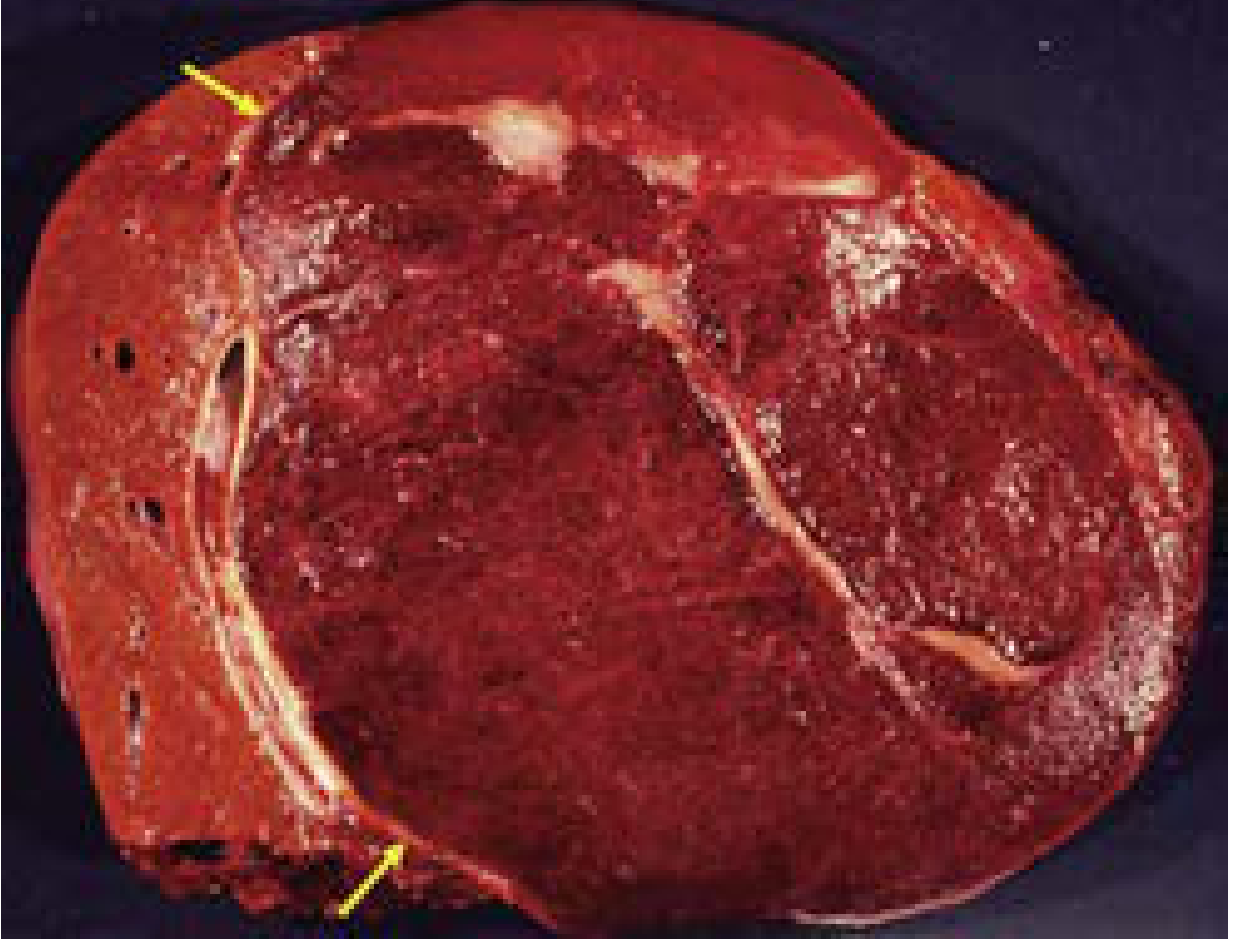
FIG. 1 - Hepatic hemangioma with surrounding pseudocapsule (arrows). Note the dark red, sponge-like appearance of blood-filled cavernous spaces. (Current Surgical Therapy 14e)
Causes / Etiology
The exact etiology is not fully understood, but several factors are established:
- Congenital origin: Hemangiomas are considered congenital vascular malformations, not acquired tumors. They arise from disordered embryological development of hepatic sinusoids.
- Sex predilection: They occur predominantly in women aged 20 to 50 years, suggesting a hormonal influence.
- Estrogen exposure: Although hemangiomas lack estrogen receptors, estrogen exposure (e.g., oral contraceptive use, pregnancy) is associated with higher rates of enlargement. Importantly, this does not increase the risk of rupture.
- Most are solitary: Approximately 90% of patients present with a single lesion; only ~10% have multifocal disease.
Pathophysiology
Structural Anatomy
Hemangiomas consist of large, blood-filled vascular spaces (cavernous sinusoids) lined by a single layer of flat endothelial cells, separated by thin fibrous septa. They have the consistency of a soft, sponge-like sac that compresses with pressure.
Key structural features:
- Pseudocapsule: A fibrous cleavage plane exists between the hemangioma and surrounding liver parenchyma - this is clinically important as it facilitates surgical enucleation.
- Thrombosis: Common within the lesion; dystrophic calcification may follow.
- Fibrous interface patterns (Zimmermann's classification, per Maingot's Abdominal Operations):
- Fibrous interface - avascular capsule-like fibrous lamellae (most common in large hemangiomas; best for enucleation)
- Interdigitating interface - mixture of parenchymal and hemangioma components without a capsule
- Compression interface - direct apposition of hemangioma and parenchyma
- Irregular/spongy interface - highly irregular border with parenchymal foci interspersed
Blood Supply and Hemodynamics
Hepatic hemangiomas are predominantly supplied by the hepatic artery (not portal vein). Blood pools within the cavernous spaces and drains slowly - this accounts for the characteristic "fill-in" pattern on contrast imaging. The slow flow also predisposes to intralesional thrombosis.
Natural History
Most hemangiomas exhibit either slow growth or no growth over time. Spontaneous rupture is exceedingly rare (only ~30 reported cases in the literature). The lesion has no malignant potential.
Symptoms and Clinical Presentation
The vast majority of hemangiomas are asymptomatic and discovered incidentally. When symptoms do occur, they are more common with larger lesions (especially those >10 cm, termed "giant hemangiomas").
Common Symptoms
- Right upper quadrant or epigastric abdominal pain/discomfort
- Abdominal fullness or pressure sensation
- Early satiety (from compression of adjacent stomach or duodenum)
- Nausea and vomiting
A plausible explanation for pain is distension of Glisson's capsule - the fibrous envelope of the liver, which is innervated. However, the majority of patients with capsular involvement remain symptom-free.
Complications (Rare)
| Complication | Details |
|---|---|
| Kasabach-Merritt Syndrome | Consumptive coagulopathy due to platelet trapping within the hemangioma. Features: thrombocytopenia, hypofibrinogenemia, elevated fibrin degradation products, coagulopathy. More common in giant hemangiomas in children. |
| Spontaneous rupture | Extremely rare (<30 cases reported). Life-threatening intra-abdominal hemorrhage requiring emergency intervention. |
| Intratumoral bleeding | Not life-threatening but may cause acute-onset symptoms. |
| Biliary obstruction | Rare; occurs with very large lesions compressing bile ducts. |
| Budd-Chiari syndrome | Extremely rare; caused by compression of hepatic venous outflow by very large hemangiomas. |
Diagnosis and Imaging
Diagnosis is almost exclusively radiological - biopsy is generally avoided due to risk of hemorrhage and poor diagnostic yield (~23% accuracy in one series).
Ultrasound (First-line)
- Well-demarcated, homogeneous, hyperechoic lesion
- Well-circumscribed with posterior acoustic enhancement (no shadowing)
- Particularly accurate for small lesions (<3 cm)
- Contrast-enhanced ultrasound (CEUS) can highlight typical vascular enhancement
CT Scan (Most Common Diagnostic Tool)
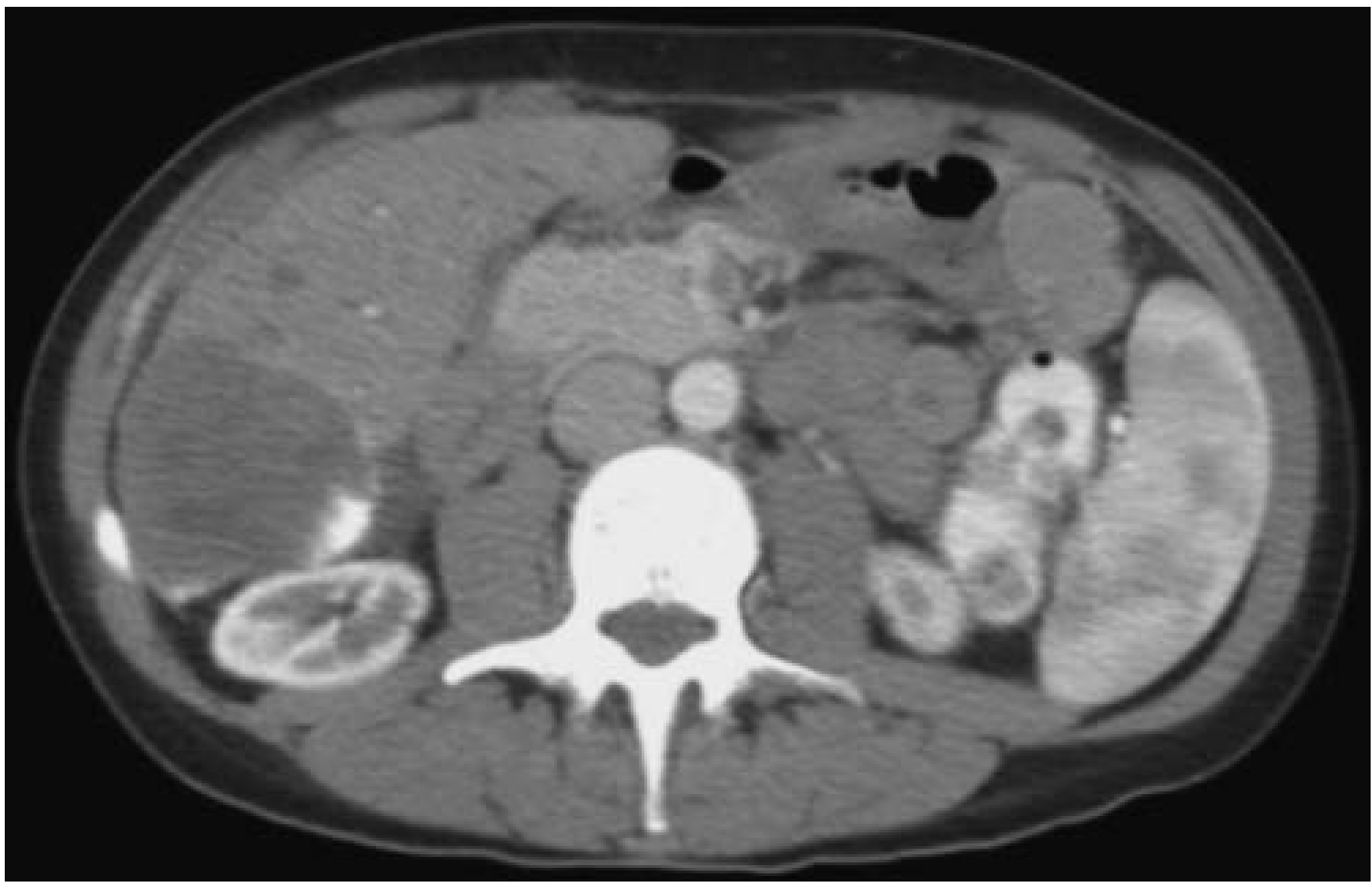
FIG. 2 - Arterial phase CT of hepatic hemangioma in the right hemiliver. Note the characteristic nodular peripheral contrast enhancement. (Maingot's Abdominal Operations)
Five CT criteria diagnostic of hemangioma (Maingot's):
- Low-density lesion on unenhanced scan
- Early peripheral (nodular) contrast enhancement in arterial phase
- Progressive centripetal opacification from periphery toward center
- Delay of at least 3 minutes before total opacification
- Eventually isodense appearance
Presence of criteria 4 and 5 plus any two others is considered diagnostic (76% of lesions meet all five criteria).
MRI (Most Sensitive - 96% Accuracy)
- Hypointense on T1-weighted sequences (vs. surrounding liver)
- Markedly hyperintense on T2-weighted sequences ("light bulb" sign)
- Gadolinium enhancement mirrors the CT pattern (peripheral nodular fill-in)
- Preferred when CT is inconclusive
Management
Four Core Principles (Current Surgical Therapy 14e)
- The majority of patients, regardless of size, are asymptomatic and do not require intervention.
- A broad differential diagnosis (GERD, peptic ulcer disease, gallstones) should always be considered before attributing symptoms to a hemangioma.
- When resection is considered, minimally invasive approaches are preferred when feasible; however, they should not expand indications for treatment.
- Operative treatment does not improve symptoms in approximately 30-50% of selected patients - careful patient selection is therefore mandatory.
Non-Operative Management (Default for Most Patients)
| Scenario | Recommendation |
|---|---|
| Asymptomatic, small lesion, clear diagnosis | No follow-up needed |
| Large lesion (>5 cm) or diagnostic uncertainty | Follow-up imaging in 3-6 months |
| Significant growth or symptoms | Consider intervention |
The natural history is stable - even large lesions (median 6 cm) followed nonoperatively over a median of 52 months show no complications, per a Dutch cohort study cited in Maingot's.
Indications for Surgery
Three accepted indications for resection:
- Severe, attributable symptoms refractory to conservative management
- Inability to confidently exclude malignancy on imaging (diagnostic equipoise)
- Development of complications (hemorrhage, Kasabach-Merritt syndrome)
Note: Size alone is not an indication for resection. Giant hemangiomas (>10 cm) may be safely observed if asymptomatic.
Surgical Options
Enucleation (preferred when possible)
- Takes advantage of the fibrous pseudocapsule as a cleavage plane
- Associated with lower postoperative complications vs. formal resection
- Similar transfusion rates to hepatic resection
- In a Memorial Sloan Kettering series, 60% of operative cases were managed by enucleation
Formal Hepatic Resection
- Used when enucleation is not technically feasible (e.g., central or deeply located lesions)
- Minimally invasive (laparoscopic/robotic) approaches preferred when technically feasible
Hepatic Artery Embolization (Transarterial Embolization)
- Used preoperatively to control bleeding in ruptured hemangiomas before surgery
- Can be used pre-resection for giant hemangiomas to reduce intraoperative blood loss
- Used for symptomatic patients who are not surgical candidates
- Controversy exists about long-term symptom relief from embolization alone
Liver Transplantation
- Considered only in exceedingly rare cases of unresectable hemangioma with Kasabach-Merritt syndrome or Budd-Chiari syndrome that cannot otherwise be managed.
Management of Specific Complications
- Kasabach-Merritt syndrome: Surgical resection is the preferred treatment if technically feasible (coagulopathy resolves post-resection). Inoperable cases: embolization with glucocorticoids, propranolol, or cytotoxic therapy. Thromboelastography (TEG) or ROTEM guides perioperative coagulation management.
- Spontaneous rupture: Emergency management with angiographic embolization first to control hemorrhage, followed by surgical resection.
- Budd-Chiari syndrome from hemangioma: Liver resection if hepatic outflow can be preserved; transplantation in extreme cases.
Summary Table
| Feature | Details |
|---|---|
| Prevalence | 5-20% of the population |
| Demographics | Women 20-50 years most commonly |
| Nature | Congenital vascular malformation; benign, no malignant potential |
| Histology | Cavernous blood-filled spaces, single endothelial cell lining, fibrous septa |
| Typical size | mm to cm; >10 cm = "giant" |
| Symptoms | Usually none; RUQ pain, satiety, fullness if large |
| Best imaging | MRI (96% accuracy); CT and US also diagnostic |
| Hallmark imaging | Peripheral nodular enhancement with centripetal fill-in |
| Treatment | Observation for most; surgery (enucleation preferred) for severe symptoms, diagnostic uncertainty, or complications |
Sources: Current Surgical Therapy 14e, p. 406-410; Maingot's Abdominal Operations, p. 947-950
This is a shared conversation. Sign in to Orris to start your own chat.