Can u explain about abdominal pain with urtricatia from basics to advanced
Reading File
Finding Sources
Finding Sources
Searching PubMed
urticaria abdominal pain mechanism
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
I now have comprehensive content from multiple authoritative textbooks. Let me compose the full answer.
Abdominal Pain with Urticaria: Basics to Advanced
1. What Is Urticaria?
Urticaria (hives) consists of transient, pruritic wheals - raised, erythematous, blanching skin lesions caused by localized edema in the superficial dermis. About 15-20% of the population experiences urticaria at some point in their lifetime. When edema extends deeper into the dermis, subcutaneous tissue, or mucosa, it becomes angioedema - and it is angioedema that most directly explains abdominal pain.
Key morphology:
- Wheals: superficial, pale center with erythematous flare, usually resolve within 24 hours
- Angioedema: deeper, asymmetric swelling, may or may not be pruritic
- The two frequently coexist, but each can occur in isolation

2. Classification
By Duration
| Type | Definition |
|---|---|
| Acute | < 6 weeks |
| Chronic | ≥ 6 weeks, recurrent |
Chronic Subtypes
- Chronic spontaneous urticaria (CSU) - ~80%, no identifiable trigger
- Chronic inducible urticaria - ~20%, specific physical stimulus
By Mechanism (Clinically Important for Abdominal Pain)
| Category | Mediator | Abdominal Pain Risk |
|---|---|---|
| Histaminergic (mast-cell driven) | Histamine | Moderate (via angioedema) |
| Bradykinin-mediated (HAE, ACE-I) | Bradykinin | High - severe GI swelling |
| Urticarial vasculitis | Immune complex | High (with hypocomplementemia) |
| Mastocytosis | Multiple mediators | Moderate-high |
3. Pathophysiology: How Urticaria Causes Abdominal Pain
3A. Mast Cell Degranulation (Core Mechanism)
Mast cells in the skin AND gut wall degranulate, releasing:
- Histamine - H1 receptors cause itch/wheal in skin; H2 receptors increase gastric acid; both cause smooth muscle contraction and vascular permeability
- Bradykinin, kallikrein - vasodilators causing plasma extravasation
- Leukotrienes, prostaglandins - amplify inflammation and bowel motility changes
- Acetylcholine - cholinergic pathway relevant in cholinergic urticaria
When mast cells in the gut wall degranulate, the result is mucosal edema, submucosal swelling, increased intestinal motility - producing crampy abdominal pain, nausea, vomiting, and diarrhea.
3B. Angioedema of the Bowel Wall
This is the single most important mechanism linking urticaria/angioedema to abdominal pain. Fluid leaks into the bowel wall layers, causing:
- Thickened intestinal loops (visible on CT)
- Functional obstruction or pseudo-obstruction
- Severe cramping, distension, and vomiting
- Ascites in severe cases
The clinical result: patients may present with an acute abdomen that mimics surgical emergencies.
3C. Two Distinct Pathways
| Pathway | Mediator | Responds to Antihistamines? |
|---|---|---|
| IgE/mast cell (type I hypersensitivity) | Histamine | YES |
| Bradykinin-mediated (HAE, ACE-I) | Bradykinin | NO |
This distinction is critical in management - bradykinin-mediated angioedema does NOT respond to epinephrine, antihistamines, or steroids.
4. Major Causes of Abdominal Pain + Urticaria
4A. Anaphylaxis (Most Urgent)
The most dangerous combination. In anaphylaxis:
- Skin (urticaria, flushing, angioedema): ~90% of cases
- GI symptoms (abdominal pain, nausea, vomiting, diarrhea): ~45% of cases
- Cardiovascular, respiratory involvement also present
Common triggers: foods (nuts, shellfish, eggs), drugs (penicillin, NSAIDs), insect venom, latex, exercise
The Harriet Lane Handbook (23rd ed.) classifies GI involvement as the third most common system affected in anaphylaxis after cutaneous and respiratory.
4B. Hereditary Angioedema (HAE) - Advanced but Critical to Know
HAE is caused by a deficiency or dysfunction of C1 esterase inhibitor (C1-INH), leading to uncontrolled complement and kallikrein-kinin activation with excess bradykinin production.
Types:
| Type | Defect |
|---|---|
| HAE Type I (~85%) | Low C1-INH quantity |
| HAE Type II (~15%) | Normal quantity, dysfunctional C1-INH |
| HAE with normal C1-INH | Mutations in Factor XII, plasminogen, others |
Key clinical features (Tietz Textbook, 7th ed.):
- Recurrent attacks of nonpitting, nonpruritic edema (NO urticaria, NO itch)
- Predominantly affects skin, gut, larynx
- Abdominal attacks - the most debilitating manifestation: severe crampy pain, vomiting, diarrhea from GI mucosal swelling; may be confused with appendicitis or bowel obstruction
- Onset typically in second decade of life
- Attacks precipitated by trauma, stress, estrogen, infections
- Life-threatening - laryngeal involvement can be fatal
Clinical pearl: If HAE is unrecognized, abdominal attacks may lead to unnecessary laparotomies. Asphyxiation is the predominant cause of death.
Diagnosis: C4 is low even between attacks (screening test). During attack: low C1-INH antigen + function. C1q is low only in acquired angioedema.
Treatment of acute HAE attack:
- C1-INH concentrate (Berinert, Cinryze)
- Icatibant (bradykinin B2 receptor antagonist)
- Ecallantide (kallikrein inhibitor)
- Fresh frozen plasma (if specific agents unavailable)
- NOT epinephrine, antihistamines, or corticosteroids (ineffective)
Prophylaxis: Berotralstat (oral kallikrein inhibitor, 150 mg daily), lanadelumab (anti-kallikrein monoclonal), tranexamic acid or attenuated androgens (danazol) in long-term prophylaxis.
4C. Visceral/GI Angioedema (Acquired)
Goldman-Cecil Medicine notes that visceral angioedema can be:
- Idiopathic
- ACE inhibitor-induced (most common drug cause - bradykinin accumulation due to reduced degradation; up to 0.7% of users)
- Acquired C1-INH deficiency (associated with B-cell lymphoma, plasma cell dyscrasias)
- Food or drug-related (NSAIDs, antibiotics)
CT scan findings: thickened fluid-filled loops of small bowel + ascites. Symptoms last 1-3 days and recur episodically.
4D. Urticarial Vasculitis
A distinct entity where the urticaria is actually due to small-vessel vasculitis rather than simple mast cell degranulation.
Clinical clues:
- Wheals lasting >24 hours (ordinary urticaria resolves in <24h)
- Lesions are painful/burning rather than itchy
- Leave bruising or hyperpigmentation on resolution
- Skin biopsy: fibrinoid necrosis, endothelial damage, immune complex deposits
Hypocomplementemic Urticarial Vasculitis (HUV) - Most Severe Form:
- Associated with low C3, C4 (hypocomplementemia)
- Systemic manifestations: abdominal pain, arthralgias, COPD, glomerulonephritis, uveitis/episcleritis
- Associated with SLE and other connective tissue diseases
- Patients with hypocomplementemic HUV are significantly more likely to have abdominal pain than normocomplementemic patients
Diagnosis: Skin biopsy with direct immunofluorescence (IgG and complement deposits). Workup for SLE (ANA, anti-dsDNA, complement levels).
4E. Cholinergic Urticaria
- Triggered by: exercise, heat, emotional stress, sweating
- Small (1-3 mm) punctate wheals with larger flare
- Can cause systemic symptoms including pruritus, nausea, abdominal pain, headache
- Abdominal symptoms arise from cholinergic-mediated smooth muscle spasm and mast cell activation
- In severe/widespread cases, systemic effects predominate
4F. Systemic Mastocytosis
In mastocytosis, pathological mast cell accumulation in multiple organs (skin, bone marrow, liver, spleen, GI tract) leads to episodic mediator release.
GI manifestations (from Andrews' Diseases of the Skin):
- Urticaria pigmentosa (maculopapular cutaneous mastocytosis) on skin
- Abdominal cramps, diarrhea, nausea, vomiting
- Gastric/duodenal ulcers (excess histamine stimulates acid)
- Malabsorption
- GI hemorrhage in severe cases
Triggers of mast cell degranulation: alcohol, NSAIDs, opioids, contrast media, temperature changes, stress.
Diagnosis: Serum tryptase > 20 ng/mL suggests systemic disease; bone marrow biopsy with >25% spindle-shaped mast cells (WHO criteria); KIT D816V mutation in >95%.
4G. Physical Urticarias with Systemic Symptoms
Heat urticaria / Cholinergic urticaria: When extensive, systemic symptoms including faintness, headache, nausea, and abdominal pain occur (Dermatology 2-Volume Set, 5th ed.).
Exercise-induced anaphylaxis/urticaria: Triggers GI cramping, especially in food+exercise combined variant (alpha-gal syndrome is a recently recognized variant).
4H. Parasitic Infections
Intestinal parasites are a classic combined cause of both urticaria and abdominal pain:
- Anisakis simplex (via raw fish/sushi) - IgE-mediated allergic reaction + GI invasion
- Strongyloides, Toxocara, Echinococcus, Schistosoma, Fasciola hepatica (hepatic capsule penetration causes RUQ pain + urticaria)
- Prominent peripheral eosinophilia is an important diagnostic clue
- Stool examination indicated in travelers and those with eosinophilia
5. Diagnostic Approach
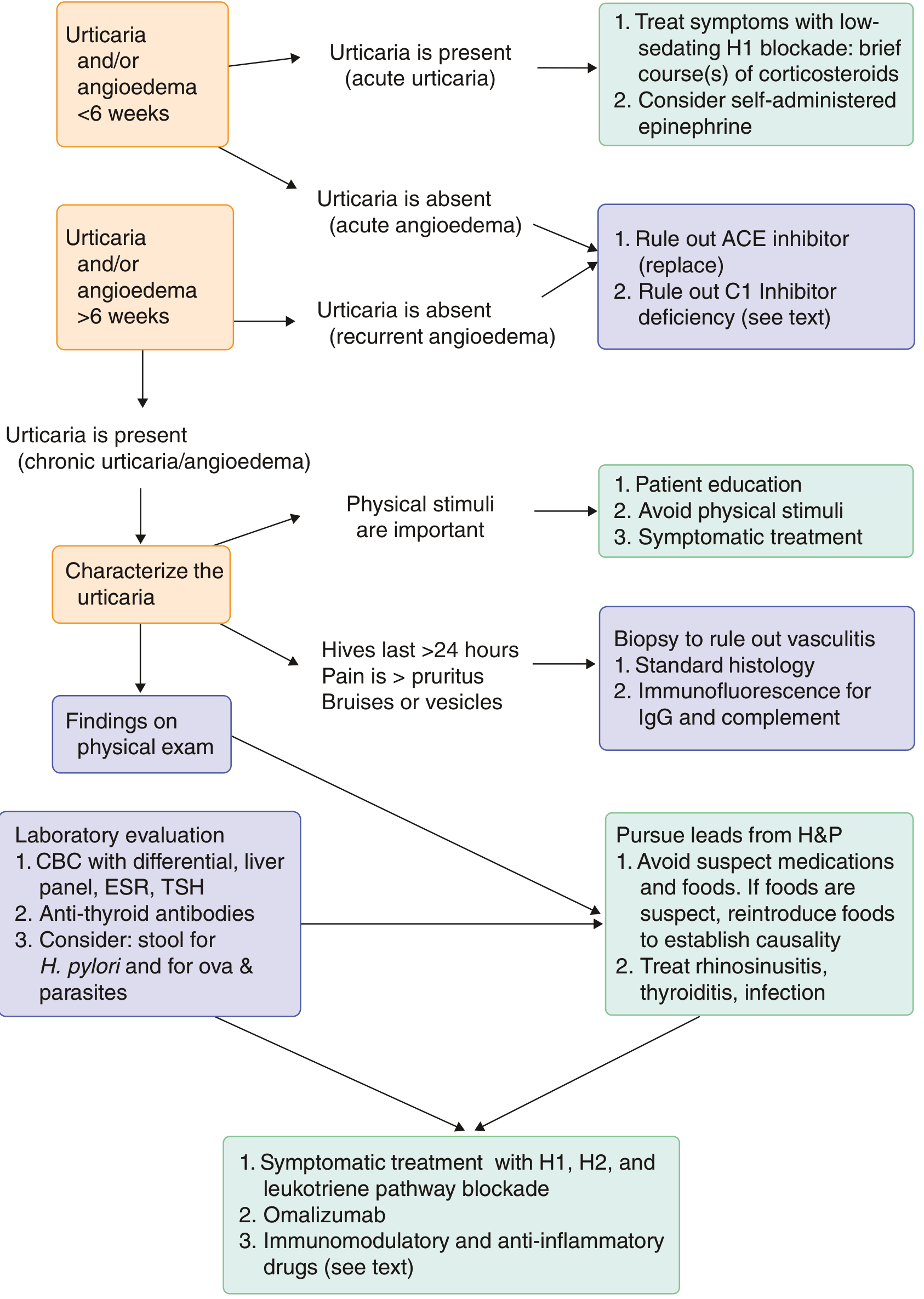
Step-by-Step Evaluation
History:
- Duration of wheals (>24 h suggests vasculitis)
- Quality of pain (itch vs. burning)
- Pattern: episodic? after specific triggers?
- Drugs (ACE inhibitors, NSAIDs, antibiotics)
- Food exposures, travel history
- Family history (HAE)
- Prior unnecessary surgeries (clue to missed HAE)
Physical Exam:
- Skin: wheal morphology, bruising, pigmentation, Darier's sign
- Look for laryngeal/tongue swelling (HAE emergency)
- Assess hemodynamic stability (anaphylaxis)
Laboratory (Goldman-Cecil Medicine, chronic urticaria):
| Test | Purpose |
|---|---|
| CBC with differential | Eosinophilia (parasites), cytopenias |
| ESR, CRP | Systemic inflammation |
| LFTs | Systemic disease |
| TSH, anti-thyroid antibodies | Thyroid autoimmunity |
| C4 level | Low in HAE (even between attacks) |
| C1-INH antigen + function | HAE diagnosis |
| C1q | Low in acquired angioedema |
| Serum tryptase | Mastocytosis, anaphylaxis |
| Stool O&P | If travel/eosinophilia |
| Skin biopsy + DIF | If vasculitis suspected |
Imaging (if abdominal symptoms severe):
- CT abdomen: thickened bowel loops, ascites, free fluid - hallmark of bowel wall angioedema
6. Treatment
6A. Acute Urticaria / Anaphylaxis
- Epinephrine 0.3-0.5 mg IM (anterolateral thigh) - first-line for anaphylaxis
- Non-sedating H1 antihistamines (cetirizine, fexofenadine, loratadine)
- Short course of corticosteroids for refractory cases
- Self-administered epinephrine auto-injector for discharge
6B. Chronic Urticaria
| Step | Treatment |
|---|---|
| Step 1 | Non-sedating H1 antihistamine (daily, not PRN) |
| Step 2 | Up-dose H1 antihistamine (up to 4x standard dose) |
| Step 3 | Add H2 blocker (ranitidine/famotidine) + leukotriene antagonist (montelukast) |
| Step 4 | Omalizumab (anti-IgE monoclonal, 150-300 mg SC monthly) |
| Step 5 | Immunomodulators (cyclosporine, mycophenolate) |
6C. Hereditary Angioedema (Bradykinin-mediated)
Do NOT use: antihistamines, corticosteroids, epinephrine (ineffective for bradykinin-mediated edema)
| Setting | Treatment |
|---|---|
| Acute attack | C1-INH concentrate, icatibant, ecallantide, or FFP |
| Short-term prophylaxis (surgery/procedures) | C1-INH concentrate or FFP |
| Long-term prophylaxis | Berotralstat (oral), lanadelumab (SC), danazol, tranexamic acid |
6D. Urticarial Vasculitis
- Normocomplementemic: antihistamines + NSAIDs (often sufficient)
- Hypocomplementemic/systemic: hydroxychloroquine, dapsone, colchicine, immunosuppressants (azathioprine, mycophenolate), or rituximab for refractory cases
6E. Mastocytosis
- Trigger avoidance
- H1 + H2 antihistamines for skin and GI symptoms
- Cromolyn sodium for GI symptoms
- Proton pump inhibitors for ulcer disease
- Midostaurin (KIT inhibitor) for advanced systemic mastocytosis
7. Summary: When to Suspect Each Diagnosis
| Presentation | Think of... |
|---|---|
| Urticaria + abdominal pain + hypotension/dyspnea after exposure | Anaphylaxis (emergency) |
| Recurrent severe abdominal pain WITHOUT hives or itch, +/- facial/laryngeal swelling | HAE (check C4) |
| Abdominal pain + urticaria on ACE inhibitor | ACE inhibitor-induced angioedema |
| Urticaria lasting >24h, painful/bruising | Urticarial vasculitis (biopsy) |
| Episodic flushing, urticaria, abdominal pain/ulcers | Systemic mastocytosis (tryptase, biopsy) |
| Abdominal pain + urticaria + eosinophilia + travel | Parasitic infection |
| Urticaria after exercise/heat/stress + abdominal pain | Cholinergic urticaria / Exercise-induced anaphylaxis |
| Urticaria + abdominal pain in SLE patient | Hypocomplementemic urticarial vasculitis |
Sources:
- Goldman-Cecil Medicine, International Edition (2-Volume Set), Ch. 232 & 235
- Dermatology 2-Volume Set, 5th ed. (Bolognia), Ch. 18
- Rosen's Emergency Medicine: Concepts and Clinical Practice, Ch. 107
- Tietz Textbook of Laboratory Medicine, 7th ed., Ch. on Hereditary Angioedema
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Ch. on Visceral Angioedema
- Goodman & Gilman's Pharmacological Basis of Therapeutics (Berotralstat)
- Andrews' Diseases of the Skin, Ch. 8
This is a shared conversation. Sign in to Orris to start your own chat.