Nerve supply of pinna, external auditory canal, middle ear, inner ear explain in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks (Gray's Anatomy for Students, Histology: A Text and Atlas, Shambaugh Surgery of the Ear, Scott-Brown's Otorhinolaryngology, Cummings Otolaryngology, and Miller's Anesthesia) along with two excellent anatomical diagrams. I have enough for a thorough, well-structured answer.
Nerve Supply of the Ear: Detailed Account
The ear is divided into four anatomical compartments - pinna (auricle), external auditory canal (EAC), middle ear, and inner ear - each with a distinct and overlapping nerve supply.
1. Pinna (Auricle)
The pinna receives a rich and complex sensory innervation from five nerves spanning the trigeminal system, cervical plexus, and vagus nerve. The muscles of the auricle (both intrinsic and extrinsic) are all motor-supplied by the facial nerve (CN VII).
Sensory Nerves
| Nerve | Origin | Area Supplied |
|---|---|---|
| Auriculotemporal nerve | CN V3 (mandibular branch of trigeminal) | Superior two-thirds of anterior surface |
| Great auricular nerve | C2, C3 (cervical plexus) | Posterior surface, lower third of anterior surface, lobule |
| Lesser occipital nerve | C2, C3 (cervical plexus) | Upper part of the earlobe, lateral occipital zone |
| Auricular branch of vagus (Arnold's nerve) | CN X | Concha, posterior wall of EAC (Ramsay Hunt zone) |
| Facial nerve (CN VII) | CN VII | Small area of skin (concha/cymba) |
Auriculotemporal nerve (V3): This is the dominant nerve of the anterior pinna. It passes through the parotid gland and ascends anterior to the auditory canal with the superficial temporal artery, passing superficial to the zygomatic arch. It covers the superior two-thirds of the anterior (lateral) surface of the pinna.
Great auricular nerve (C2, C3): Arises from the second and third cervical roots, emerges from the posterior border of the sternocleidomastoid muscle, and ascends (dividing into anterior and posterior branches) toward the mandible, parotid gland, and pinna. It supplies the lower back of the auricle, the lobule, and the skin of the angle of the mandible.
Lesser occipital nerve (C2, C3): Arises from the ventral primary rami of C2 and C3, and supplies the upper part of the earlobe and the lateral occipital zone.
Arnold's nerve (auricular branch of vagus, CN X): This nerve passes behind the internal jugular vein and enters the mastoid canaliculus on the lateral wall of the jugular foramen. It emerges via the tympanomastoid fissure to supply the concha and posterior wall of the EAC. This is the basis of the Ramsay Hunt syndrome zone - herpes zoster reactivation in the geniculate ganglion causes vesicles in this distribution.
Miller's Anesthesia, 10e, p.11040; Scott-Brown's Otorhinolaryngology Vol 2, p.1666
2. External Auditory Canal (EAC)
The EAC (approximately 24 mm long, outer one-third cartilaginous, inner two-thirds bony) has a partially overlapping nerve supply:
Sensory Nerves
| Nerve | Area Supplied |
|---|---|
| Auriculotemporal nerve (CN V3) | Anterior and superior walls (especially cartilaginous part) |
| Auricular branch of vagus - Arnold's nerve (CN X) | Posterior wall and floor (bony part especially) |
| Facial nerve (CN VII) | Small contribution to posterior EAC (via posterior auricular branch) |
Auriculotemporal nerve (V3): The mandibular branch of CN V supplies the anterior and superior EAC skin. This is clinically relevant - referred otalgia from TMJ disorders and dental pathology travels via this nerve.
Arnold's nerve (CN X): Supplies the posterior and inferior walls of the EAC, especially the bony portion. Stimulation of this nerve explains the ear-cough reflex (Arnold's reflex) - coughing triggered by ear syringing or instrumentation of the posterior EAC wall. It also explains why cardiac and esophageal pathology can refer pain to the ear (referred otalgia via CN X). The Hitselberger sign (hypoesthesia of the posterior EAC due to CN X compression) is an early sign of acoustic neuroma.
Facial nerve (CN VII): A small sensory contribution via the posterior auricular nerve supplies the skin of the posterior EAC and adjacent concha.
Scott-Brown's Otorhinolaryngology Vol 2, p.1662-1666; Roberts and Hedges' Clinical Procedures, p.32-38
3. Middle Ear
The middle ear is innervated primarily through the tympanic plexus, which sits on the promontory of the medial wall.
Tympanic Plexus - Composition
The tympanic plexus is formed by two sources:
1. Tympanic nerve (Jacobson's nerve) - CN IX branch:
- Arises from the glossopharyngeal nerve (CN IX) at the petrous (inferior) ganglion after CN IX exits the skull through the jugular foramen
- Passes through the inferior tympanic canaliculus (a small canal in the keel of the petrous bone, between the jugular and carotid foramina) to enter the middle ear
- Runs over the promontory of the cochlea, forming the tympanic plexus
2. Caroticotympanic nerves:
- Sympathetic branches from the plexus surrounding the internal carotid artery
- Enter the middle ear through small canaliculi
What the Tympanic Plexus Supplies
The tympanic plexus supplies the mucous membrane lining:
- All walls and contents of the middle ear cavity
- The mastoid air cells and antrum
- The pharyngotympanic (Eustachian) tube mucosa
Muscles of the Middle Ear - Motor Supply
| Muscle | Motor Nerve |
|---|---|
| Tensor tympani | Branch from mandibular nerve (V3) via medial pterygoid nerve |
| Stapedius | Branch of facial nerve (CN VII) |
Continuation - Lesser Petrosal Nerve
The tympanic plexus gives off the lesser petrosal nerve, which carries preganglionic parasympathetic fibers originally from the inferior salivatory nucleus (via CN IX). The lesser petrosal nerve:
- Leaves the promontory area
- Travels through the petrous temporal bone
- Exits onto the anterior surface of the petrous bone through the hiatus for the lesser petrosal nerve (just inferior to the hiatus for the greater petrosal nerve)
- Traverses the middle cranial fossa diagonally
- Exits through the foramen ovale to reach the otic ganglion, where it synapses
- Postganglionic fibers travel via the auriculotemporal nerve to supply the parotid gland
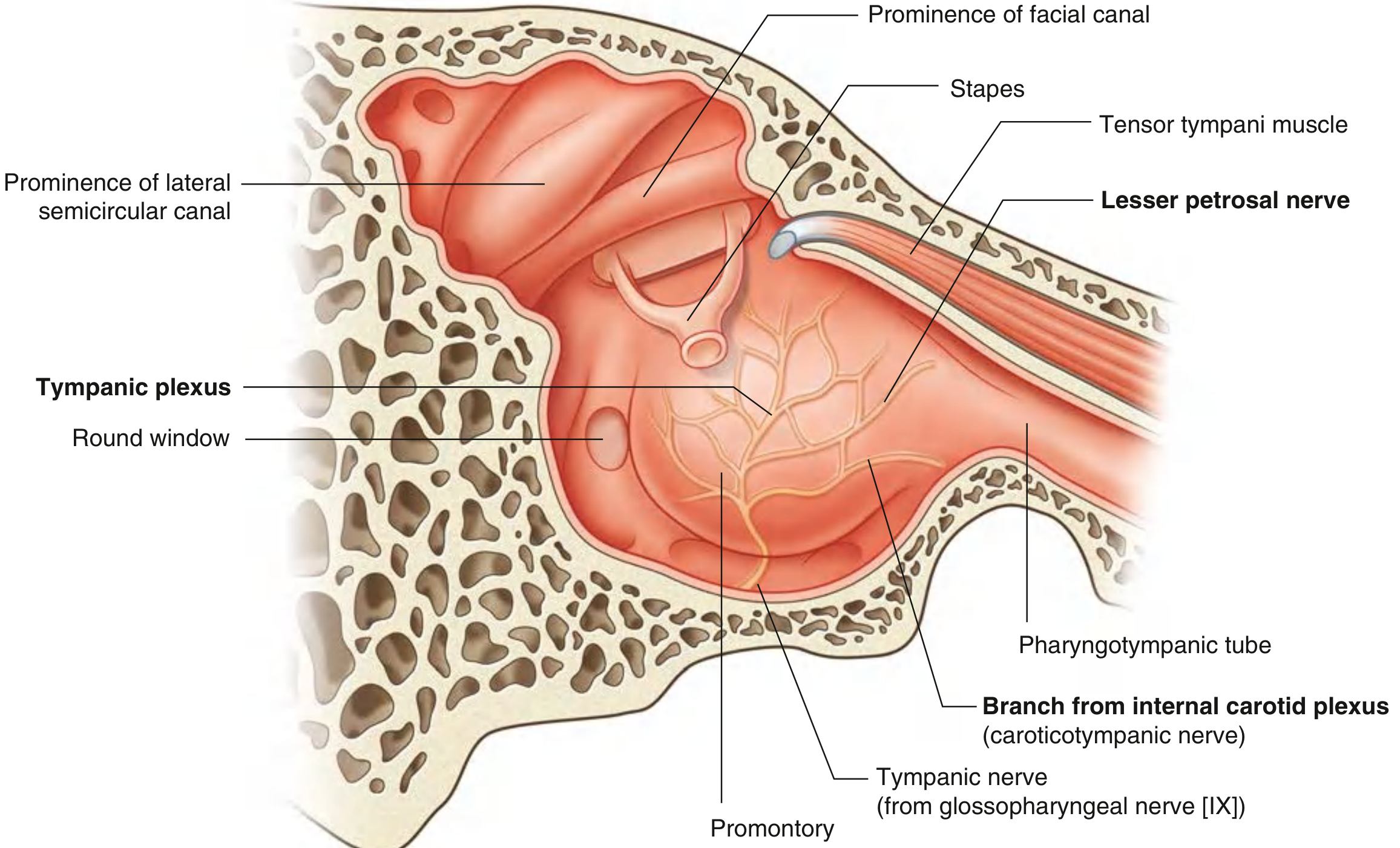
Fig. Innervation of the middle ear showing the tympanic plexus on the promontory, tympanic nerve from CN IX, caroticotympanic nerve from the internal carotid plexus, and the lesser petrosal nerve. - Gray's Anatomy for Students
Gray's Anatomy for Students, p.1103-1104; Scott-Brown's Otorhinolaryngology Vol 2, p.1656-1660; Cummings Otolaryngology, p.1849
4. Inner Ear
The inner ear is exclusively innervated by the vestibulocochlear nerve (CN VIII), which divides into two functional divisions after entering the internal acoustic meatus (IAM).
CN VIII Divisions
A. Cochlear Nerve (Hearing)
- Carries impulses from the spiral organ of Corti in the cochlear duct
- Cell bodies of the bipolar neurons are located in the spiral ganglion of Corti within the modiolus (central bony column of the cochlea)
- ~90% of dendrites synapse with inner hair cells; remaining ~10% synapse with outer hair cells
- Axons of spiral ganglion cells form the cochlear nerve, travel through the modiolus, emerge at the base of the cochlea (fundus of IAM), and enter the brainstem
- Terminate in the dorsal and ventral cochlear nuclei of the medulla oblongata
- Secondary fibers cross to the contralateral side and travel via the lateral lemniscus to the inferior colliculus, then to the medial geniculate nucleus of the thalamus, and finally to the primary auditory cortex (Heschl's gyri, temporal lobe)
B. Vestibular Nerve (Balance)
- Carries impulses from the vestibular labyrinth
- Cell bodies are in the vestibular ganglion (of Scarpa) located in the IAM
- Dendritic processes originate from:
- Cristae ampullares of the three semicircular ducts (anterior, posterior, lateral) - detect rotational acceleration
- Macula of the utricle - detects horizontal linear acceleration and gravity
- Macula of the saccule - detects vertical linear acceleration
- They synapse at the base of vestibular hair cells: as a chalice (calyx) around type I hair cells or as a bouton on type II hair cells
- Axons terminate in four vestibular nuclei (superior, inferior, medial, lateral) in the medulla/pons
- Secondary fibers project to the cerebellum, and to CN III/IV/VI nuclei (vestibulo-ocular reflex)
C. Efferent Olivocochlear Tract (Rasmussen's bundle)
A small number of efferent fibers from the superior olivary complex travel alongside the afferent CN VIII fibers (olivocochlear tract / cochlear efferents of Rasmussen). These efferent fibers:
- Synapse on afferent endings beneath inner hair cells, or directly on the basal aspect of outer hair cells
- Thought to modulate the sensitivity of the cochlea (noise protection, attention mechanisms)
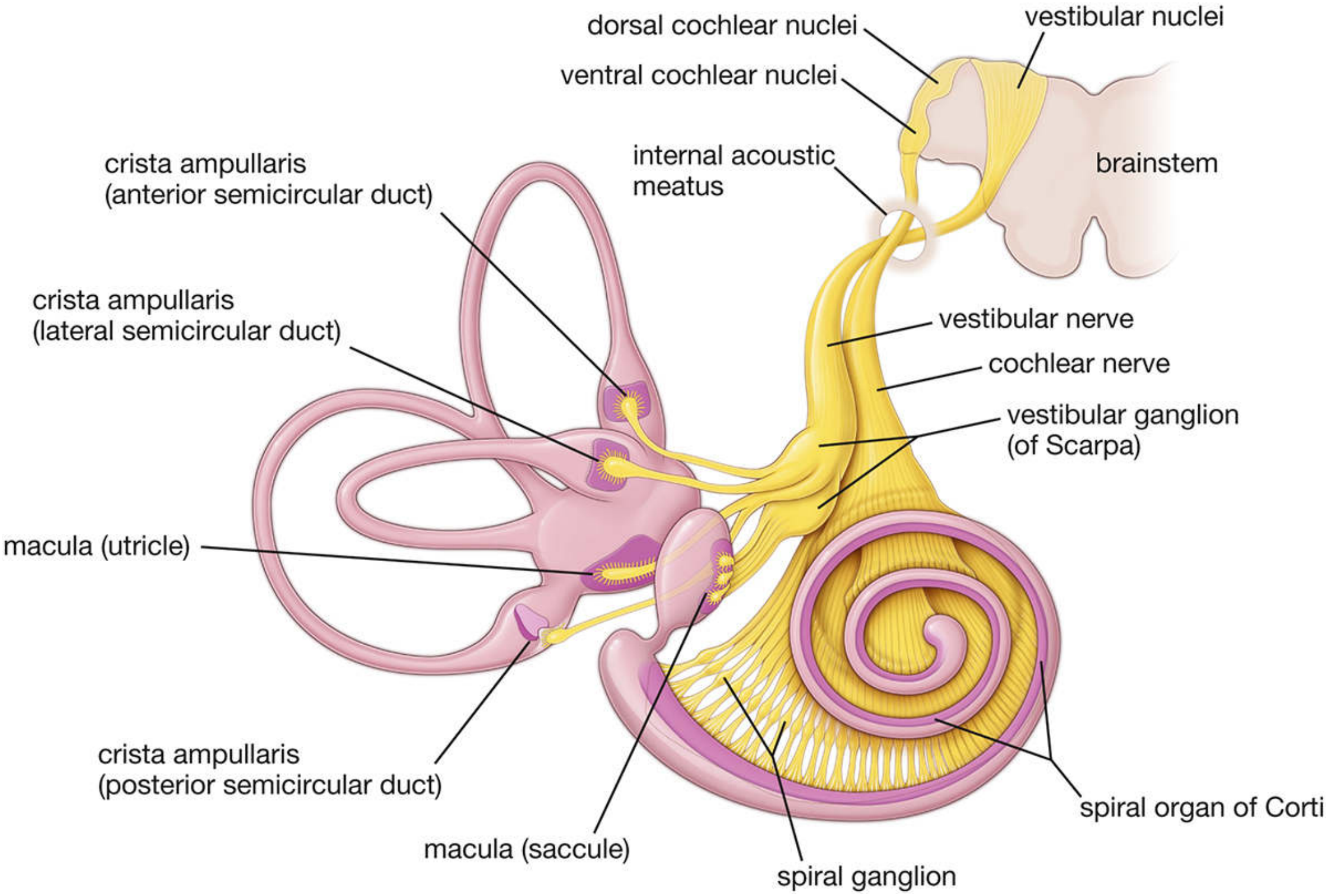
Fig. Innervation of the membranous labyrinth. The cochlear nerve arises from the spiral ganglion supplying the organ of Corti; the vestibular nerve arises from the vestibular ganglion (of Scarpa) supplying the three cristae ampullares and the maculae of the utricle and saccule. Both join to form CN VIII. - Histology: A Text and Atlas
Histology: A Text and Atlas (Pawlina), p.2510-2511; Gray's Anatomy for Students, p.1105-1107
Clinical Correlations at a Glance
| Clinical Scenario | Nerve Involved | Mechanism |
|---|---|---|
| Ramsay Hunt syndrome | CN VII (geniculate ganglion) with Arnold's nerve (CN X) territory vesicles | VZV reactivation in geniculate ganglion - vesicles in concha/EAC |
| Referred otalgia from tonsil/tongue base | CN IX (Jacobson's nerve) | Same nerve supplies middle ear and posterior oropharynx |
| Referred otalgia from dental/TMJ | CN V3 (auriculotemporal) | Same nerve supplies anterior EAC and teeth/TMJ |
| Referred otalgia from larynx/esophagus | CN X (Arnold's nerve) | Same nerve supplies posterior EAC and larynx |
| Arnold's ear-cough reflex | CN X | Stimulation of posterior EAC triggers cough via vagal reflex |
| Hitselberger's sign | CN X in EAC | Acoustic neuroma compresses CN X in IAM; hypoesthesia in posterior EAC |
| Sensorineural hearing loss | Cochlear nerve / spiral ganglion | Cochlear nerve damage from noise, ototoxins, aging |
| Vertigo | Vestibular nerve | Superior vestibular neuritis (anterior + lateral semicircular canals) vs inferior (posterior SCC + saccule) |
Sources:
- Gray's Anatomy for Students, 4th ed., pp. 1103-1107
- Histology: A Text and Atlas (Pawlina), pp. 2510-2511
- Miller's Anesthesia, 10e, pp. 11040-11041
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2, pp. 1655-1666
- Shambaugh Surgery of the Ear, pp. 421-422
- Cummings Otolaryngology Head and Neck Surgery, p. 1849
https://youtu.be/HVfVoQeqCWk?si=hCuVrQrzKlpnWvQY
analyse_media
The video couldn't be fully played due to YouTube's bot-protection check, but enough metadata was extracted to give you a useful summary.
Video Details
- Title: Ophthalmology Complete Marking
- Channel: Learn MBBS
- Uploaded: April 3, 2021
- Views: ~20,786
What This Video Is About
This is an exam-oriented "marking" guide for the Ophthalmology subject in the MBBS curriculum (typically Phase 3 / 3rd Year). "Marking" videos are a popular study format among South Asian medical students where an educator goes through a standard ophthalmology textbook (such as Parsons' Diseases of the Eye or Khurana's Comprehensive Ophthalmology) and highlights:
- High-yield topics - chapters and concepts most frequently asked in university written exams and viva
- Syllabus prioritization - what to read in detail, what to skim, and what to skip to optimize study time
- Important diagrams - key anatomical drawings students must know (e.g., layers of the cornea, visual pathway, aqueous humor circulation)
- Core pathology - standard exam topics like Cataract, Glaucoma, Corneal ulcers, Refractive errors, Retinal detachment, and Squint
How to Use It
If you're studying Ophthalmology for your MBBS exams, this kind of video is best used as a study roadmap - watch it alongside your textbook to know which sections to focus on. If you'd like, I can help you with any specific Ophthalmology topic covered in the curriculum.
This is a shared conversation. Sign in to Orris to start your own chat.