Neuro muscler junction 6 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a thorough 6-mark answer. Here is the complete, exam-ready response:
Neuromuscular Junction (NMJ)
Definition
The neuromuscular junction (NMJ), also called the motor end plate, is the specialized chemical synapse between the terminal of a lower motor neuron (alpha motor neuron) and a skeletal muscle fibre. It converts an electrical nerve impulse into a chemical signal that triggers muscle contraction.
Structure
The NMJ has three main components:
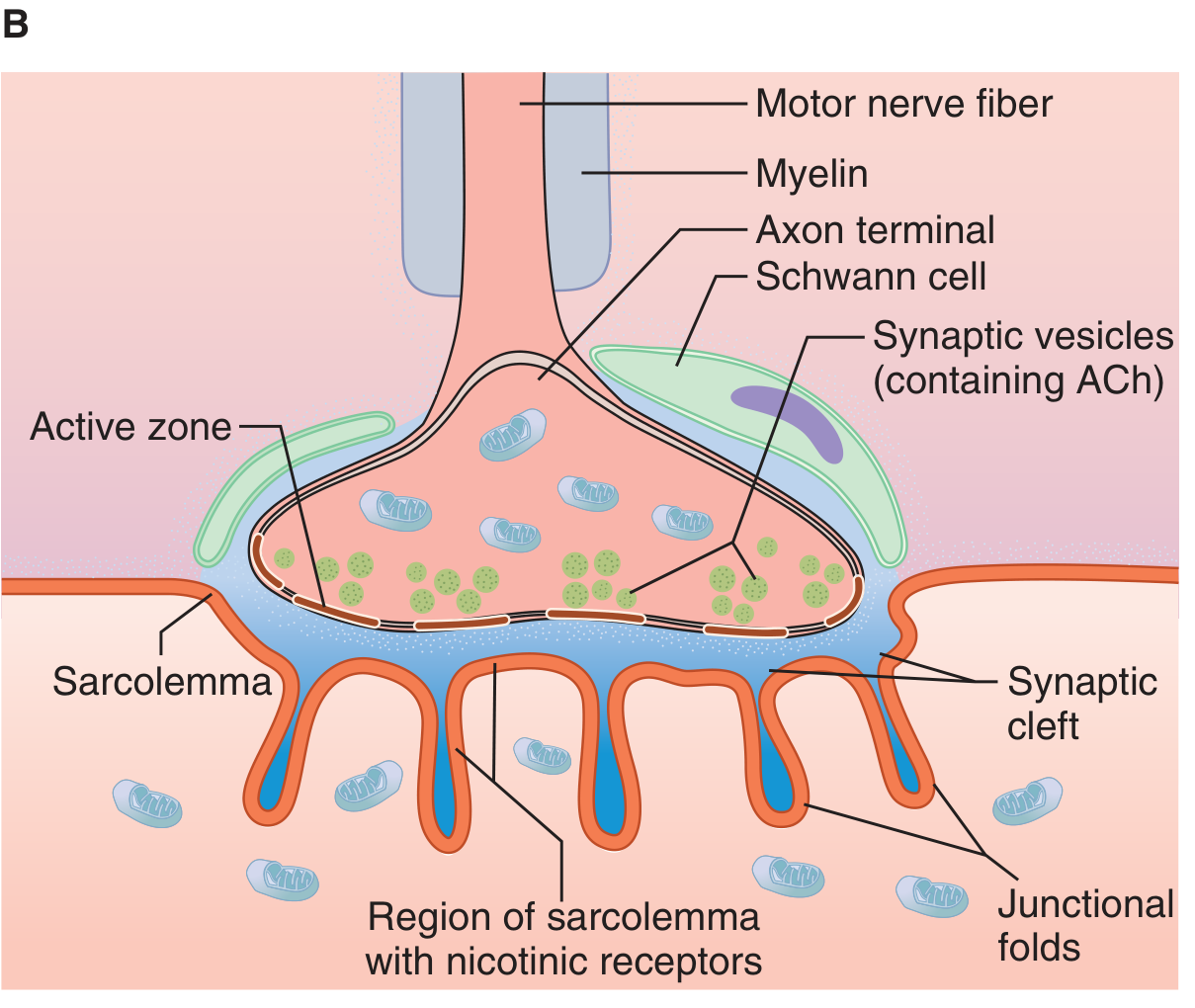
1. Presynaptic (nerve) terminal
- The myelinated motor axon loses its myelin sheath near the muscle and divides into terminal boutons (knob-like endings)
- Each bouton contains ~300,000 synaptic vesicles, each packed with acetylcholine (ACh)
- Dense bars on the inner neural membrane flank voltage-gated Ca²⁺ channels - these are the active zones for vesicle docking and exocytosis
- Numerous mitochondria supply ATP for ACh synthesis
2. Synaptic cleft
- 20-30 nm wide space between nerve terminal and muscle membrane
- Contains the enzyme acetylcholinesterase (AChE), embedded in a collagen matrix, which rapidly degrades ACh
3. Postsynaptic (muscle) membrane - Motor End Plate
- The muscle membrane here (sarcolemma) is thickened and thrown into junctional (subneural) folds, greatly increasing surface area
- Nicotinic ACh receptors (nAChRs) are densely concentrated at the crests of these folds, directly opposite the active zones
- Voltage-gated Na⁺ channels are concentrated deeper in the folds
Each motor axon innervates several muscle fibres forming a motor unit; each muscle fibre receives input from only one nerve terminal.
Nicotinic ACh Receptor Structure
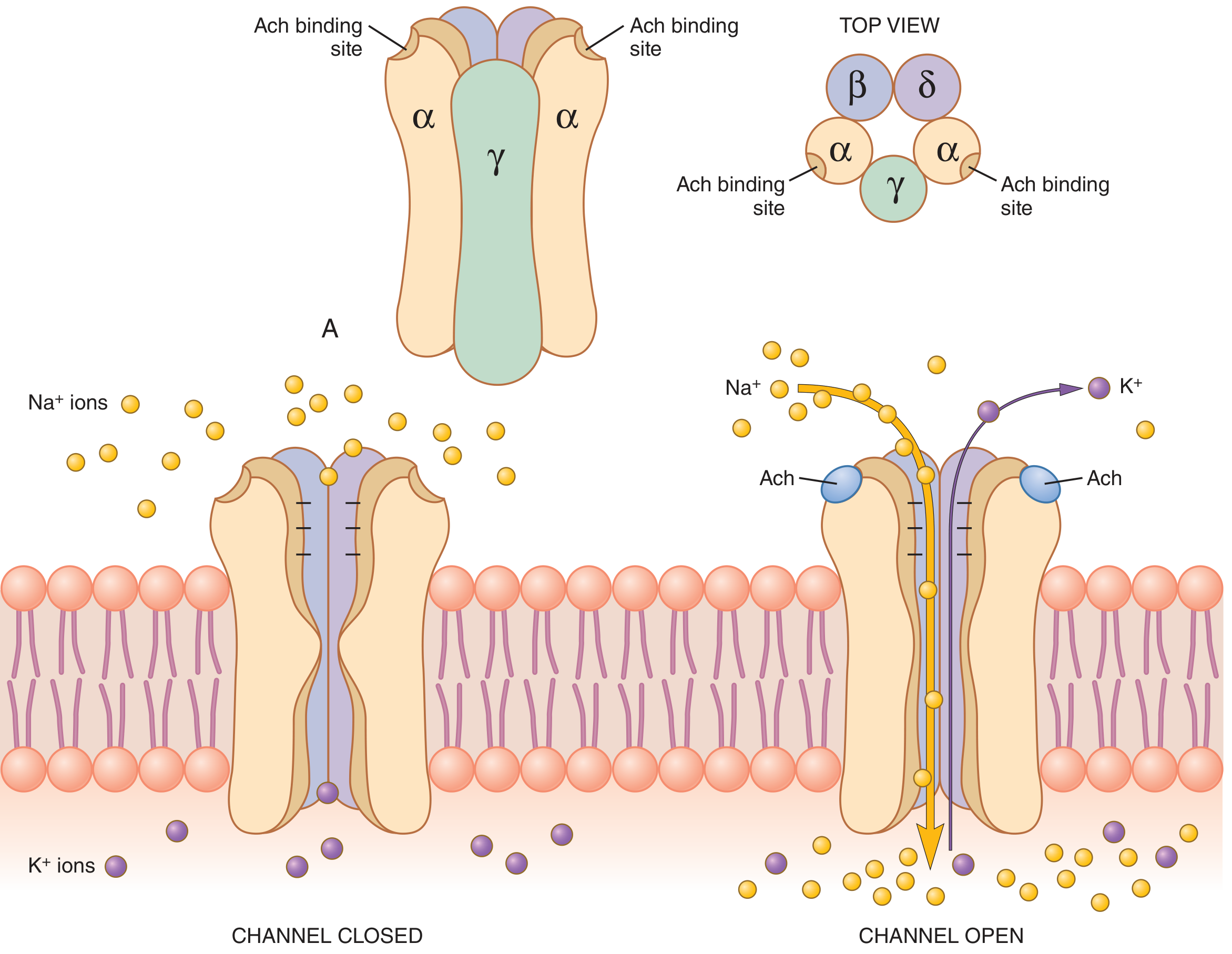
The nAChR is a pentameric ligand-gated ion channel with molecular weight ~275,000 Da:
- Subunits: 2α + 1β + 1δ + 1γ (fetal) or 1ε (adult) arranged around a central pore
- ACh binds simultaneously to both α subunits, causing a conformational change that opens the channel (~0.65 nm diameter)
- The open channel allows Na⁺, K⁺, and Ca²⁺ to pass; negatively charged channel mouth repels Cl⁻
- Net effect: large inward Na⁺ current (Na⁺ electrochemical driving force ~160 mV inward vs. K⁺ ~10 mV outward) → depolarisation
Sequence of Events at Transmission
| Step | Event |
|---|---|
| 1 | Action potential arrives at axon terminal |
| 2 | Voltage-gated Ca²⁺ channels open → Ca²⁺ influx |
| 3 | Ca²⁺ activates Ca²⁺-calmodulin kinase → phosphorylates synapsin proteins → vesicles freed from cytoskeleton |
| 4 | ~125 vesicles dock at active zones and undergo exocytosis → ACh released into synaptic cleft |
| 5 | ACh diffuses to nAChRs on junctional folds |
| 6 | Binding of 2 ACh molecules opens the ion channel → Na⁺ influx → End Plate Potential (EPP) of +50 to +75 mV |
| 7 | EPP depolarises adjacent muscle membrane beyond threshold → muscle action potential → muscle contraction |
| 8 | AChE rapidly hydrolyses ACh → choline is recycled back into the terminal for ACh re-synthesis |
End Plate Potential (EPP)
- A local graded depolarisation generated at the motor end plate
- Not propagated; it is always suprathreshold under normal conditions (the NMJ has a safety factor of ~3x - the EPP generated is approximately 3 times the minimum needed to fire an action potential)
- Subthreshold EPPs are produced by curare (competitive nAChR blocker) or botulinum toxin (blocks ACh release)
Safety Factor & Fatigue
- Under normal conditions, each nerve impulse produces ~3× the minimum EPP needed, ensuring reliable transmission
- At very high stimulation rates (>100/s for several minutes), ACh vesicle depletion can cause fatigue - impulses may fail to propagate to the muscle
- In normal activity, measurable NMJ fatigue is rare
Termination of ACh Action
AChE in the synaptic cleft hydrolyses ACh within a few milliseconds into choline + acetate:
- Prevents re-excitation of the muscle after each action potential
- Choline is actively re-taken up by the nerve terminal and used to re-synthesise ACh (via choline acetyltransferase + acetyl-CoA)
Clinical Relevance
| Condition | Mechanism |
|---|---|
| Myasthenia Gravis | Autoantibodies against postsynaptic nAChRs → reduced EPP → fatigable weakness |
| Lambert-Eaton Syndrome | Autoantibodies against presynaptic voltage-gated Ca²⁺ channels → reduced ACh release |
| Botulinum toxin | Cleaves SNARE proteins → blocks vesicle fusion → no ACh release → flaccid paralysis |
| Organophosphate poisoning | Inhibit AChE → ACh accumulation → sustained depolarisation → paralysis + cholinergic crisis |
| Curare / Non-depolarising NMBDs | Competitive nAChR blockade → no EPP |
| Succinylcholine (depolarising NMBD) | Persistent nAChR activation → phase I depolarising block |
Sources: Ganong's Review of Medical Physiology, 26th Ed. | Guyton & Hall Textbook of Medical Physiology | Boron & Boulpaep Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.