I have my university exam of 1 st year of subject biochemistry These are the important question give me answer of this "Albinism" and remeber it's a university examination The answer should be easy to memorize and follow the pattern of answer writing as in University paper
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I have all the material needed. Here is your complete, exam-ready university answer on Albinism:
ALBINISM
Definition
Albinism is a group of inherited metabolic disorders characterized by a defect in tyrosine metabolism, resulting in partial or complete absence of melanin pigment from the skin, hair, and eyes.
Biochemical Basis
Melanin is the dark pigment normally synthesized in melanocytes from the amino acid tyrosine. The key enzyme responsible is tyrosinase (a copper-dependent enzyme), which catalyzes the first two steps in melanin synthesis:
Tyrosine →(Tyrosinase)→ DOPA →(Tyrosinase)→ DOPAquinone →→ Melanin
In albinism, tyrosinase is absent or defective, so this pathway is blocked and melanin cannot be formed. The melanocytes are present in normal numbers but fail to produce pigment.
Metabolic Pathway Diagram:
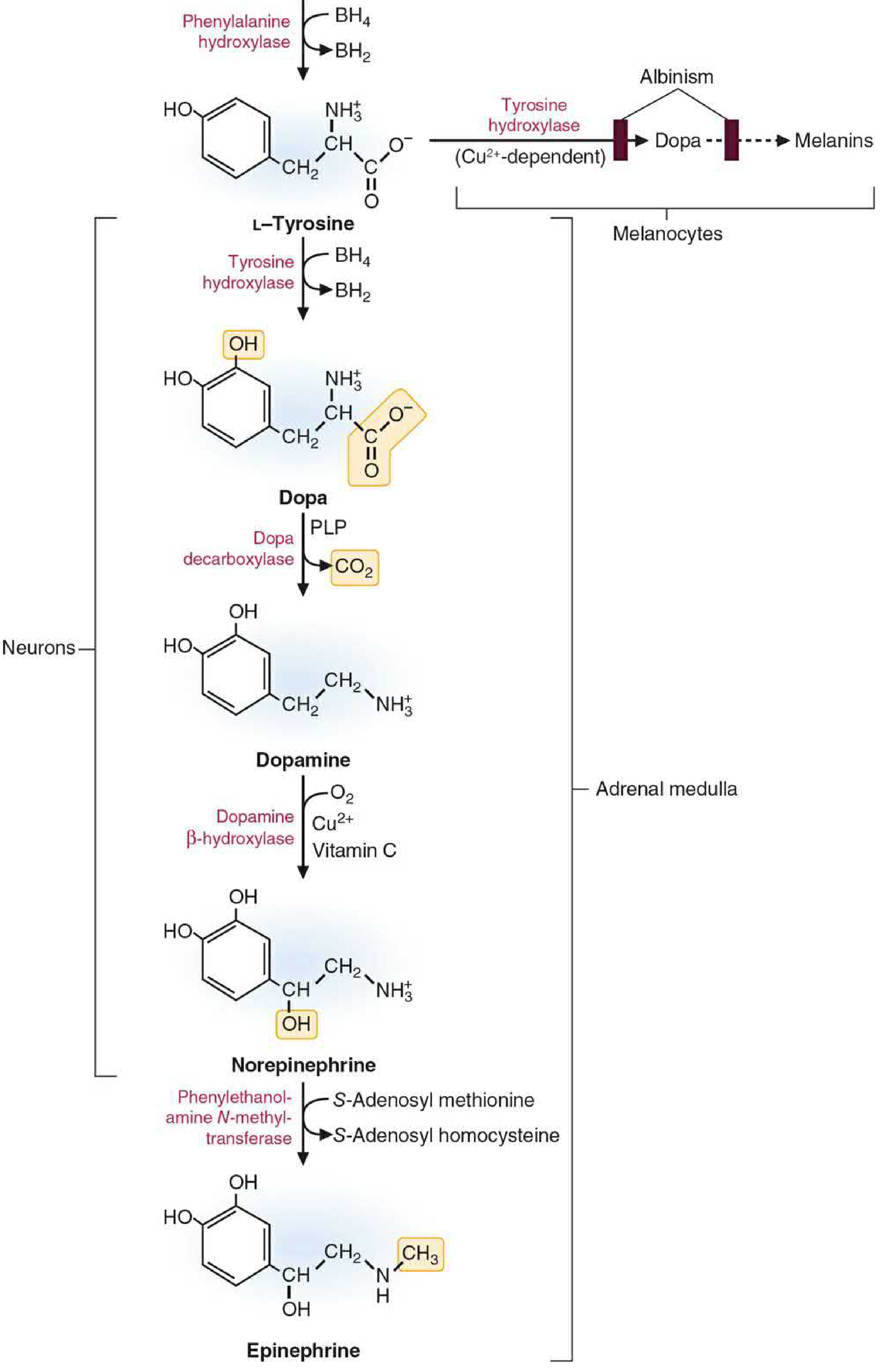
Note: The dark boxes in the diagram show the enzymes that, when defective, lead to albinism.
Genetics / Inheritance
| Feature | Details |
|---|---|
| Primary mode | Autosomal Recessive (AR) |
| Other modes | Autosomal Dominant, X-linked (rare) |
| Gene affected | TYR gene (encodes tyrosinase) - most common |
| Prevalence | ~1 in 17,000 (varies by type and population) |
Types of Albinism
1. Oculocutaneous Albinism (OCA) - Most Common
Affects skin + hair + eyes
| Type | Enzyme Status | Features |
|---|---|---|
| OCA Type 1A (Tyrosinase-negative) | Tyrosinase completely absent | Most severe; white hair, white skin, blue/pink eyes - lifelong, no tanning |
| OCA Type 1B (Yellow mutant) | Tyrosinase greatly reduced | Some pigment may develop with age; can tan slightly |
| OCA Type 2 (Tyrosinase-positive) | Tyrosinase present but OCA2 gene mutated | Most common worldwide (~50% of OCA); pigment present at birth, may increase with age |
2. Ocular Albinism (OA)
- Only the eyes are affected; skin and hair appear normal
- X-linked inheritance (primarily affects males)
Clinical Features
A. Skin:
- Milky white or very pale skin
- Does not tan
- Highly sensitive to sunlight (photosensitive)
- Increased risk of skin cancer (squamous cell carcinoma, basal cell carcinoma, melanoma)
B. Hair:
- White or light yellow hair
- White eyebrows and eyelashes
C. Eyes (Ocular Features):
- Photophobia (sensitivity to light) - due to lack of iris pigment
- Nystagmus (involuntary rhythmic eye movements)
- Strabismus (squint)
- Reduced visual acuity (vision 20/200 to 20/400 in severe cases)
- Iris translucency - irises appear light blue or pink/red (due to underlying blood vessels showing through)
- Foveal hypoplasia (underdevelopment of fovea)
Clinical Photo:

Patient showing characteristic red irises and white eyebrows/lashes in OCA
Pathophysiology (Why These Features Occur)
| Feature | Reason |
|---|---|
| White skin/hair | No melanin synthesized by melanocytes |
| Red/pink eyes | Blood vessels of choroid visible through unpigmented iris |
| Photophobia | Iris cannot filter light without pigment |
| Nystagmus | Abnormal routing of optic nerve fibers at chiasm (due to lack of retinal melanin during development) |
| Skin cancer risk | Melanin normally protects against UV radiation; its absence leaves DNA unprotected |
Diagnosis
- Clinical examination - skin, hair, and eye inspection
- Hair bulb tyrosinase test - incubate hair bulbs in tyrosine; color change = tyrosinase-positive; no color = tyrosinase-negative
- Molecular genetic testing - gene mutation analysis (TYR gene)
- Ophthalmological assessment - nystagmus, visual acuity, foveal hypoplasia
Treatment / Management
There is no cure for albinism. Management is supportive:
- Sun protection - sunscreen (SPF 30+), protective clothing, hats, sun avoidance
- Vitamin D supplementation - required because sun avoidance limits natural synthesis
- Corrective lenses - for refractive errors and to improve visual acuity
- Low vision aids - magnifiers, tinted lenses for photophobia
- Strabismus - may be corrected surgically
- Regular skin screening - for early detection of skin cancer
- Genetic counseling - for affected individuals and families
Key Points to Remember (Memory Aid)
- Enzyme defect: Tyrosinase (copper-dependent)
- Metabolic block: Tyrosine → DOPA (first step blocked)
- Inheritance: Autosomal Recessive (main mode)
- Triad of features: White skin + White hair + Ocular problems
- 3 eye features: Photophobia + Nystagmus + Reduced visual acuity
- Major complication: Skin cancer (UV damage due to absent melanin)
- No treatment exists for the enzyme defect; management is only supportive
Sources: Lippincott Illustrated Reviews: Biochemistry 8th ed., p. 769 | Andrews' Diseases of the Skin, Clinical Dermatology | Emery's Elements of Medical Genetics and Genomics
This is a shared conversation. Sign in to Orris to start your own chat.