Disease Representation Diagram
Patient: Mr. Anil Kumar | 44 yrs | Male | CECT Abdomen | 22 Jun 2026 | Medanta
FINDINGS & TREATMENT PLAN
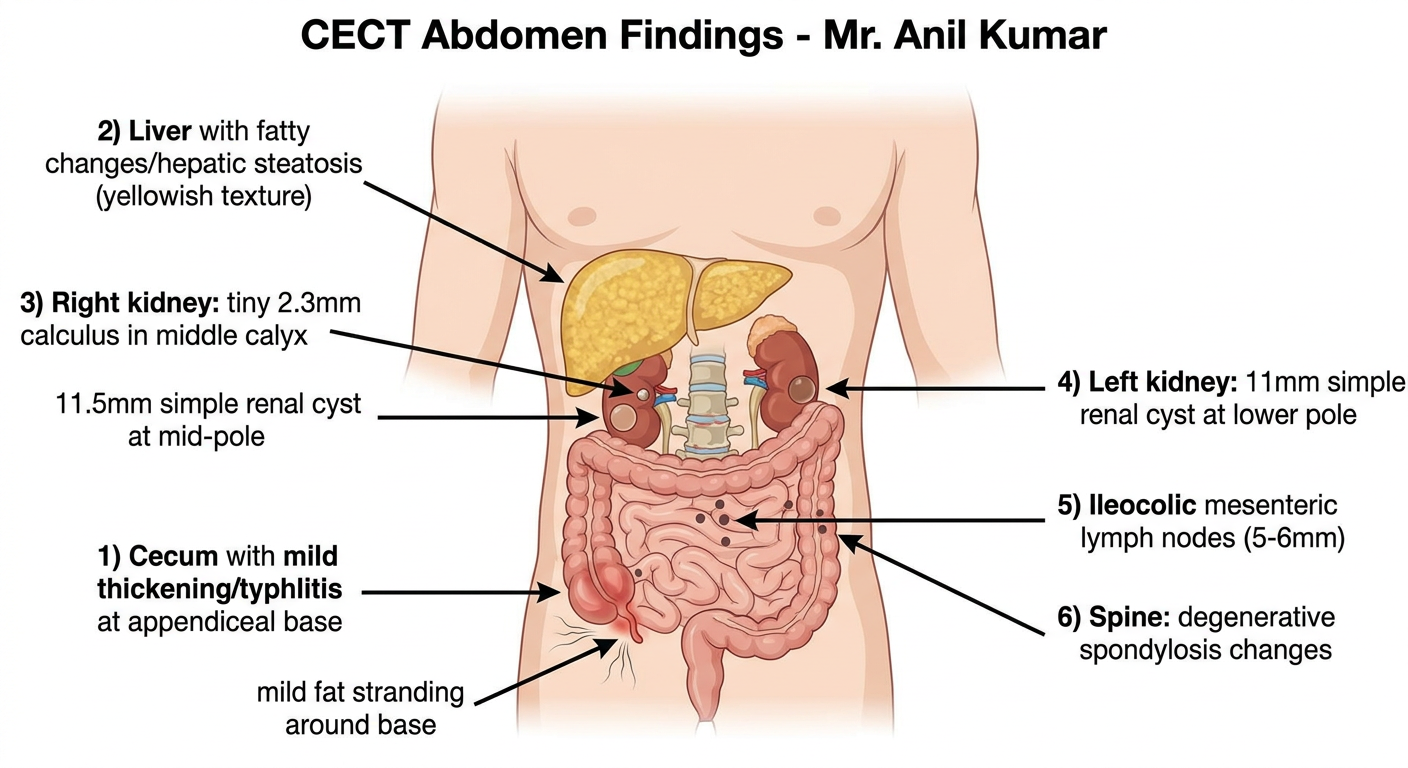
FINDING 1 - Mild Typhlitis (Cecal Inflammation)
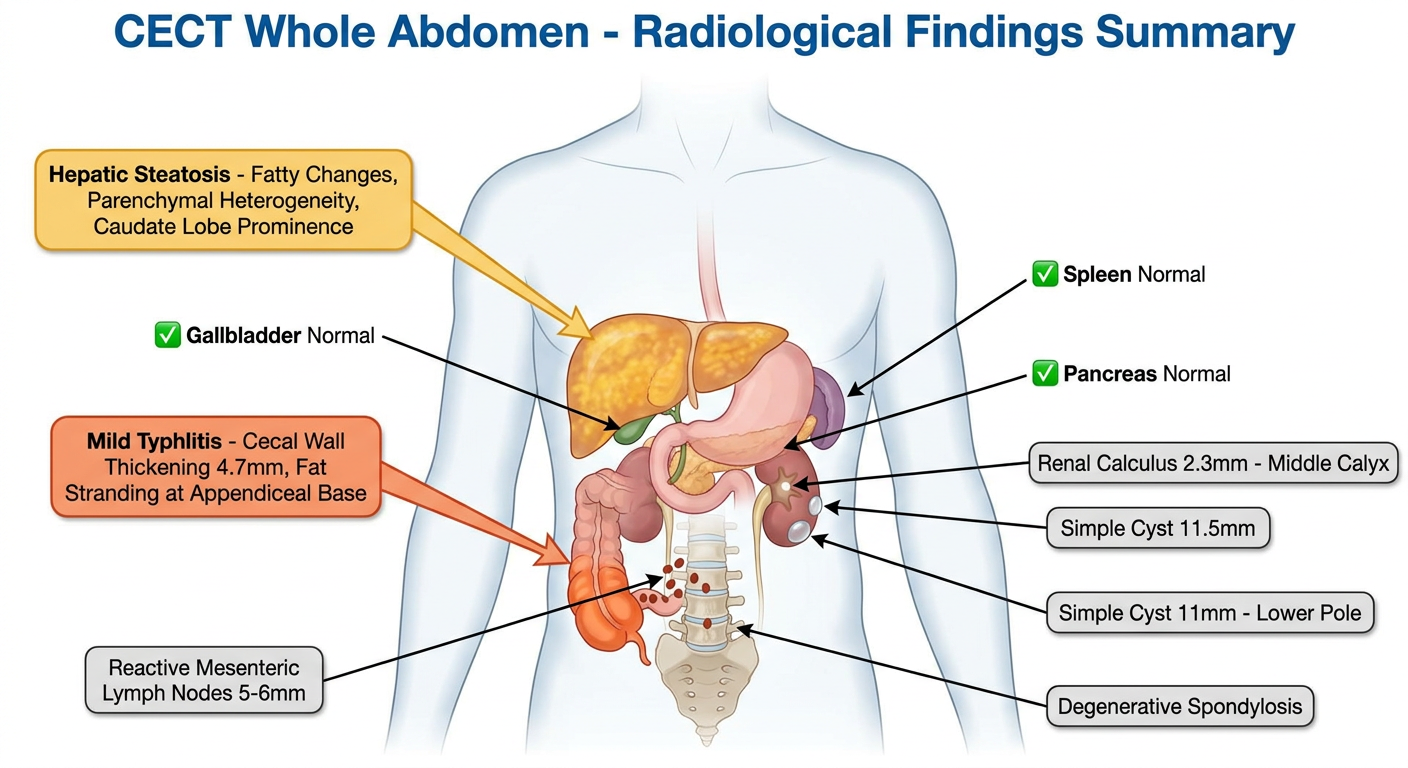
CT Finding: Mild symmetrical cecal wall thickening extending to appendiceal base (4.7mm), fat stranding around base, rest of appendix undefined. Possible mild typhlitis. Ileocolic mesenteric lymph nodes 5-6mm (reactive).
Disease Explanation:
Typhlitis is inflammation of the cecum (the pouch at the start of the large intestine). In this patient, it is a non-neutropenic, mild form - likely infectious or inflammatory in origin rather than chemotherapy-related. The fat stranding means inflammation is spreading into surrounding fatty tissue. The radiologist has rightly asked for correlation with previous surgical history (prior appendectomy?).
Treatment:
| Recommendation |
|---|
| Antibiotics | Tab. Amoxicillin-Clavulanate 625mg three times daily x 7 days OR Ciprofloxacin 500mg twice daily + Metronidazole 400mg three times daily x 7 days |
| Diet | Soft, low-fibre diet during active inflammation. Avoid raw vegetables, spicy food |
| Hydration | 2-3 litres of oral fluids per day |
| Analgesics | Tab. Paracetamol 500mg as needed for pain (avoid NSAIDs initially) |
| Probiotics | Saccharomyces boulardii or Lactobacillus-based probiotic for 4 weeks |
| GI Referral | Colonoscopy after 6-8 weeks to exclude Crohn's disease or IBD (given lymph nodes + cecal thickening) |
| Follow-up imaging | Repeat USG or CT in 6 weeks to confirm resolution |
| Surgery | Not needed now - only if perforation, abscess, or non-resolution occurs |
FINDING 2 - Hepatic Fatty Changes (MASLD/NAFLD)
CT Finding: Liver 14cm (normal size), fatty changes, parenchymal heterogeneity, fissure widening, caudate lobe prominence. No focal lesion, no IHBRD.
Disease Explanation:
This is Metabolic dysfunction-Associated Steatotic Liver Disease (MASLD) - formerly called NAFLD. Fat accumulates inside liver cells, causing heterogeneous texture on CT. The caudate lobe prominence and fissure widening suggest this is beyond simple steatosis and heading toward early fibrosis changes. This needs staging urgently.
Treatment (AASLD/EASL 2024 Guidelines):
| Recommendation |
|---|
| Investigations first | LFT, fasting lipids, HbA1c, FIB-4 score, FibroScan (liver elastography) to stage fibrosis |
| Weight loss | 7-10% body weight reduction - single most effective treatment |
| Diet | Mediterranean diet - olive oil, vegetables, fish, whole grains. Eliminate sugar, processed carbs, fructose corn syrup |
| Exercise | 150 minutes moderate aerobic activity per week minimum |
| Alcohol | Complete and permanent cessation |
| Medication | If T2 diabetes/obesity: Semaglutide (GLP-1 agonist) - proven to reduce liver fat. Resmetirom (Rezdiffra) - FDA approved 2024 specifically for MASH with fibrosis |
| Supplements | Vitamin E 800 IU/day (non-diabetic patients), Omega-3 fatty acids |
| Monitoring | LFTs every 3 months, repeat FibroScan at 1 year |
FINDING 3 - Renal Calculus Right Kidney (2.3mm) + Bilateral Simple Cysts
CT Finding: Tiny 2.3mm concretion in right middle calyx. Simple cyst 11.5mm right mid-pole. Simple cyst 11mm left lower pole. No hydronephroureteronephrosis.
Disease Explanation:
The 2.3mm kidney stone is very small - most stones under 5mm pass on their own within 4 weeks with adequate fluids and medication. There is no obstruction (no hydronephrosis), which is reassuring. The simple renal cysts are completely benign fluid-filled sacs (Bosniak Category I) - they need no treatment, only periodic surveillance.
Treatment:
| Recommendation |
|---|
| Fluids | 2.5-3 litres water per day to flush the stone naturally |
| Medical Expulsive Therapy | Tab. Tamsulosin 0.4mg at bedtime x 4 weeks - relaxes ureteric muscle to help stone pass |
| Pain relief | Tab. Ketorolac or Diclofenac as needed for renal colic episodes |
| Diet | Reduce oxalate foods (spinach, nuts, tea, chocolate). Limit salt and red meat. Do NOT restrict calcium |
| Metabolic workup | 24-hour urine for oxalate, calcium, uric acid, citrate, creatinine to identify stone type |
| Renal cysts | Yearly ultrasound surveillance - no treatment needed for Bosniak I |
| Urology referral | If stone does not pass in 4-6 weeks, or if fever/pain/obstruction develops |
FINDING 4 - Degenerative Spondylosis (Spine)
CT Finding: Degenerative spondylotic changes seen in spine (incidental on lung base cuts).
Treatment:
| Recommendation |
|---|
| Physiotherapy | Core muscle strengthening, postural correction, McKenzie exercises |
| Analgesics | Tab. Etoricoxib 60mg once daily after food (short courses as needed) |
| Supplements | Calcium 1000mg + Vitamin D3 2000 IU daily |
| Lifestyle | Avoid prolonged sitting, heavy lifting. Swimming and walking are ideal |
| Orthopaedic review | If back pain radiates to legs, or if tingling/numbness develops |
Normal Findings (No Action Needed)
- Stomach, duodenum, bowel loops - Normal
- Gallbladder, CBD, CHD, Pancreas - Normal
- Spleen (9.5cm) - Normal, no portal hypertension
- Bilateral adrenals - Normal
- Urinary bladder, prostate, seminal vesicles - Normal
- Portal vein, hepatic artery (separate right hepatic artery origin - anatomical variant, benign)
- No pleural or pericardial effusion
Priority Action Checklist for Dr. Sukrit Sud
| Priority | Action | Timeframe |
|---|
| 🔴 Urgent | Start antibiotics for typhlitis | Today |
| 🔴 Urgent | Blood tests: CBC, LFT, CRP, HbA1c, lipids | This week |
| 🟡 Soon | FibroScan for liver fibrosis staging | Within 2 weeks |
| 🟡 Soon | Tamsulosin + high fluid intake for renal stone | Start now |
| 🟡 Soon | GI consultation + colonoscopy planning | Within 4-6 weeks |
| 🟢 Routine | Lifestyle changes for MASLD | Ongoing |
| 🟢 Routine | Annual USG for renal cyst surveillance | 1 year |
| 🟢 Routine | Physiotherapy for spondylosis | Elective |
⚕️ Medical Disclaimer: This report analysis is for educational reference only. All treatment decisions must be made by the treating physician (Dr. Sukrit Sud) after clinical examination, complete history review, and investigation results. The radiologist has specifically recommended clinical correlation.