Tuberculosis covercall point related to medical pathology
Reading File
Finding Sources
Finding Sources
Searching PubMed
tuberculosis pathology granuloma
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Finding Sources
I now have all the material needed to write a thorough, well-structured response. Let me compile it:
Tuberculosis - Medical Pathology: Key Points
1. Causative Agent & Transmission
Mycobacterium tuberculosis - an obligate aerobic, acid-fast bacillus (AFB). It is transmitted by inhalation of aerosolized droplet nuclei from infected individuals. The organism is characterized by a lipid-rich cell wall (mycolic acid) that makes it resistant to Gram staining but identifiable by Ziehl-Neelsen (ZN) or auramine-rhodamine stain (Robbins).
2. Pathogenesis & Immune Response
This is the "covercall" core of TB pathology.
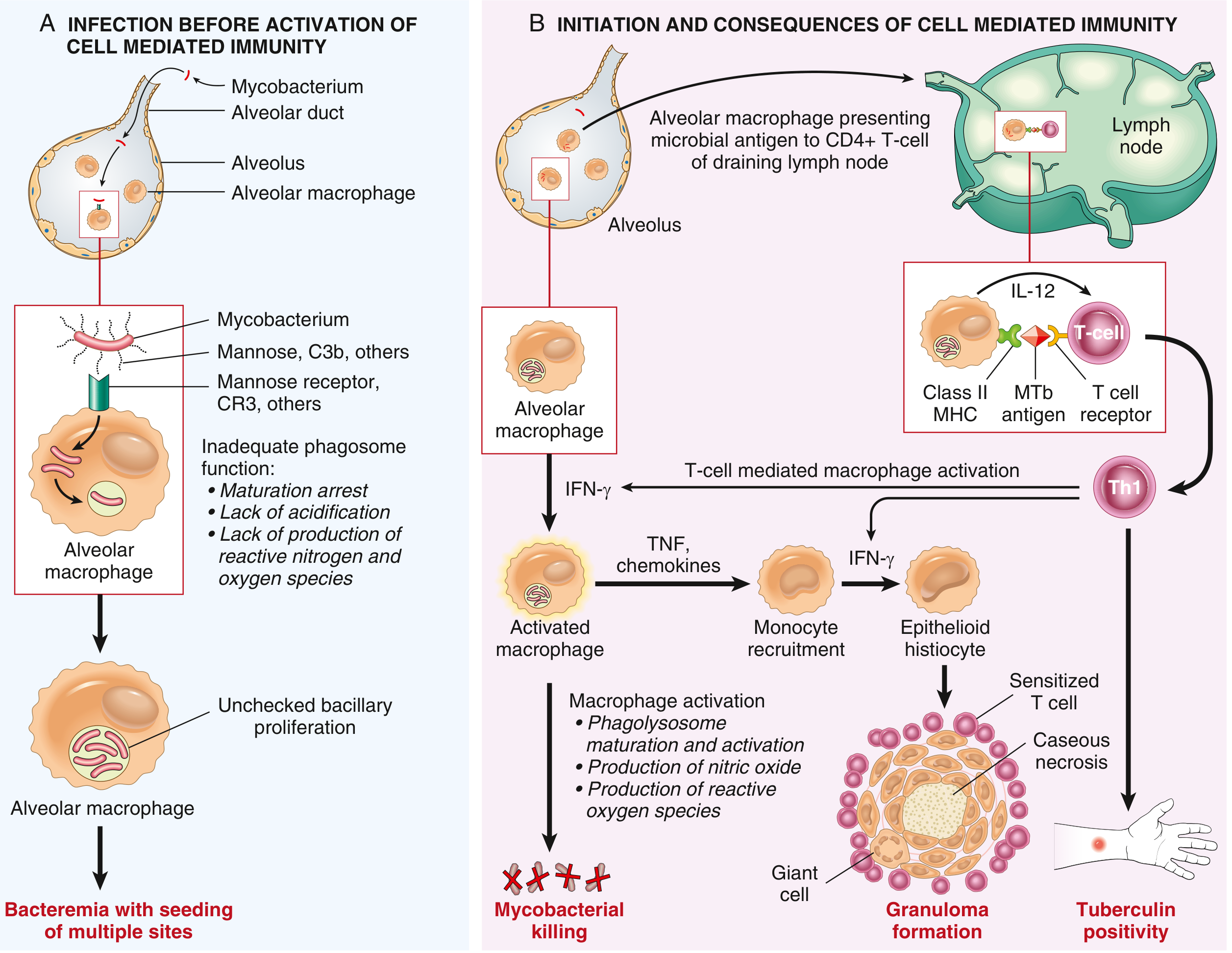
Phase A: Before Cell-Mediated Immunity (first ~3 weeks)
- Inhaled bacilli are engulfed by alveolar macrophages
- M. tuberculosis survives within the phagosome by:
- Arresting phagosome maturation
- Preventing phagolysosome acidification
- Blocking reactive nitrogen and oxygen species
- Result: Unchecked bacillary proliferation and bacteremia with seeding of multiple sites (liver, spleen, bone marrow, kidneys, meninges, apices of both lungs)
Phase B: Initiation of Cell-Mediated Immunity (~3 weeks onward)
- Macrophages present MTb antigens via MHC Class II to CD4+ T cells in draining lymph nodes
- Macrophage-secreted IL-12 drives differentiation to Th1 CD4+ T cells
- Th1 cells release IFN-γ → activates macrophages
- Activated macrophages:
- Produce TNF (recruits monocytes)
- Upregulate iNOS (nitric oxide - kills mycobacteria)
- Produce reactive oxygen species and defensins
- Macrophages differentiate into epithelioid histiocytes → form granulomas; some fuse to form Langhans-type giant cells
Key concept: Immunity comes at the cost of hypersensitivity and tissue destruction (caseation). Defects in IL-12, IFN-γ, TNF, or NO production result in poorly formed granulomas and disease progression. - Robbins & Kumar Basic Pathology, p. 475
3. Primary Tuberculosis
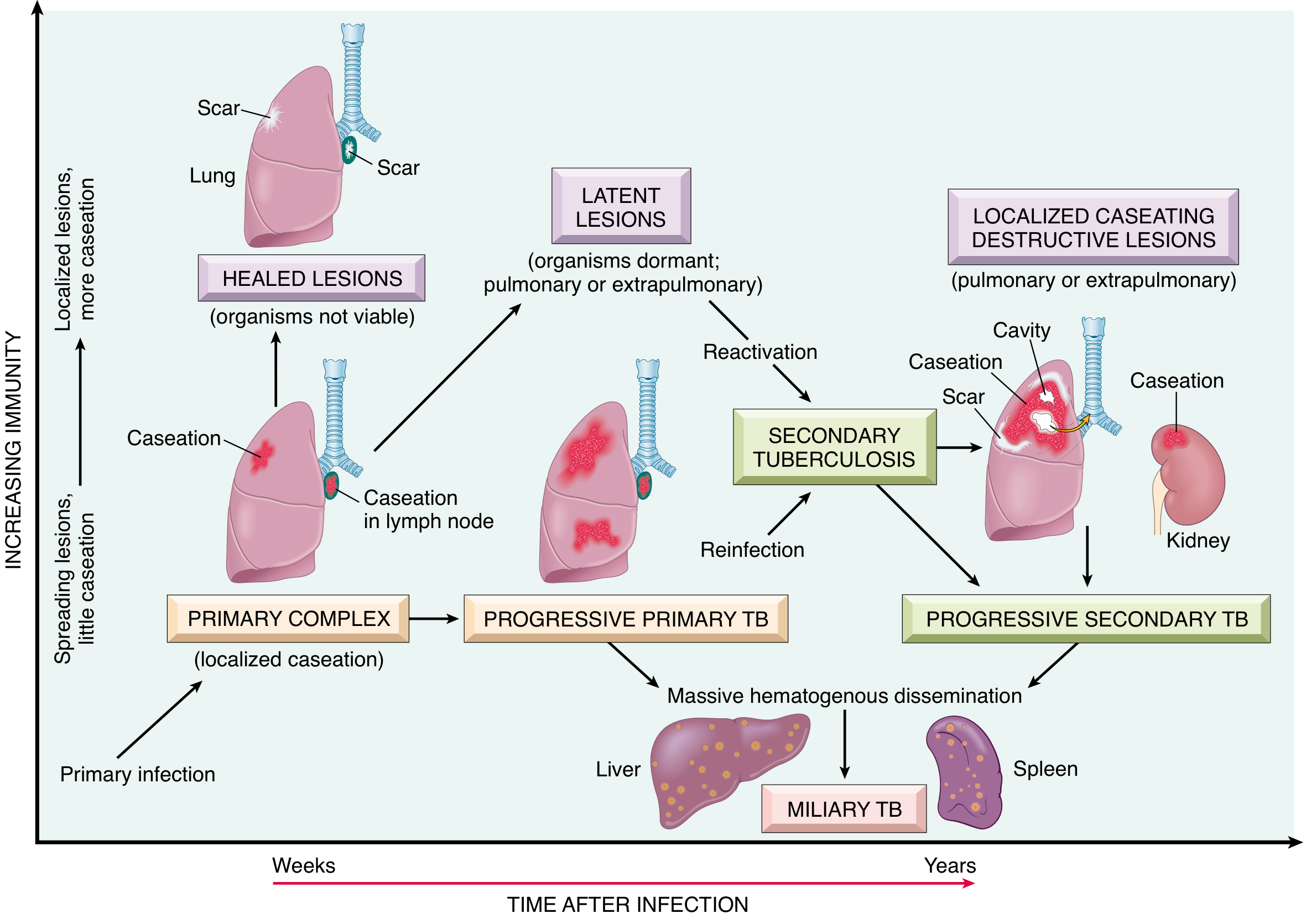
Morphology: The Ghon Complex
| Component | Detail |
|---|---|
| Ghon Focus | 1-1.5 cm gray-white area of caseous consolidation in lower part of upper lobe or upper part of lower lobe, close to pleura |
| Ghon Complex | Parenchymal Ghon focus + caseating hilar/regional lymph nodes |
| Ranke Complex | Calcified Ghon complex (visible on X-ray) after healing |
- In ~95% of cases, cell-mediated immunity controls the infection
- The Ghon complex undergoes progressive fibrosis and calcification
- Despite hematogenous seeding, no lesions develop in organs if immunity is intact
- Only ~5% of newly infected individuals develop significant disease
Progressive Primary TB
- Occurs in immunocompromised patients (HIV, severe malnutrition, very young/old)
- Resembles acute bacterial pneumonia: lobar consolidation, hilar lymphadenopathy, pleural effusion
- May lead to miliary TB or tuberculous meningitis via lympho-hematogenous spread
- Histologically: sheets of macrophages with numerous bacilli but no granulomas (Panel D in image below)
4. Histological Spectrum of Tuberculosis
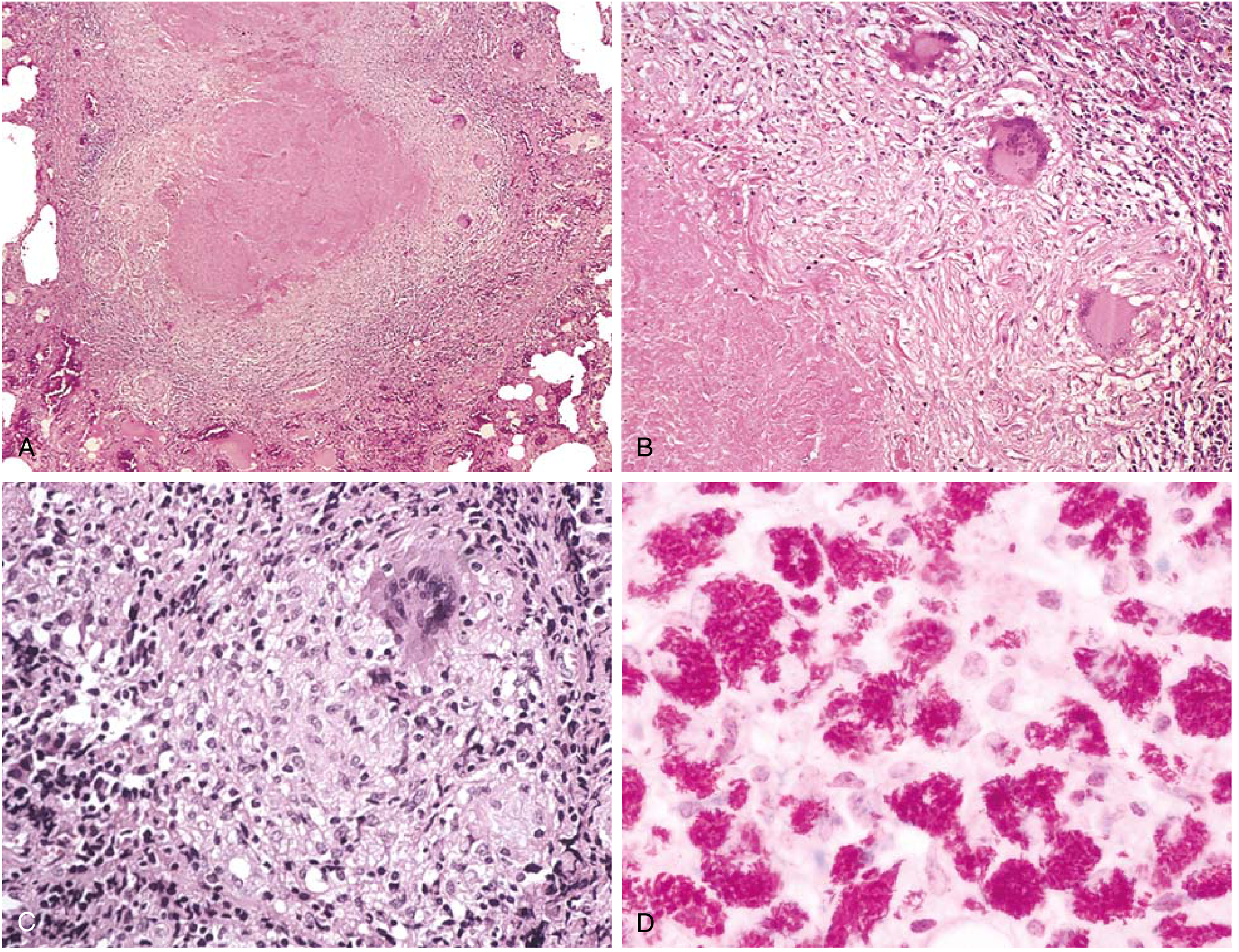
The Tuberculous Granuloma (MUST-KNOW for exams)
- Central caseous necrosis - "cheese-like," pink, acellular material
- Surrounded by: Epithelioid macrophages (activated, elongated)
- Langhans giant cells - nuclei arranged in horseshoe/peripheral arc pattern
- Peripheral rim of lymphocytes and plasma cells
- Outer layer of fibroblasts (fibrosis in healing)
Note: Non-caseating granulomas can occur even in immunocompetent TB patients; therefore ZN/acid-fast staining is always indicated when TB is suspected, regardless of whether caseation is present. - Robbins & Kumar Basic Pathology, p. 477
Caseation vs. Non-caseation
| Feature | Caseating | Non-caseating |
|---|---|---|
| TB | Most typical | Can occur |
| Sarcoidosis | No | Classic |
| Other mimics | Deep fungal infection, leprosy | - |
5. Secondary (Reactivation/Postprimary) Tuberculosis
- Arises in a previously sensitized host - either reactivation of latent disease or re-infection
- Classically involves the apex of upper lobes (high oxygen tension favors aerobic mycobacteria)
- Prompt and marked tissue response due to pre-existing hypersensitivity
- Regional lymph nodes less involved than in primary TB (unlike primary where lymph nodes are prominent)
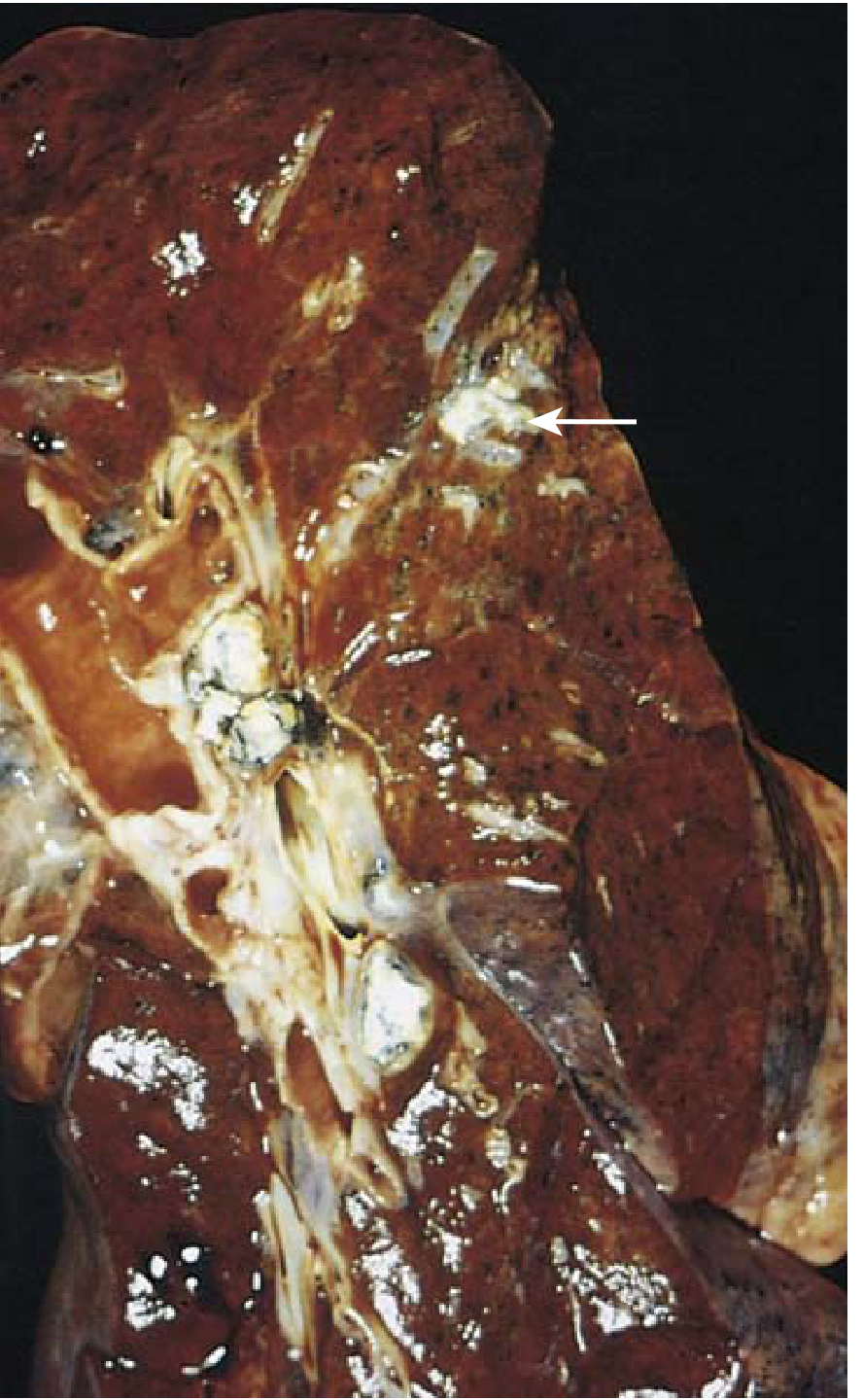
Morphology of Secondary TB
- Initial focus: <2 cm consolidation within 1-2 cm of apical pleura
- Gray-to-yellow with central caseation and peripheral fibrosis
- Cavitation is a hallmark - cavity erodes into airway → expectorated sputum contains bacilli (source of transmission)
- Healing: fibrous encapsulation → fibrocalcific scars
- Active histology: coalescent nodules with central caseation (classic tubercle)
Systemic Symptoms of Secondary TB
- Constitutional: malaise, anorexia, weight loss, low-grade remittent fever (afternoon fever), night sweats
- Pulmonary: productive cough, purulent sputum, hemoptysis (in ~50%)
- Extension to pleura: pleuritic chest pain
6. Miliary Tuberculosis
- Massive hematogenous dissemination of bacilli
- Millet seed-sized (1-2 mm) granulomas scattered throughout lungs, liver, spleen, bone marrow, kidneys, adrenals
- CXR: diffuse bilateral 1-2 mm nodules ("snowstorm" appearance)
- More common in immunocompromised and young children
- Can cause TB meningitis, TB peritonitis, Addison's disease (adrenal involvement)
7. Extrapulmonary TB - Key Sites
| Site | Pathological Finding | Clinical Point |
|---|---|---|
| Lymph nodes (most common extrapulmonary) | Caseating lymphadenitis, can form "cold abscess" | Cervical - scrofula |
| Spine (Pott's disease) | Bony destruction of vertebral bodies | Angular kyphosis (gibbus deformity), paraplegia |
| Genitourinary | Renal cortex granulomas → papillary necrosis | Sterile pyuria, hematuria |
| Meningitis | Basal exudate, perivascular cuffing | Cranial nerve palsies, hydrocephalus |
| Intestine (ileocaecal) | Ulcers (transverse, unlike Crohn's longitudinal), epithelioid granulomas | Malabsorption, obstruction |
| Adrenal | Bilateral caseation | Addison's disease |
| Pericardium | Fibrinous/constrictive pericarditis | Constrictive pericarditis |
8. TB in HIV/Immunocompromised
- Risk increases at all stages of HIV; falls with ART
- With CD4+ >300: "Usual" secondary TB (apical cavitation)
- With CD4+ <200: Resembles progressive primary TB (lobar consolidation, hilar nodes, no cavitation)
- With severe immunodeficiency: No granulomas - sheets of macrophages, very high bacillary load
- Higher rate of false-negative sputum smears and tuberculin tests ("anergy")
- Extrapulmonary involvement >50% in severe immune compromise
- TNF antagonists (used in RA, IBD) also markedly increase TB reactivation risk
9. Diagnosis - Pathological & Laboratory Methods
| Test | Notes |
|---|---|
| ZN (Acid-fast) stain | Identifies AFB in sputum/tissue; needs 10,000 bacilli/mL |
| Culture (Lowenstein-Jensen) | Gold standard; solid agar grows in 3-6 weeks; liquid media 2 weeks |
| PCR (GeneXpert MTB/RIF) | Rapid; detects MTb AND rifampicin resistance |
| Tuberculin skin test (Mantoux/PPD) | Induration at 48-72 hours; does not differentiate active vs. latent; BCG causes false positives |
| IGRA (IFN-γ release assay) | In vitro; fewer false positives; less affected by BCG |
| Histopathology | Caseating granuloma; AFB stain on tissue |
10. Summary Covercall Points
| Point | Detail |
|---|---|
| Causative organism | M. tuberculosis - acid-fast bacillus |
| Entry | Inhalation of droplet nuclei |
| Key immune cell | CD4+ Th1 T cells; activated macrophages |
| Key cytokines | IL-12 (Th1 differentiation), IFN-γ (macrophage activation), TNF (monocyte recruitment) |
| Primary lesion | Ghon focus → Ghon complex → Ranke complex |
| Granuloma type | Caseating (Langhans giant cells + epithelioid histiocytes + central caseation) |
| Secondary TB location | Apex of upper lobes bilaterally |
| Key complication of secondary | Cavitation → airway spread → infectivity |
| Miliary TB | Hematogenous dissemination → millet-seed granulomas everywhere |
| HIV + TB | No granulomas in severe immunodeficiency; high bacillary load |
| Reactivation triggers | HIV, TNF antagonists, malnutrition, diabetes, elderly, steroids |
Sources:
- Robbins & Kumar Basic Pathology (Robbins Pathology), Ch. 11 - Lung Pathology, pp. 475-478
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Ch. 8, pp. 352-355
- [Fitzpatrick's Dermatology Vol. 1&2] - Histopathology of tuberculoid granulomas
- [Bailey & Love's Short Practice of Surgery, 28th Ed.] - Surgical pathology of ileocaecal TB
Most commonsite for pulmonary tb is
Finding Sources
Finding Sources
Finding Sources
The textbook source confirms it clearly. Here is the complete answer:
Most Common Site for Pulmonary TB
Secondary (Reactivation) TB - the classic form
The most common site is the apical and posterior segments of the right upper lobe, and the apical-posterior segment of the left upper lobe.
"The most frequent sites are the apical and posterior segments of the right upper lobe and the apical-posterior segment of the left upper lobe."
- Murray & Nadel's Textbook of Respiratory Medicine
Why the Apex?
The reason is related to high oxygen tension in the lung apices - M. tuberculosis is an obligate aerobe that thrives in high-oxygen environments. The apices also have:
- Poor lymphatic drainage (less immune surveillance)
- Lower blood flow relative to ventilation
- Less macrophage activity compared to lower lobes
Summary by TB Type
| Type | Common Site |
|---|---|
| Primary TB | Lower part of upper lobe / upper part of lower lobe (distal air spaces, close to pleura) - forms Ghon focus |
| Secondary (Reactivation) TB | Apex of upper lobes - apical & posterior segments (RIGHT > LEFT) |
| Miliary TB | Diffuse bilateral involvement (hematogenous spread) |
| Progressive primary TB (HIV/immunocompromised) | Lower and middle lobes (resembles bacterial pneumonia) |
Key Exam Point
- Secondary TB = Apex of upper lobe = high O₂ tension
- Cavitation is characteristic at this site - the cavity erodes into airways → infected sputum expectorated → source of transmission
- On CXR: upper lobe fibronodular shadows/cavities are the classic radiological hallmark
Source: Murray & Nadel's Textbook of Respiratory Medicine; Robbins, Cotran & Kumar Pathologic Basis of Disease
Whzt is the difference btw low grade and high grade fever
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Searching the Web
low grade vs high grade fever temperature classification medical definition
I have sufficient knowledge to give a complete and accurate answer. Here is the full comparison:
Low-Grade vs High-Grade Fever
Definition of Normal Body Temperature
Normal oral temperature: 36.5 - 37.4°C (97.7 - 99.3°F)
Fever (pyrexia) = core temperature above 37.5°C (99.5°F)
Temperature Classification
| Grade | Temperature (°C) | Temperature (°F) | Clinical Term |
|---|---|---|---|
| Normal | 36.5 - 37.4°C | 97.7 - 99.3°F | Afebrile |
| Low-grade fever | 37.5 - 38.4°C | 99.5 - 101.1°F | Subfebrile / Low pyrexia |
| Moderate fever | 38.5 - 39.4°C | 101.3 - 102.9°F | Moderate pyrexia |
| High-grade fever | 39.5 - 40.9°C | 103.1 - 105.6°F | High pyrexia |
| Hyperpyrexia | ≥41°C | ≥105.8°F | Medical emergency |
Costanzo Physiology: "Fever is an abnormal elevation of body temperature. Pyrogens produce fever by increasing the hypothalamic set-point temperature."
Key Differences at a Glance
| Feature | Low-Grade Fever | High-Grade Fever |
|---|---|---|
| Temperature | 37.5 - 38.4°C | ≥39.5°C |
| Onset | Gradual, insidious | Usually acute, sudden |
| Duration | Often prolonged (weeks-months) | Usually shorter (days) |
| Pattern | Remittent, intermittent | Continuous, swinging |
| Rigor/chills | Absent or mild | Often present (rigors) |
| Constitutional symptoms | Mild (fatigue, night sweats) | Severe (malaise, headache, myalgia) |
| Response to antipyretics | Mild/variable | Usually responds well |
Pathophysiology (Common to Both)
The mechanism is the same for both - only the degree differs:
- Pyrogens (bacteria, viruses, immune complexes, tumors, drugs) stimulate phagocytic cells
- These cells release IL-1, IL-6, TNF-α (endogenous pyrogens)
- These act on the anterior hypothalamus → increased local prostaglandin E2 synthesis
- Hypothalamic set-point rises → shivering (heat generation), vasoconstriction (heat conservation)
- Body temperature rises to match the new set-point
Aspirin/NSAIDs work by inhibiting cyclooxygenase → blocking prostaglandin synthesis → lowering the set-point back to normal. - Costanzo Physiology, 7th Ed.
Clinical Causes by Grade
Low-Grade Fever causes:
- Tuberculosis (classic - afternoon low-grade fever + night sweats)
- Viral infections (EBV, CMV, HIV)
- Autoimmune diseases (SLE, RA, IBD)
- Malignancies (lymphoma - "B symptoms")
- Infective endocarditis (subacute - SBE)
- Brucellosis
- Typhoid (early stages)
- Physiological (ovulation, pregnancy)
High-Grade Fever causes:
- Acute bacterial infections (pneumonia, meningitis, UTI, sepsis)
- Malaria (Plasmodium falciparum - can be very high)
- Dengue fever
- Typhoid (later stages - "stepladder" fever)
- Drug fever
- Septicemia
- Acute appendicitis, peritonitis
Hyperpyrexia (>41°C) causes:
- Gram-negative septicemia/septic shock
- Heat stroke
- Malignant hyperthermia (anesthetic complication)
- Pontine hemorrhage (neurogenic fever)
- Thyroid storm
Fever Patterns - Clinically Important
| Pattern | Description | Associated Disease |
|---|---|---|
| Continuous/Sustained | Persistent, <1°C variation, never normal | Lobar pneumonia, typhoid |
| Remittent | Persistent, >1°C variation, never normal | TB, infective endocarditis |
| Intermittent | Returns to normal daily | Malaria, pyemia, abscess |
| Hectic/Swinging | Wide swings, chills + sweating | Abscess, septicemia |
| Relapsing | Fever-free periods, then recurs | Malaria, Brucella, Borrelia |
| Pel-Ebstein | Weeks of fever, then weeks of normal | Hodgkin's lymphoma |
Exam Pearl: TB Fever Pattern
TB characteristically produces a low-grade, remittent fever appearing late each afternoon, accompanied by night sweats and weight loss. This pattern is driven by cytokines (TNF, IL-1) released by activated macrophages in granulomas. - Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.