Renal Calculi (Nephrolithiasis / Urolithiasis) - Comprehensive Review
1. Causes and Risk Factors
Pathogenesis
Kidney stones form when urine becomes supersaturated with stone-forming solutes - that is, when the concentration product of the stone components exceeds their solubility product. The key process is nucleation (crystallization), which progresses to crystal aggregation and stone growth. In calcium stone formers, the stone typically initiates at Randall's plaque - calcium phosphate deposits that form in the renal interstitium at the thin limb of the loop of Henle, migrate to the papillary tip, and provide a nidus for calcium oxalate deposition.
Natural inhibitors of crystallization (citrate, Tamm-Horsfall protein, osteopontin) normally prevent stone formation even in supersaturated urine. Stone disease results when supersaturation overwhelms these defenses.
Dietary Risk Factors
| Factor | Effect |
|---|
| Low fluid intake / dehydration | Concentrated urine - most common correctable cause |
| High animal protein | Increases urinary calcium, uric acid; reduces citrate |
| High sodium intake | Increases urinary calcium excretion |
| High oxalate foods (spinach, rhubarb, nuts, chocolate, tea) | Increases urinary oxalate |
| High fructose / sucrose intake | Increases urinary uric acid and calcium |
| Low dietary calcium | Paradoxically increases stone risk by allowing more oxalate absorption from gut |
| Vitamin C in high doses | Metabolized to oxalate |
(Goldman-Cecil Medicine, p. 148-155; Harrison's Principles of Internal Medicine 22E, p. 2496-2502)
Non-dietary / Systemic Risk Factors
Metabolic disorders:
- Hypercalciuria (most common metabolic cause): absorptive (excess intestinal calcium absorption), renal (impaired tubular reabsorption), or resorptive (hyperparathyroidism, bone disease, sarcoidosis, vitamin D excess)
- Hyperparathyroidism - raises serum calcium leading to hypercalciuria
- Hyperoxaluria: primary (hepatic enzyme defect - autosomal recessive) or enteric (Crohn disease, celiac disease, jejunoileal bypass - malabsorbed fat binds calcium, freeing oxalate for colonic absorption)
- Hypocitraturia: citrate is the most important inhibitor of calcium stones; reduced by acidosis, chronic diarrhea, renal tubular acidosis, hypokalemia
- Hyperuricosuria: gout, myeloproliferative disorders, high-purine diet
- Renal tubular acidosis (type 1): results in alkaline urine, hypercalciuria, and hypocitraturia
- Cystinuria: autosomal recessive disorder with defective renal tubular reabsorption of dibasic amino acids (SLC3A1 / SLC7A9 mutations)
- Primary hyperoxaluria: autosomal recessive defects in hepatic glyoxylate pathway enzymes (AGXT, GRHPR, HOGA1 genes)
- Obesity and metabolic syndrome: insulin resistance impairs renal ammonium excretion, causing persistently low urine pH that promotes uric acid stones
- Gout: associated with uric acid stones
- Type 2 diabetes mellitus
Anatomical factors:
- Medullary sponge kidney
- Urinary stasis (obstruction, horseshoe kidney, uretero-pelvic junction obstruction)
- Neurogenic bladder, indwelling urinary catheters
Infections:
- Urease-producing bacteria (Proteus, Klebsiella, Staphylococcus) - cause struvite stones
Medications:
- Triamterene, indinavir, topiramate, acetazolamide, excess vitamin D/C
Demographic and environmental risk factors:
- Male sex (15% lifetime risk vs. 10% in women)
- Peak incidence 4th-5th decade
- White ethnicity (higher risk in industrialized nations)
- Hot, dry climates (greater insensible fluid loss)
- Family history of stone disease (>2-fold increased risk)
- Sedentary occupations with restricted fluid intake
- Previous stone episode (recurrence rate >50% at 10 years)
(Harrison's 22E, p. 2492-2537; Goldman-Cecil Medicine, p. 38-65; Robbins & Cotran Pathologic Basis of Disease, p. 877)
2. Types of Renal Stones
Classification by Composition
| Stone Type | Prevalence | Appearance | Radiodensity |
|---|
| Calcium oxalate / phosphate | 70-80% | Hard, spiculated (oxalate); smooth (phosphate) | Radiopaque |
| Struvite (magnesium ammonium phosphate) | 5-25% | Large, staghorn calculi | Radiopaque (faintly) |
| Uric acid | 5-10% | Smooth, yellow-brown | Radiolucent on plain X-ray (visible on CT) |
| Cystine | 1-2% | Smooth, waxy; staghorn | Faintly radiopaque |
| Drug-induced / miscellaneous | ~5% | Variable | Variable |
(Robbins & Cotran, p. 416-423; Goldman-Cecil Medicine, p. 44)
Detailed Characteristics by Type
1. Calcium Oxalate Stones (most common)
- Associated with: idiopathic hypercalciuria (50%), hypercalcemia/hypercalciuria (10%), hyperoxaluria (5%), hyperuricosuria (20%), hypocitraturia, no known abnormality (15-20%)
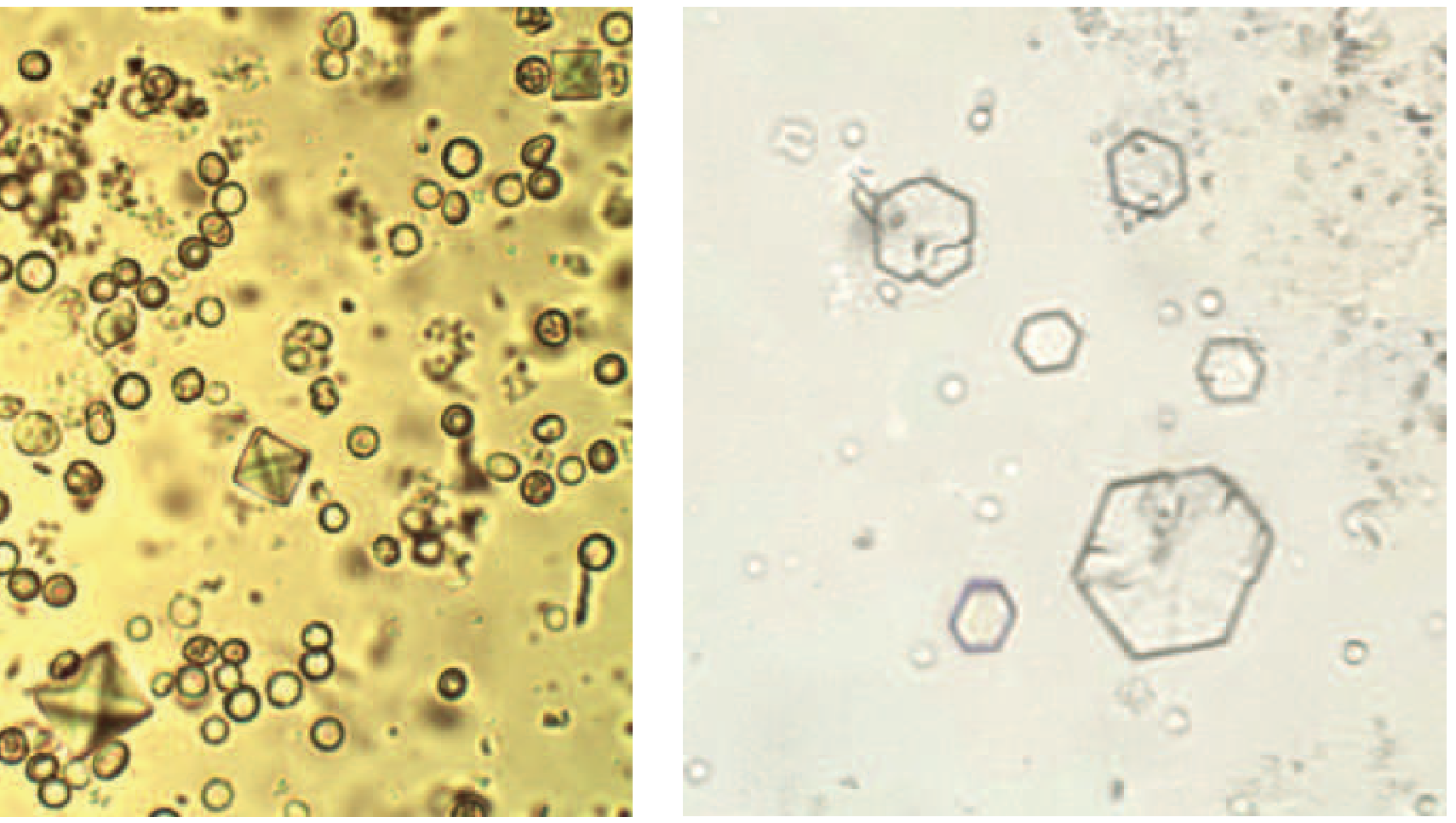
- May be monohydrate (dense, spindle-shaped) or dihydrate (bipyramidal shape on microscopy)
- Calcium oxalate dihydrate crystals appear bipyramidally shaped on urine microscopy
2. Calcium Phosphate (Hydroxyapatite / Brushite)
- Linked to renal tubular acidosis type 1 and primary hyperparathyroidism
- Form in alkaline urine
3. Struvite (Infection) Stones
- Form only with urease-producing bacteria creating an alkaline urine (pH ≥ 7)
- Organisms: Proteus mirabilis, Klebsiella, Staphylococcus epidermidis, Mycoplasma, yeast (E. coli does NOT produce urease)
- Form the largest stones - staghorn calculi that fill the entire renal pelvis and calyces
- Far more common in women (susceptibility to upper UTIs)
- Poor antibiotic penetration; potential for urosepsis unless stones removed
4. Uric Acid Stones
- Increasing in prevalence, parallel to the obesity epidemic
- Require persistently low urine pH (<5.5) - the primary determinant
- Associated with obesity, insulin resistance, type 2 diabetes, gout, myeloproliferative disorders, tumor lysis syndrome, high-purine diets
- 50% are idiopathic
- Classically radiolucent on plain X-ray but visible on CT
5. Cystine Stones
- Autosomal recessive disorder (mutations of SLC3A1 or SLC7A9 genes)
- Defective reabsorption of COLA amino acids: Cystine, Ornithine, Lysine, Arginine
- Poor solubility of cystine leads to stone formation
- Appear as hexagonal crystals on urine microscopy (see image below)
- Often bilateral, multiple, staghorn pattern; recurrent episodes reduce GFR
- Faintly radiopaque (ground-glass appearance)
Urine sediment: calcium oxalate dihydrate crystals (bipyramidal, left) and cystine crystals (hexagonal, right) - Harrison's Principles of Internal Medicine 22E
3. Clinical Manifestations
Symptoms
A. Renal / Ureteral Colic (cardinal symptom)
- Sudden onset of severe, unilateral flank pain - the most common and dramatic presentation
- Despite the name "colic," the pain does not typically completely subside; it varies in intensity
- Rapidly escalating; no alleviating posture or position
- Accompanied by nausea (frequent) and vomiting (occasional)
- Pain radiation depends on stone location:
- Upper ureter: pain radiates anteriorly to the flank/abdomen
- Lower ureter: radiates to the ipsilateral testicle (men) or labium majus (women)
- Ureterovesical junction: urgency, frequency, burning micturition mimicking cystitis
B. Hematuria
- Present in most cases (micro or gross hematuria)
- Gross hematuria without pain can occur
- Absence of hematuria does not exclude a stone (especially with complete obstruction)
C. Other symptoms
- Dysuria, urinary frequency, urgency (especially with distal ureteral stones)
- Nausea and vomiting (often intense)
- Abdominal distension
- Asymptomatic stones discovered incidentally on imaging (7.8-10% of screened populations)
D. Differential diagnosis to consider:
- Stone at right ureteropelvic junction: mimics acute cholecystitis
- Stone at right pelvic brim: mimics acute appendicitis
- Stone at left pelvic brim: mimics sigmoid diverticulitis
(Harrison's Principles of Internal Medicine 22E, p. 2551-2553)
Complications
| Complication | Mechanism |
|---|
| Urinary obstruction | Stone lodges in ureter/ureteropelvic junction |
| Hydronephrosis / hydroureter | Progressive dilation of renal pelvis and ureters due to obstruction |
| Pyelonephritis / urosepsis | Obstruction predisposes to upper UTI; struvite stones harbor bacteria |
| Septicemia | Infected obstructed system - urological emergency |
| Acute kidney injury (AKI) | Bilateral obstruction, or obstruction of a solitary kidney |
| Chronic kidney disease / renal failure | Recurrent obstruction, infection, scarring, tubular atrophy, interstitial fibrosis |
| Renal papillary atrophy | Blunting of pyramids in chronic hydronephrosis |
| Hypertension | Secondary to renal parenchymal damage |
| Renal tubular acidosis | Particularly with bilateral partial obstruction |
(Robbins & Cotran Pathologic Basis of Disease, p. 386-406; CGHS Homoeopathy bulletin)
4. Diagnostic Approach
History
Key elements to elicit:
- Previous stone episodes (number, type, interventions)
- Family history of stone disease
- Diet history: fluid intake, animal protein, high-oxalate foods, calcium intake, supplements
- Medical history: gout, hyperparathyroidism, inflammatory bowel disease, recurrent UTIs, gastric bypass surgery, diabetes
- Current medications (triamterene, topiramate, vitamin C, calcium supplements)
- Review of systems: high insensible losses, GI malabsorption symptoms
Physical Examination
- Costovertebral angle (CVA) tenderness - hallmark finding
- Blood pressure (hypertension from renal damage)
- BMI / body weight
- Signs of primary hyperparathyroidism (rare)
- Signs of gout (tophi)
Imaging Studies
| Modality | Key Features |
|---|
| Non-contrast helical CT (NCCT) - First line | Highly sensitive; detects stones as small as 1 mm; visualizes uric acid stones (radiolucent on plain X-ray); shows perinephric stranding, hydroureteronephrosis, stone location and size |
| Plain X-ray KUB | Detects radiopaque stones; misses ureteral stones and uric acid stones; limited sensitivity |
| Ultrasound KUB | Avoids radiation; excellent for hydronephrosis; sensitive for renal stones but poor for ureteral stones; useful in pregnancy and children |
| Intravenous pyelogram (IVP) | Shows obstruction and anatomy; replaced largely by CT |
| MR urography | For patients with contraindications to CT contrast; identifies hydronephrosis and ureteral lesions |
Key imaging finding: Coronal NCCT showing an obstructing ureteral calculus with hydroureteronephrosis and perinephric fat stranding (shown in Figure 330-2, Harrison's 22E).
Laboratory Investigations
Acute evaluation:
- Serum electrolytes (uncover hypokalemia, renal tubular acidosis)
- Serum creatinine (renal function)
- Serum calcium, phosphorus, uric acid
- PTH level if calcium is elevated, high-normal, or low-normal
- 25-Hydroxy vitamin D
- CBC (elevated WBC with infection)
- Urine culture if infection is suspected
Urinalysis:
- pH: acidic (<5.5) favors uric acid stones; alkaline (>7) favors struvite and calcium phosphate stones
- Hematuria (RBCs)
- Pyuria (infection)
- Crystals: bipyramidal = calcium oxalate dihydrate; hexagonal = cystine; coffin-lid shaped = struvite; needle-shaped = uric acid
- Urine culture
24-hour urine collection (for metabolic workup - especially after first stone):
- Total volume
- pH
- Calcium, oxalate, uric acid, citrate, phosphate, sodium, creatinine
- Calculated supersaturation values
Stone analysis: Chemical composition of passed or retrieved stone via infrared spectroscopy or X-ray diffraction - guides targeted prevention
(Harrison's Principles of Internal Medicine 22E, p. 2561-2613; Goldman-Cecil Medicine)
5. Management
A. Conservative / Medical Management
Acute pain management:
- Parenteral NSAIDs (e.g., ketorolac): randomized trials show equal efficacy to opioids with fewer side effects - first-line
- Opioid analgesics: for breakthrough pain or NSAID contraindications
- Antiemetics for nausea/vomiting
- Hydration: maintain euvolemia (excessive fluid administration not shown to benefit stone passage)
Medical expulsive therapy (MET):
- Alpha-1 adrenergic blockers (tamsulosin): relax smooth muscle of lower ureter, increasing stone passage rates
- Calcium channel blockers (nifedipine): alternative
- Most effective for distal ureteral stones ≤10 mm
- Stones ≤4 mm: 90% pass spontaneously; stones 5-7 mm: ~50% pass; stones ≥8 mm: unlikely to pass
Long-term dietary modification:
- Increase fluid intake: minimum 2-3 L/day (target urine output >2 L/day) - single most important measure
- Moderate animal protein restriction
- Reduce sodium intake
- Maintain adequate dietary calcium intake (do NOT restrict)
- Restrict dietary oxalate (spinach, rhubarb, nuts, chocolate) for calcium oxalate stone formers
Pharmacological prevention by stone type:
| Stone Type | Medical Prevention |
|---|
| Calcium stones with hypercalciuria | Thiazide diuretics (reduce urinary calcium) |
| Calcium stones with hypocitraturia | Potassium citrate (alkalinizes urine, increases citrate) |
| Calcium stones with hyperuricosuria | Allopurinol |
| Uric acid stones | Potassium citrate or sodium bicarbonate (raise urine pH to 6-6.5); allopurinol for hyperuricemia |
| Struvite stones | Treat/eradicate underlying infection; acetohydroxamic acid (urease inhibitor) |
| Cystine stones | Potassium citrate, tiopronin, D-penicillamine (chelate cystine); high fluid intake >3 L/day |
B. Surgical / Interventional Management
Indications for intervention:
- Stone ≥6 mm (low probability of spontaneous passage)
- Persistent obstruction
- Uncontrolled pain or infection
- Progressive renal deterioration
- Active stone growth
| Procedure | Indication | Key Points |
|---|
| Extracorporeal Shockwave Lithotripsy (SWL) | Renal stones ≤20 mm; most proximal ureteral stones | Least invasive; shockwaves fragment stone percutaneously; decreasing use in favor of URS |
| Ureteroscopy (URS) + laser lithotripsy | Ureteral stones; small renal stones | Increasingly preferred; basket extraction or holmium laser; high stone-free rates |
| Percutaneous Nephrostolithotomy (PCNL) | Large (>20 mm), staghorn, complex renal stones | Gold standard for large/complex stones; highest stone-free rate |
| Laparoscopic / robotic stone surgery | Selected patients; complex anatomy | Used in specialized centers; excellent outcomes |
| Open stone surgery | Rare (<1% in developed countries) | Reserved for failed endourologic approaches; still performed in select developing settings |
| Ureteral stent | Bridge therapy; relieve obstruction | Cystoscopically placed; often requires anesthesia; uncomfortable; may increase UTI risk |
"Sandwich technique": combined SWL + PCNL for very large staghorn calculi.
(Campbell Walsh Wein Urology, p. 219-224; Harrison's 22E, p. 2569-2582)
6. Long-Term Outcomes
Stone Passage
- Stones ≤4 mm: ~90% pass spontaneously within 4 weeks
- Stones 5-7 mm: ~50% pass
- Stones ≥8 mm: unlikely to pass spontaneously and typically require intervention
- Natural history of asymptomatic renal stones: many will grow over time, become symptomatic, and ultimately require treatment; a minority remain stable indefinitely
Stone Recurrence
- Recurrence is very common - more than 50% of first-time stone formers will have a recurrence within 10 years
- Without metabolic evaluation and preventive measures, recurrence is the norm
- With targeted dietary and pharmacological prevention, recurrence rates can be significantly reduced
- A careful evaluation to identify predisposing factors is appropriate even after the first stone
Impact on Renal Function
- Single uncomplicated stone passage: minimal long-term impact on GFR
- Recurrent obstruction and instrumentation: can progressively reduce GFR, particularly in cystinuria
- Bilateral partial obstruction: earliest manifestation is inability to concentrate urine (polyuria, nocturia); can progress to distal tubular acidosis, renal salt wasting, chronic tubulointerstitial nephritis, papillary atrophy
- Complete bilateral obstruction: rapidly leads to AKI/anuria
- Struvite (staghorn) calculi: particularly damaging - risk of urosepsis; 40% of pediatric patients with renal scarring develop stage 3+ CKD at 14-year follow-up
- Primary hyperoxaluria: progressive intraparenchymal calcium oxalate deposition leading to ESRD, cardiomyopathy, bone marrow suppression at an early age
- Hypertension is a recognized sequela of chronic obstructive nephropathy
(Campbell Walsh Wein Urology, p. 229-242; Robbins & Cotran, p. 384-406; Harrison's 22E, p. 2587)
7. Homoeopathic Therapeutics for Renal Calculi
Homoeopathy prescribes on the basis of individualization - matching the totality of the patient's symptoms (physical, mental, general) to the remedy picture. There is no single specific remedy for renal calculi; selection depends on the characteristic pain, urinary symptoms, constitutional type, and modalities.
Homoeopathic medicines are reported to be effective in expelling calculi up to 7-8 mm in size and in preventing recurrence when constitutional medicine is used. They are dispensed as mother tinctures, dilutions, biochemics, and triturations.
Principal Homoeopathic Remedies
1. Berberis Vulgaris (Most frequently indicated)
- "Excellent remedy for renal calculi" (Kent)
- Pain radiates from a point and shoots in all directions - upwards to kidneys and downward into bladder, along the ureter, extending into legs
- Formation of pin-head calculi in the renal pelvis descending to bladder with great suffering
- Patient cannot bear the least motion; sits bent over the painful side for relief
- Cannot bear jarring; steps down carefully
- Burning and soreness in the lumbar region
- Urine: dark, turbid, with copious sediment; slow to flow; constant urging
- May also be associated with biliary calculi
- One of the most important remedies for nephritic colic
2. Lycopodium Clavatum
- Usually right-sided complaints
- Pain extends along the ureter and ends in the bladder; does NOT go down the leg (differentiates from Berberis)
- Backache relieved by urination
- Red sand (lithic acid/urate deposits) in clear urine
- Constitutional: desire for sweets and hot drinks; all symptoms worse 4-8 PM; hunger but fullness after little food; flatulence requiring loosening of clothing
3. Sarsaparilla
- Renal colic with severe pain at the conclusion of urination
- Urine passes freely only when standing; can only urinate if standing (characteristic)
- White chalky deposits in urine
- Sand or gravel in urine
- Child screams before and during urination
4. Nux Vomica
- Right-sided renal colic (especially right kidney)
- Pain extends to genitalia and down the leg with nausea and vomiting
- Renal colic with each pain shooting to the rectum, urging to stool
- Must strain to urinate; bladder feels full yet urine dribbles; straining stops the dribbling
- Constitutional type: hypersensitive, mentally and physically; irritable, choleric; lean; chilly
- "Renal colic is caused by a stone in the ureter causing spasm; the proper medicine relaxes these fibres and forces the calculi out at once" - Kent
5. Ocimum Canum (Alfavaca/Sweet Basil)
- Uric acid calculi and high uric acid in urine
- Right-sided renal colic with intense nausea and vomiting
- Urine brick-red or saffron-yellow colored, turbid; smells like musk
- Cramping, twisting pains with great restlessness
- Frequently indicated in children's renal colic
6. Belladonna
- Renal colic with sharp, shooting pains coming suddenly and going suddenly
- Crampy, straining pains along the ureter during passage of calculus
- Patient: feverish, excitable, hypersensitive to jarring
- Pains come and go suddenly (characteristic)
- Associated with redness, heat, dryness
7. Argentum Nitricum
- Nephralgia from congestion of kidneys or passage of calculi
- Dull aching in small of back and over bladder
- Urine dark, contains blood or deposit of renal epithelium and uric acid; passed in drops (nephritic colic)
- Burning while passing urine; urethra feels swollen
- Constitutional: craves sweets (which disagree); anxious, hurried; anticipation anxiety
8. Calcarea Carbonica
- Constitutional remedy for calcium stone formers, especially in fair, flabby, phlegmatic patients
- Tendency to deposits; chilly; desires eggs
- Used for prevention/recurrence in the appropriate constitutional type
9. Nitric Acid
- Urinary calculi when urine contains oxalic acid; for oxalic acid calculi
- Urine of intolerable fetid odour; may smell like horse urine; may feel cold as passed
- Splinter-like pains; worse on touch
- Constitutional: craves salt and fats
10. Benzoic Acid
- Nephritic colic with strongly offensive urine
- Urine deep-red, dark brown, cadaverous smell; alternately thick like pea-soup, then clear
- Patient feels better when urine is profuse and thick; suffers in joints and heart when urine is clear and scanty
- Associated with gout/joint symptoms
11. Hepar Sulphuris Calcareum
- Struvite-type or infected stones with extreme sensitivity to touch and cold
- Hyperirritability; suppurative tendency
- Used when stones are associated with recurrent infection
12. Pareira Brava
- Constant urging to urinate; violent pains radiating down the thighs
- Must go on hands and knees to urinate; urine passes in drops
- Urine contains uric acid crystals, blood, pus; ammoniacal odor
- Particularly indicated in renal/vesical calculi with urethral obstruction
Biochemic Tissue Salts
- Calcarea Phosphorica: calcium phosphate stones; defective calcium metabolism; chronic tendency
- Natrum Sulphuricum: for calculi with excess uric acid; liver affections
- Calcarea Fluorica: hard deposits; tendency to form calculi; associated with tissue induration
General Homoeopathic Advice
- Treatment should be under guidance of a qualified homoeopathic physician
- Constitutional (chronic) prescription prevents recurrence
- USG KUB monitoring every 6 months in patients with recurrence or family history
- Homoeopathic medicines should be taken 30 minutes before or after food
- Conventional life-saving medications for comorbidities (BP, diabetes) should NOT be stopped
- Medicines effective in expelling stones up to 7-8 mm without surgery
(Sources: Dr. Bhatia's Asha Homeopathy; CGHS Ministry of Health Homoeopathy bulletin, Role of Homoeopathy in Management of Renal Stones, June 2023)
Summary Table
| Aspect | Key Points |
|---|
| Most common stone type | Calcium oxalate/phosphate (70-80%) |
| Most common cause | Idiopathic hypercalciuria; dehydration |
| Cardinal symptom | Severe flank pain (renal colic) + hematuria |
| Best imaging | Non-contrast helical CT |
| First-line analgesia | NSAIDs (ketorolac) = opioids for acute colic |
| Spontaneous passage | ≤4 mm: 90%; ≥8 mm: unlikely |
| Recurrence rate | >50% within 10 years |
| Most important prevention | High fluid intake (>2-3 L/day) |
| Gold standard for large stones | PCNL |
| Key homoeopathic remedies | Berberis vulgaris, Lycopodium, Sarsaparilla, Nux vomica, Ocimum canum |
Sources: Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine; Robbins, Cotran & Kumar Pathologic Basis of Disease; Campbell Walsh Wein Urology; CGHS Ministry of Health - Role of Homoeopathy in Management of Renal Stones (June 2023); Dr. Bhatia's Asha Homeopathy Center.