I am a first-year resident in General Medicine. I see many patients with pyuria on the urine complete and also many times there are many RBCs present in the urine complete examination. How to proceed further to localize the disease? By history, examination, and other clinical investigations what definition diagnosis to be kept in mind and how to assess such patients clinically in wards?
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the material I need for a thorough, well-structured answer. Let me compose the comprehensive clinical guide.
Approach to Pyuria and Hematuria on Urine Complete Examination: A Clinical Guide for the Ward Resident
Based on Harrison's Principles of Internal Medicine 22E (2025), Goldman-Cecil Medicine, Comprehensive Clinical Nephrology 7E, NKF Primer on Kidney Diseases 8E, and The Washington Manual.
Part 1 - Definitions and Significance
Pyuria is defined as >10 WBCs per high-power field (HPF) on urine microscopy of a centrifuged sample. The leukocyte esterase dipstick is a surrogate for pyuria (sensitivity 62-98%, specificity 55-96%).
Hematuria is defined as >2-5 RBCs/HPF on microscopy. Dipstick detects hemoglobin - a positive dipstick with no RBCs on microscopy suggests myoglobinuria/rhabdomyolysis (false positive), not true hematuria.
Clinically significant (persistent) hematuria requires at least ONE of:
-
3 RBCs/HPF on three separate urinalyses
- A single urinalysis with >100 RBCs/HPF
- Any gross hematuria
Important: In catheterized patients, pyuria and bacteriuria are almost universal and do not by themselves diagnose UTI. Symptoms are required.
Part 2 - The First Step: Characterize the Urine Sediment
Before you jump to a diagnosis, look at WHAT is present in the urine. This single step already points you in the right direction.
| Sediment Finding | Points Toward |
|---|---|
| WBCs + bacteria + WBC casts | Pyelonephritis / bacterial UTI |
| WBCs only ("sterile pyuria") | TB, atypical organisms, interstitial nephritis, interstitial cystitis |
| RBCs + RBC casts + proteinuria | Glomerulonephritis (glomerular source) |
| Dysmorphic RBCs ("Mickey Mouse" cells, acanthocytes) | Glomerular origin - phase contrast microscopy helpful |
| Non-dysmorphic RBCs, no casts, no proteinuria | Urothelial / lower tract source (stone, tumor, cyst, trauma, prostatitis) |
| WBC casts (in absence of bacteria) | Acute interstitial nephritis, GN |
| Muddy brown granular casts + renal tubular epithelial cells | Acute tubular necrosis |
| Broad/waxy casts | CKD with tubular atrophy |
| Eosinophiluria (Hansel stain) | Allergic interstitial nephritis, atheroembolic disease |
| Uric acid crystals | Tumor lysis syndrome |
| Calcium oxalate crystals | Ethylene glycol poisoning |
The image below from Harrison's 22E illustrates this beautifully:
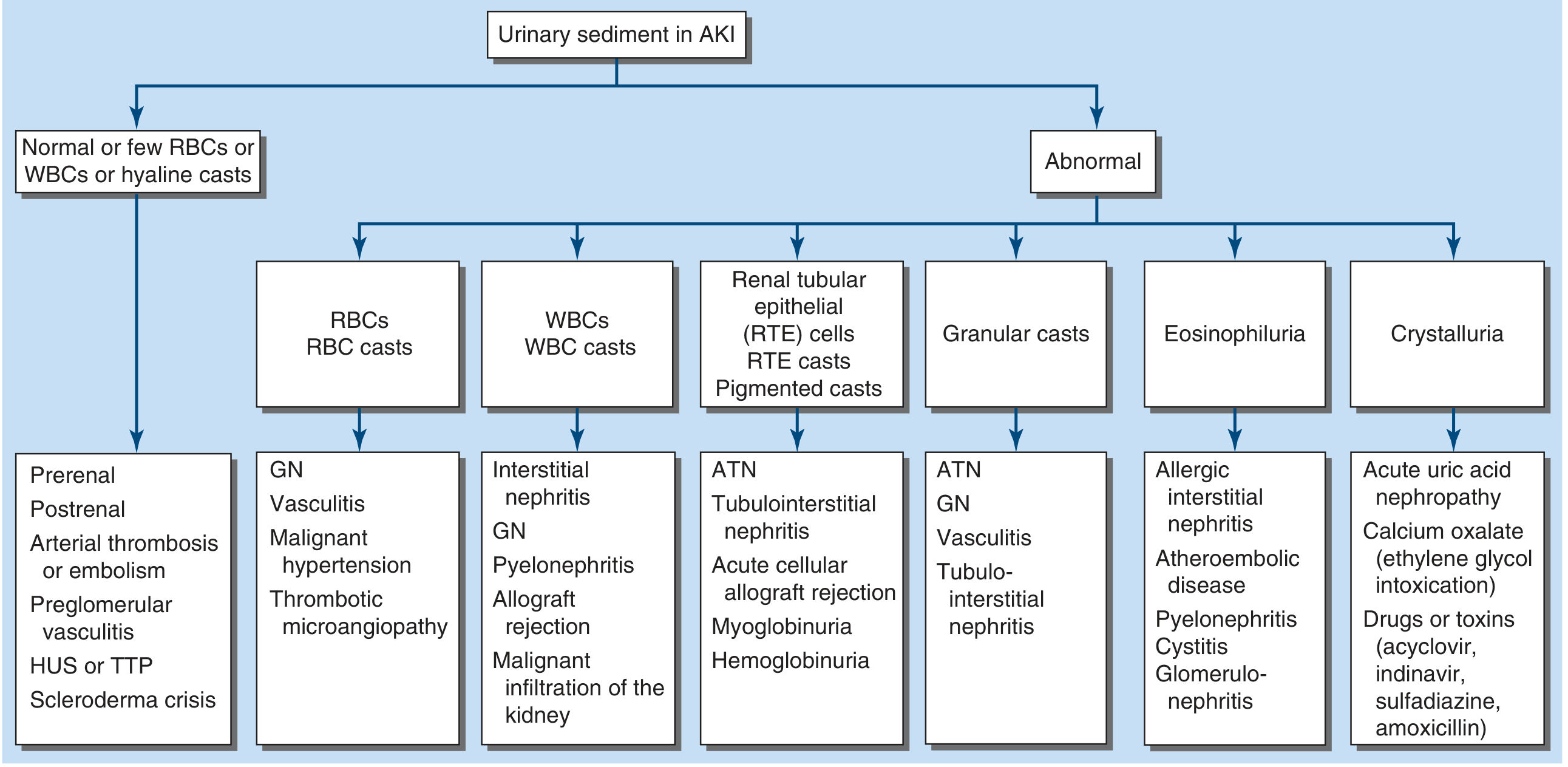
Figure: Interpretation of urinary sediment findings - Harrison's Principles 22E, p. 2424
Part 3 - Localizing the Disease: A Step-by-Step History
The history is your most powerful localizing tool. Ask in a structured sequence.
A. Onset and Time Course
- Acute onset (days): acute GN (post-streptococcal), acute pyelonephritis, drug-induced AIN, urolithiasis, trauma
- Episodic gross hematuria concurrent with URTI: IgA nephropathy ("synpharyngitic hematuria" - same-day onset is key; 10-14 day delay suggests post-streptococcal GN)
- Chronic / smoldering: CKD, chronic interstitial nephritis, thin basement membrane disease, Alport syndrome, urothelial malignancy
B. Symptoms to Ask Directly
| Symptom | Localizing Value |
|---|---|
| Dysuria, frequency, urgency, suprapubic pain | Lower UTI (cystitis/urethritis) |
| Flank/loin pain + fever + rigors + costovertebral angle (CVA) tenderness | Upper UTI (pyelonephritis) |
| Painless gross hematuria | STRONGLY suggests urothelial malignancy (bladder/renal pelvis) - do not assume benign |
| Gross hematuria with clots | Postrenal/collecting system - NOT typically intrinsic renal |
| Frothy/foamy urine | Significant proteinuria (nephrotic range) |
| Puffiness (periorbital in morning, ankle swelling) | Nephrotic or nephritic syndrome |
| Oliguria / anuria + hematuria | Acute GN / RPGN - emergency |
| Recent sore throat (10-14 days ago) or skin infection | Post-infectious GN |
| Joint pains, malar rash, photosensitivity | Lupus nephritis (SLE) |
| Haemoptysis + hematuria | Pulmonary-renal syndrome: Goodpasture's, ANCA vasculitis |
| Dysuria without pyuria in sexually active person | STI (Chlamydia, gonorrhoea) |
| Dry eyes, dry mouth + renal disease | Sjogren's syndrome, TINU syndrome |
| Painful red eye (uveitis) + renal disease | TINU syndrome (Tubulointerstitial Nephritis and Uveitis) |
C. Drug and Toxin History
- PPIs, sulfa drugs, cephalosporins, fluoroquinolones, NSAIDs, checkpoint inhibitors: drug-induced ATIN
- Analgesics (phenacetin, acetaminophen combinations), lithium: chronic interstitial nephritis
- Rifampicin: granulomatous interstitial nephritis
- Aniline dyes (occupational), cyclophosphamide: urothelial malignancy
- Herbal remedies (aristolochic acid): Balkan nephropathy / chronic TIN
D. Past History and Systemic Disease
- Diabetes mellitus: diabetic nephropathy, susceptibility to infections
- Hypertension: hypertensive nephrosclerosis
- Prior sore throat / skin infections: post-infectious GN
- Systemic diseases: SLE, ANCA vasculitis, amyloidosis, myeloma
- Recurrent UTI, urological abnormalities: complicated UTI
E. Family History
- Renal failure in family: Alport syndrome (COL4A5 mutation, X-linked), PCKD
- Microscopic hematuria in family members: thin basement membrane disease
- Multiple bilateral renal cysts: PCKD (also look for cerebral aneurysm history)
Part 4 - Physical Examination: What to Look For
General
- Blood pressure: hypertension is a cardinal feature of both GN and pyelonephritis
- Edema: periorbital (suggests nephrotic), peripheral, anasarca
- Pallor: anaemia of CKD, haemolytic anaemia in TMA (HUS/TTP)
- Weight (fluid overload in acute GN)
Skin and Mucous Membranes
- Malar/"butterfly" rash: SLE
- Palpable purpura (lower limbs): IgA vasculitis (Henoch-Schonlein Purpura), ANCA vasculitis
- Livedo reticularis: atheroembolic disease, antiphospholipid syndrome
- Rash: drug reaction in ATIN
Eyes
- Uveitis/iritis: TINU syndrome
- Fundoscopy: diabetic retinopathy (coexisting with microalbuminuria suggests diabetic nephropathy), hypertensive changes
Ears
- Sensorineural hearing loss: Alport syndrome
Abdomen
- Flank/costovertebral angle tenderness (gentle percussion): acute pyelonephritis, acute GN (tender inflamed kidneys)
- Ballotable kidneys: PCKD, hydronephrosis
- Palpable bladder (percussion): outflow obstruction
- Suprapubic tenderness: cystitis
Respiratory
- Signs of pulmonary haemorrhage (haemoptysis, crackles): Goodpasture's syndrome, ANCA vasculitis (pulmonary-renal syndrome)
Joints
- Arthritis: SLE, ANCA vasculitis, reactive arthritis
Part 5 - Key Clinical Syndromes to Keep in Mind
Once you have finished your history and examination, map your patient to one of these syndromes:
1. Nephritic Syndrome
- Haematuria (dysmorphic RBCs / RBC casts) + proteinuria (1-2 g/24h) + hypertension + oedema + oliguria + rising creatinine
- Causes: post-infectious GN, IgA nephropathy, lupus nephritis, ANCA vasculitis, Goodpasture's
2. Nephrotic Syndrome
- Heavy proteinuria (>3 g/24h) + hypoalbuminaemia + oedema + hypercholesterolaemia + microscopic haematuria
- Causes: minimal change disease, FSGS, membranous nephropathy, diabetic nephropathy
3. Rapidly Progressive GN (RPGN) - EMERGENCY
- Rapid rise in creatinine over days-weeks + active nephritic sediment (RBC casts, dysmorphic RBCs)
- Pathological equivalent: crescentic GN
- Three immunological categories: ANCA-positive (anti-MPO, anti-PR3), anti-GBM (Goodpasture's), immune complex (low C3 - SLE, post-infectious, cryoglobulinaemia)
- If pulmonary haemorrhage present: pulmonary-renal syndrome
4. Acute Tubulointerstitial Nephritis (ATIN)
- Drug exposure + fever + rash + eosinophilia + rising creatinine
- Urine: WBC casts, activated T lymphocytes, eosinophils (Hansel stain), no/minimal proteinuria
- May have polyuria (nephrogenic DI), electrolyte disorders (RTA pattern)
5. Lower UTI (Cystitis)
- Dysuria + frequency + urgency + suprapubic pain
- Urine: pyuria + bacteriuria; no casts; no significant proteinuria
- No systemic signs
6. Upper UTI (Pyelonephritis)
- Fever + rigors + CVA tenderness ± lower UTI symptoms
- Urine: WBC casts + bacteriuria; pyuria
- Requires urine culture + sensitivity
7. Sterile Pyuria - must be explained
- WBCs present, culture negative. Think of:
- Genitourinary tuberculosis (early morning urine x 3 for AFB, TB PCR)
- Atypical organisms: Chlamydia, Ureaplasma, Mycoplasma, gonorrhoea (STI screen)
- Allergic/drug-induced interstitial nephritis
- Interstitial cystitis
- Sarcoidosis / IgG4-related TIN
- Prior antibiotic treatment masking positive culture
8. Isolated Microscopic Hematuria
- Commonest glomerular causes: IgA nephropathy, thin basement membrane disease, hereditary nephritis (Alport)
- If dysmorphic RBCs + RBC casts + protein >500 mg/d: virtually diagnostic of GN - needs biopsy
- If no casts, non-dysmorphic RBCs, no proteinuria: urological workup (stones, tumour, BPH)
- Age >35 years or risk factors for urothelial cancer: cystoscopy mandatory
- CT urography for upper tract evaluation
Part 6 - Investigations to Order in the Ward
Tier 1 - For every patient (Basic workup)
- Urine complete examination (UCE): dipstick + microscopy - always examine fresh urine personally
- Urine culture and sensitivity (midstream clean catch)
- Spot urine protein-to-creatinine ratio (UPCR) or 24-hour urine protein
- Spot urine albumin-to-creatinine ratio (UACR) (especially for diabetics and early disease)
- Serum creatinine + eGFR
- Blood urea nitrogen (BUN)
- Serum electrolytes (Na, K, Cl, HCO3)
- Complete blood count - anaemia (CKD, haemolysis, myeloma), eosinophilia (ATIN, atheroembolic), thrombocytopenia (TMA)
- Blood pressure (essential at every visit)
- Renal ultrasound: kidney size (small = CKD; large = acute GN, PCKD, DM), cortical thickness, echogenicity, hydronephrosis, stones
Tier 2 - Targeted by clinical pattern
If GN suspected (RBC casts, dysmorphic RBCs, significant proteinuria):
- Serum C3, C4 (low in post-infectious GN, SLE, MPGN, cryoglobulinaemia)
- ANA, anti-dsDNA, anti-Sm (SLE)
- ANCA (p-ANCA/anti-MPO; c-ANCA/anti-PR3) - for vasculitis
- Anti-GBM antibody (Goodpasture's)
- Hepatitis B surface antigen, Hepatitis C antibody (membranous, MPGN, cryoglobulinaemia)
- Cryoglobulins
- Serum protein electrophoresis + free light chains (myeloma)
- ASO titre, anti-DNase B, streptozyme (post-streptococcal GN)
- ADAMTS13 level + Shiga toxin if TMA suspected
- Renal biopsy - for definitive diagnosis when GN is suspected and kidneys are normal in size
If interstitial nephritis suspected:
- Urine eosinophils (Hansel stain is more sensitive than Giemsa)
- FENa (if oliguric - <1% in prerenal, >3% in established ATN)
- Giemsa-stained cytocentrifuged urine for activated T cells, eosinophils, plasma cells
- Beta-2 microglobulin (tubular proteinuria)
If infection/pyuria:
- Three early morning urine specimens for AFB (GENITOURINARY TB workup)
- STI screen (endocervical swabs for Chlamydia, gonorrhoea) in sexually active patients
- Fungal culture if immunocompromised
If stone/obstruction suspected:
- Non-contrast CT KUB (best for stones)
- 24-hour urine calcium, oxalate, urate, citrate (if recurrent stones)
- Serum PTH if hypercalcaemia (nephrocalcinosis)
- 24-hour urine oxalate if IBD / gastric bypass patient
If urothelial malignancy suspected (painless haematuria, age >35, occupational exposure):
- CT urography
- Cystoscopy
- Urine cytology
Part 7 - Quick Decision Framework for the Ward
PYURIA found on UCE
|
+-----------+
| |
Bacteriuria No bacteriuria
present (Sterile pyuria)
| |
Lower UTI sx? Think:
(dysuria, freq) TB / STI / ATIN /
| Interstitial cystitis
YES → Cystitis (culture + treat)
NO ↓
Fever + CVA tenderness?
YES → Pyelonephritis (admit if severe, IV antibiotics)
HEMATURIA found on UCE
|
+------------------+
| |
Gross hematuria Microscopic hematuria
| |
Clots present? RBC casts or
dysmorphic RBCs?
YES → Postrenal YES → Glomerulonephritis
(collecting sys) (serologies + biopsy)
NO → IgA neph, |
trauma, lower NO → Urological cause
tract bleed (CT + cystoscopy if >35y)
Part 8 - Pitfalls to Avoid
- Do not diagnose UTI on pyuria alone in catheterised patients or those recently on antibiotics - symptoms are required.
- Do not assume hematuria is benign in patients over 35 - exclude malignancy first.
- Gross hematuria with blood clots is not glomerular - it indicates lower tract/collecting system pathology.
- Sterile pyuria must be investigated - the three most commonly missed diagnoses are genitourinary TB, interstitial nephritis, and STIs.
- A negative dipstick does not rule out bacteriuria in pregnancy - send urine culture regardless.
- Foamy urine + haematuria is not simply "infection" - measure a spot UPCR, as this may be nephrotic syndrome.
- Do not confuse myoglobinuria with hematuria - dipstick positive but no RBCs on microscopy = rhabdomyolysis until proven otherwise.
- In IgA nephropathy, haematuria appears at the SAME TIME as URTI (synpharyngitic), NOT 10-14 days later as in post-streptococcal GN.
Key References:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 319 (Approach to Renal/Urinary Tract Disease), Chapter 326 (Glomerular Diseases), Chapter 140 (UTI)
- Goldman-Cecil Medicine, Chapter 100 (Approach to the Patient with Renal Disease), p. 2494 (Pyuria section)
- NKF Primer on Kidney Diseases 8E, p. 3046 (Nephritic Syndrome, IgA Nephropathy)
- Comprehensive Clinical Nephrology 7E, p. 988 (Urinalysis and Urine Microscopy)
- The Washington Manual, p. 551 (UTI Diagnosis)
This is a shared conversation. Sign in to Orris to start your own chat.