Hernia. Clinical classification. General characteristics of hernia.Rare forms of hernia.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Now I have all the material needed for a comprehensive, well-structured answer. Let me compile it.
Hernia: Clinical Classification, General Characteristics, and Rare Forms
Definition
A hernia is a protrusion of an organ or structure through an opening or pouch. Abdominal wall hernias protrude through the muscular and fascial walls of the abdomen and consist of two parts:
- The orifice (defect in the aponeurotic wall)
- The hernia sac (composed of peritoneum with abdominal contents)
Internal hernias are contained within the abdominal cavity and do not always have a hernia sac.
I. General Characteristics
Structural Components
- Hernia orifice/neck — the fascial defect through which contents protrude
- Hernia sac — peritoneal lining enclosing the herniated contents
- Hernia contents — commonly omentum, small bowel; less often colon, bladder, ovary, etc.
Congenital vs. Acquired
- Congenital — due to a pre-existing anatomical defect (e.g., patent processus vaginalis → indirect inguinal hernia in infants)
- Acquired — from weakening of the abdominal wall due to aging, repetitive strain, surgery, or increased intra-abdominal pressure (obesity, ascites, pregnancy, chronic cough, constipation)
II. Clinical Classification
A. By Reducibility (most clinically important)
| State | Definition | Clinical significance |
|---|---|---|
| Reducible | Contents can spontaneously or manually return to the abdomen | Elective repair advised |
| Irreducible / Incarcerated | Contents cannot be returned | Does not necessarily imply vascular compromise; urgent repair generally indicated |
| Strangulated | Vascular supply is compromised → ischemia or necrosis | Surgical emergency |
A wide-necked hernia may contain non-reducible bowel with no compromise of blood supply and no symptoms other than a bulge. Conversely, smaller hernias carry a greater risk of strangulation — up to 40% of femoral hernias are strangulated at first presentation, vs. only 2% of incisional hernias.— Sleisenger and Fordtran's Gastrointestinal and Liver Disease
B. By Location
1. External (protrude through the abdominal wall)
Groin Hernias
| Type | Anatomy | Epidemiology | Risk of incarceration |
|---|---|---|---|
| Indirect inguinal | Passes through the deep (internal) inguinal ring, traverses the inguinal canal; lateral to inferior epigastric vessels | Most common hernia (65–70% of groin hernias); more frequent in males; congenital origin (patent processus vaginalis) | Moderate; highest in infants (<1 yr) |
| Direct inguinal | Pushes directly through the posterior wall of the inguinal canal (Hesselbach's triangle); medial to inferior epigastric vessels; does not travel along canal | 2nd most common groin hernia; acquired; older men | Low (wide neck) |
| Femoral | Protrudes through the femoral canal, inferior to the inguinal ligament, medial to the femoral vein, lateral to the lacunar ligament | Relatively uncommon; more frequent in women; increases with age | High — up to 45%; 30–40% present as emergencies |
| Pantaloon | Combination of direct + indirect components straddling the inferior epigastric vessels | Uncommon; difficult to reduce manually | Variable |
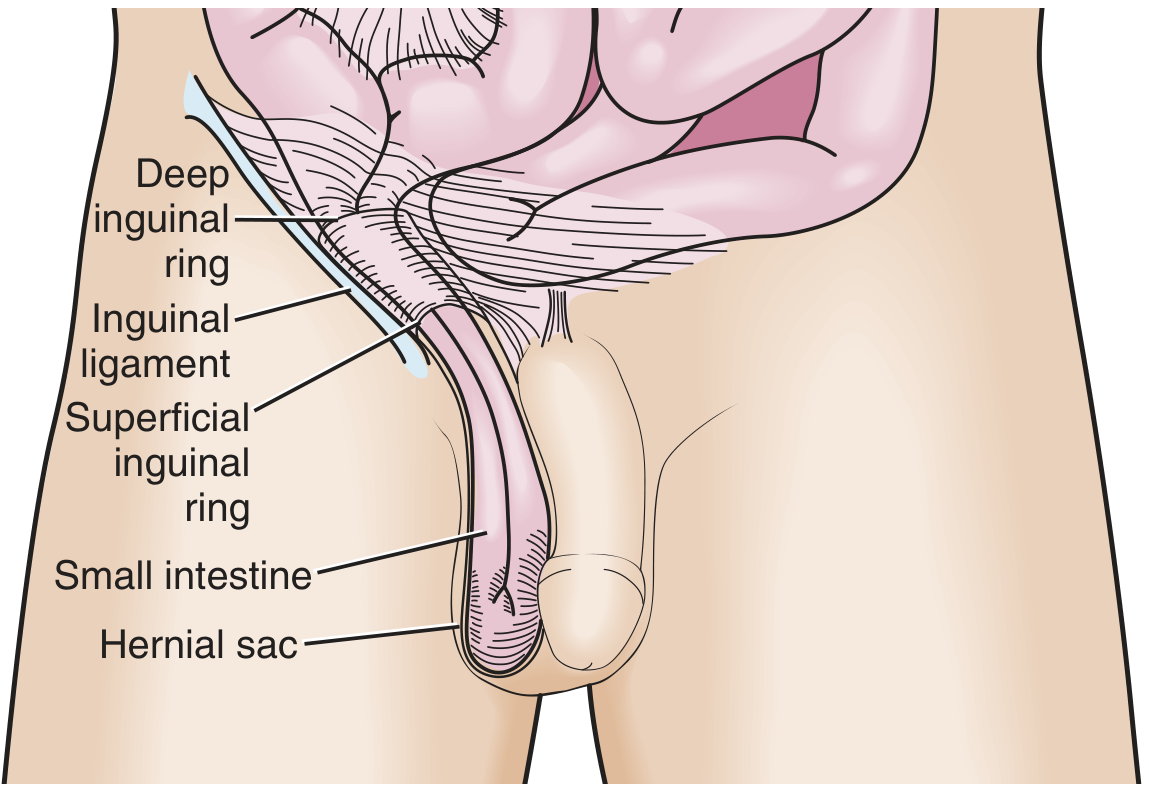
Fig. 1 — Indirect inguinal hernia (Roberts and Hedges' Clinical Procedures in Emergency Medicine)
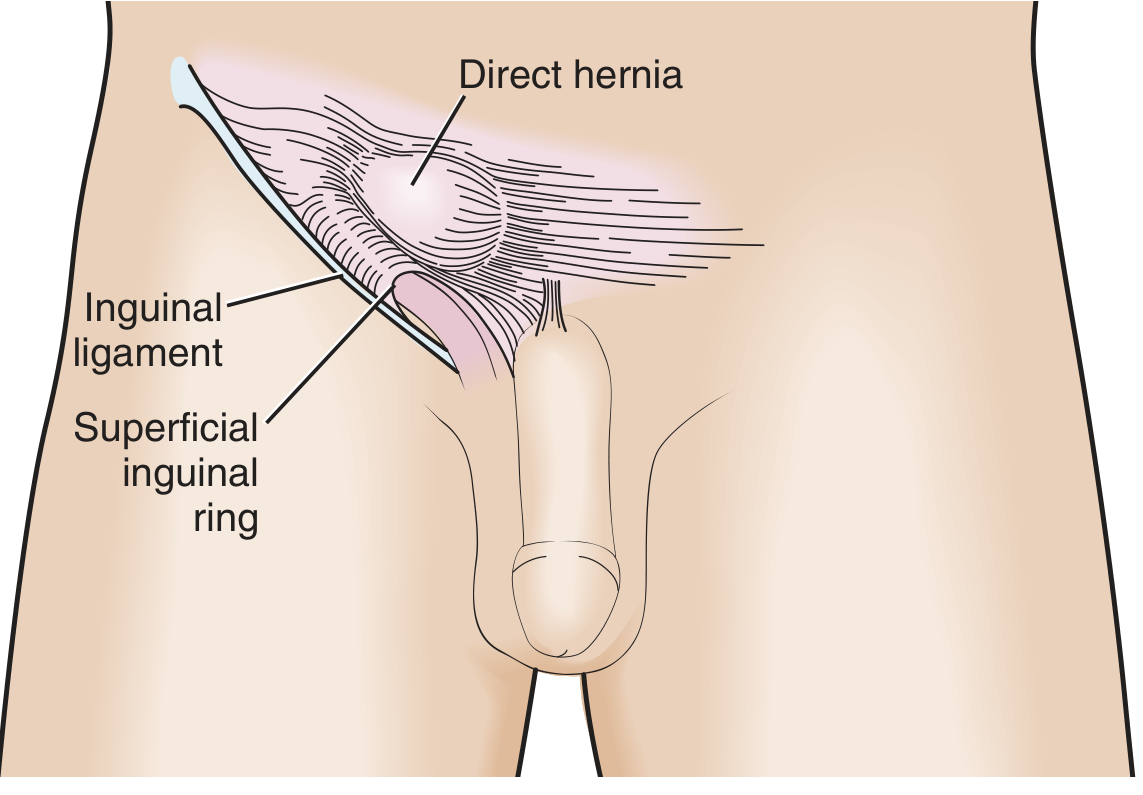
Fig. 2 — Direct inguinal hernia
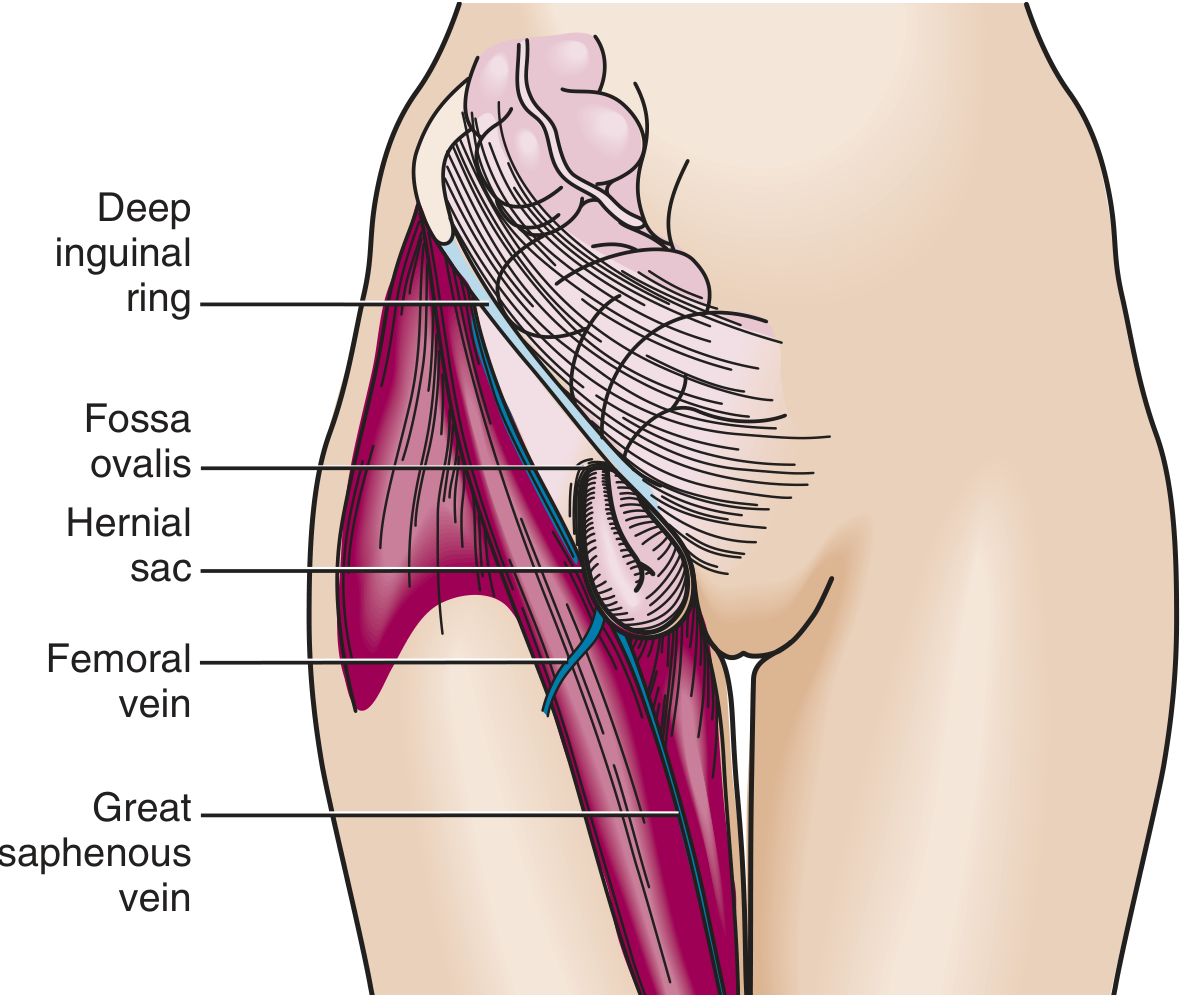
Fig. 3 — Femoral hernia
Ventral / Midline Hernias
| Type | Location | Key features |
|---|---|---|
| Umbilical | Through the fibromuscular umbilical ring | Congenital in infants (often self-resolving by age 5 if <1.5 cm); acquired in adults with ↑ intra-abdominal pressure (obesity, ascites, pregnancy); ~15% of emergency hernia surgery; 60% of emergency repairs show strangulation |
| Epigastric | Through the linea alba, between xiphoid and umbilicus | Usually small, contains preperitoneal fat; may be multiple ("Swiss cheese" defects); complications rare |
| Incisional | Through a previous surgical wound | Occurs in up to 20% of patients after abdominal surgery; recurrence rate 20–50%; larger defects paradoxically carry lower incarceration risk |
Diaphragmatic Hernias
| Type | Description |
|---|---|
| Sliding hiatal (Type I) | Gastroesophageal junction + portion of stomach above diaphragm; orientation unchanged; most common diaphragmatic hernia |
| Paraesophageal (Type II–IV) | GEJ remains below diaphragm but gastric fundus (and potentially entire stomach) herniates; risk of gastric volvulus and strangulation |
| Congenital (Bochdalek / Morgagni) | Congenital diaphragmatic defect; often left-sided (Bochdalek); may contain stomach, bowel, spleen |
| Traumatic | Post-injury diaphragmatic tear |
2. Internal Hernias (contained within the peritoneal cavity)
Congenital forms: paraduodenal (most common congenital internal hernia) and through the foramen of Winslow (posterior to the porta hepatis).
Acquired forms: most commonly iatrogenic following operations that divide the mesentery — Roux-en-Y gastric bypass, colectomy, or pancreaticoduodenectomy. Most common sites after RYGB: mesojejunal mesenteric window, then Petersen's window, then mesocolic window.
The "whirl sign" on CT (mesenteric vessels and bowel appearing to twist around a point) is a key diagnostic finding for internal hernia.
C. By Aetiology
| Category | Examples |
|---|---|
| Congenital | Indirect inguinal, paraduodenal, through foramen of Winslow |
| Acquired | Direct inguinal, incisional, femoral, umbilical (adult), parastomal |
| Traumatic | Diaphragmatic, incisional |
| Iatrogenic | Post-bariatric internal hernia, parastomal |
III. Rare (Uncommon) Forms of Hernia
1. Spigelian Hernia
- Protrudes through a defect in the lateral edge of the rectus abdominis at the level of the semilunar (Spigelian) line and near the arcuate line
- The defect is in the transverse abdominal aponeurosis (spigelian fascia)
- Usually an intramural / interparietal hernia — the sac remains within the abdominal wall layers and may not be visible externally; therefore frequently missed on clinical examination
- Typically in patients aged 40–70 years
- Incarceration rate up to 20% (often contains omentum)
- Diagnosis confirmed with ultrasound or CT
2. Obturator Hernia ("Little Old Lady's Hernia")
- Occurs through the obturator foramen (greater and lesser foramina)
- Almost exclusively in older, cachectic, multiparous women (obturator foramen is larger in women; weight loss depletes the fatty plug)
- Accounts for ~1% of hernia repairs in Asia; 0.07% in the West
- Typically presents as small bowel obstruction
- Pathognomonic signs:
- Howship-Romberg sign — paresthesia/pain in the inner thigh, worsened by hip extension/adduction/internal rotation, relieved by flexion (pressure on obturator nerve); seen in 25–50%
- Hannington-Kiff sign — absent adductor reflex on percussion above the knee
- Richter-type strangulation is common; diagnosis frequently delayed and often made at laparotomy
3. Sciatic Hernia
- Protrudes through the greater or lesser sciatic foramen (formed by the sciatic notch and the sacrospinous/sacrotuberous ligaments)
- May contain ovary, ureter, bladder, or bowel
- Even rarer than obturator hernia: <100 cases reported in the literature
- More common in older women; occasionally seen in children
4. Perineal Hernia
- Occurs through the soft tissues of the perineum; very rare
- Primary: through the urogenital diaphragm (anterior) or between levator ani and coccygeus muscles (posterior); more common in middle-aged women
- Secondary (postoperative): after abdominoperineal resection, pelvic exenteration, or hysterectomy; occurs in <3% of pelvic exenterations and <1% of APRs
5. Lumbar Hernia
- Protrudes through the lumbar triangle (Petit's — inferior lumbar triangle, or Grynfeltt-Lesshaft — superior lumbar triangle)
- Rare; presents as a posterior flank mass
- May be primary (congenital/spontaneous) or secondary (post-traumatic, post-surgical)
6. Richter Hernia (special variant, not rare in femoral region)
- Only one wall of the bowel (most often the antimesenteric side) is caught in the hernia orifice
- Key danger: strangulation can occur without complete intestinal obstruction, making it a diagnostic trap
- Most common in association with femoral hernias; also inguinal
- A complete obstruction can develop if more than half of the bowel circumference becomes incarcerated
7. Paraduodenal (Mesocolic) Hernia
- Most common congenital internal hernia
- Herniation of small bowel into peritoneal folds/fossae adjacent to the duodenojejunal junction
- Left-sided more common than right-sided
- Presents with recurrent episodes of partial bowel obstruction
8. Foramen of Winslow Hernia
- Herniation through the epiploic foramen (posterior to the porta hepatis)
- Very rare; usually contains small bowel, rarely cecum or gallbladder
- High risk of strangulation due to narrow neck
9. Supravesical Hernia
- Protrudes through the supravesical fossa (space anterior to the bladder)
- May be internal or external (appears as inguinal hernia clinically)
- ~30% of cases have associated bladder compression symptoms
10. Broad Ligament Hernia (in females)
- Herniation through a defect in the broad ligament of the uterus
- Can cause chronic pelvic pain; bowel obstruction in ~50%
- May contain small bowel, sigmoid colon, appendix, omentum, or ureter
IV. Hernia-Related Epidemiology (Key Facts)
- Hernias of all types are the second leading cause of small bowel obstruction in Western countries (after adhesions)
- Lifetime risk of groin hernia requiring repair: 27% in men, 3% in women
- ~800,000 groin hernia repairs/year in the USA; 80–90% performed in men
- Indirect inguinal hernias account for 65–70% of groin hernias in both sexes
- Among patients operated for SBO due to hernia, ischemia occurs in up to 75%, necrosis in >25%
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Roberts and Hedges' Clinical Procedures in Emergency Medicine; Mulholland and Greenfield's Surgery: Scientific Principles and Practice, 7e
This is a shared conversation. Sign in to Orris to start your own chat.