Sjogren syndrome
Reading File
Finding Sources
Searching PubMed
"Sjogren syndrome"[MeSH Terms]
Finding Sources
Searching PubMed
"Sjogren syndrome" AND treatment
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Sjögren Syndrome
Sjögren syndrome is a chronic systemic autoimmune disease primarily targeting exocrine glands, characterized by lymphoplasmacytic infiltration, glandular hypofunction, and the hallmark sicca complex of dry eyes and dry mouth. It predominantly affects women (~90% of patients) in their fourth to fifth decades of life, with an estimated prevalence of 1-3%.
Classification
| Type | Definition |
|---|---|
| Primary | Sicca features confined to exocrine glands, without another underlying autoimmune disease |
| Secondary | Sicca features occurring in the setting of another autoimmune disease (RA, SLE, polymyositis, systemic sclerosis, or primary biliary cirrhosis) |
Pathophysiology
The etiology involves a multifactorial interaction between genetics, the immune system, and environmental triggers.
- Genetic predisposition: HLA alleles B8 and DR3 create susceptibility. The major histocompatibility complex is involved.
- Triggering event: Likely a viral infection (e.g., Epstein-Barr virus has been implicated) that initiates an aberrant autoimmune reaction.
- Immune mechanism:
- Dense lymphocytic infiltration of exocrine glands - predominantly CD4+ T lymphocytes and B lymphocytes, with fewer CD8+ T cells, macrophages, and dendritic cells.
- B-cell overstimulation leads to excess immunoglobulins and autoantibodies, altered B-cell distribution peripherally and in salivary glands.
- Formation of germinal centers allows autoreactive B-cell clones to escape tolerance checkpoints.
- Follicular helper T-cell levels are increased.
- IL-12 and IFN-γ are upregulated; Th1 cytokines mediate interactions between APCs and CD4+ T cells in early lesions.
- Aquaporin water channels appear to be an important target - both duct and secretory cells are activated CD4+ T cell targets.
- Salivary gland epithelial cells display an activated phenotype and are presumed to drive the chronic inflammatory response.
Key autoantibodies:
- Anti-Ro (SS-A) - present in 40-80% of primary Sjögren syndrome cases
- Anti-La (SS-B) - another characteristic marker
- Both are ribonuclear proteins detected by ELISA
Clinical Features
Glandular (Sicca) Manifestations
Xerostomia (dry mouth):
- Difficulty chewing, swallowing, and phonation
- Dental caries (multiple)
- Food adherence to buccal mucosa
- Intolerance to acidic and spicy foods
- Smooth, fissured tongue with atrophy of filiform papillae
- Intraoral Candida albicans overgrowth (common)
- Parotid gland enlargement in 25-66% of patients - initially unilateral, eventually bilateral (recurrent/episodic or chronic/fixed)
Keratoconjunctivitis sicca (dry eyes):
- Foreign body sensation - described as "gritty" or "sandy"
- Dilation of bulbar conjunctival vessels, periorneal injection
- Irregularity of corneal image
- Occasionally lacrimal gland enlargement
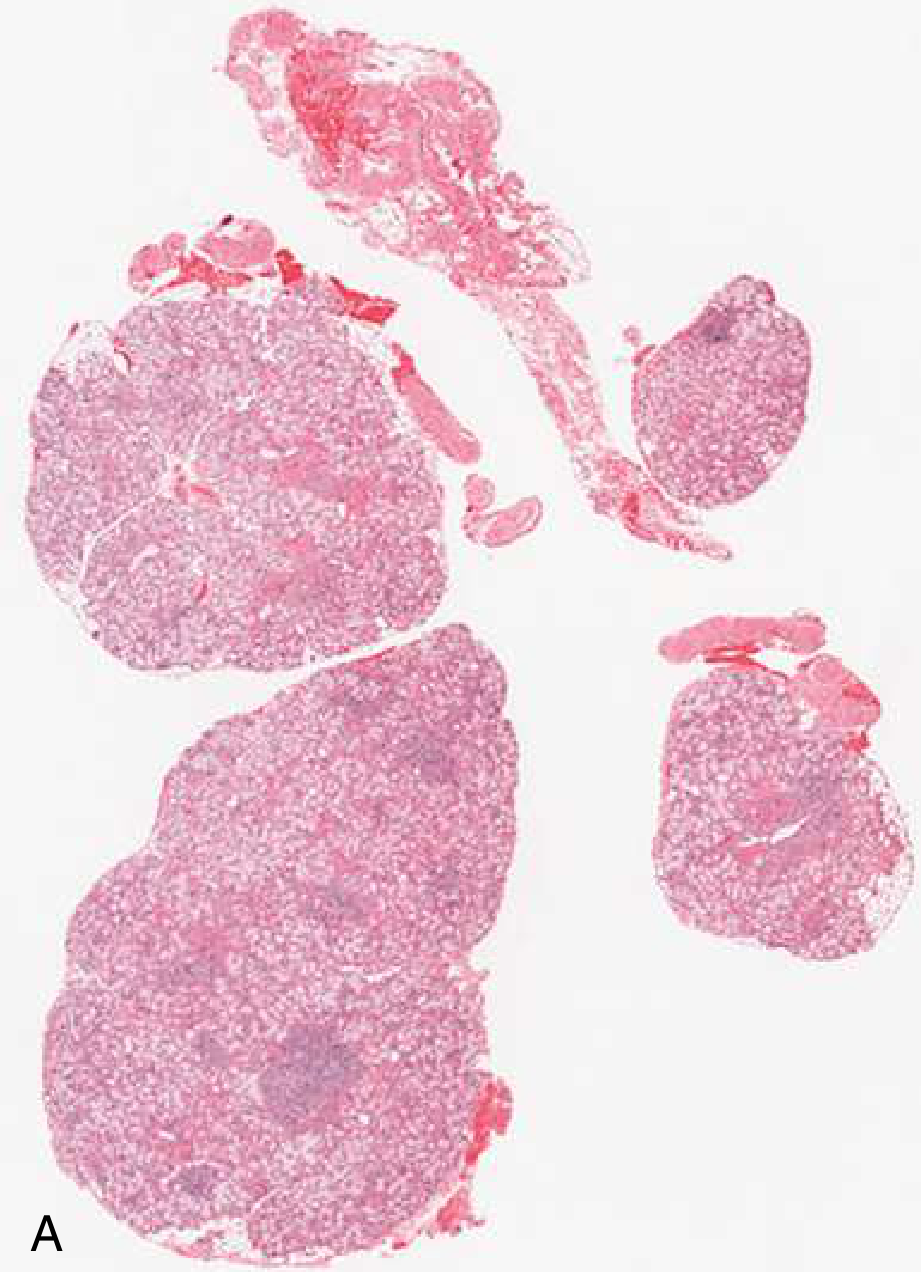
Histopathology of labial salivary glands in primary Sjögren syndrome: H&E staining showing focal lymphocytic sialadenitis - Goldman-Cecil Medicine
Extraglandular Manifestations
| System | Manifestations |
|---|---|
| Constitutional | Generalized malaise, fatigue, low-grade fever, myalgia, arthralgia |
| Skin | Xerosis, Raynaud phenomenon, palpable purpura, recurrent urticaria-like lesions |
| Musculoskeletal | Polyarthralgia/polyarthritis |
| Pulmonary | Dryness of pharynx/esophagus, dysphagia, bronchitis, pneumonia, interstitial lung disease |
| Renal | Renal tubular acidosis, interstitial nephritis |
| Neurological | Peripheral sensory and motor polyneuropathies (can mimic MS), central nervous system involvement, autonomic dysfunction |
| Vascular | Vasculitis in 20-30% |
| Hematologic | Hematologic abnormalities |
Malignant Transformation
- Sjögren syndrome predisposes to non-Hodgkin B-cell lymphoma (marginal zone B-cell lymphoma of salivary/lacrimal glands is most common).
- ~3% develop lymphoma during 9 years of observation; risk persists even after two decades of benign disease.
- High-risk features for lymphoma: palpable purpura, low C4, mixed monoclonal cryoglobulinemia, persistent unilateral or bilateral parotid enlargement.
Diagnosis
Objective Tests
Ocular dryness:
- Schirmer test: <5 mm wetting per 5 minutes (Schirmer I) or stimulated test using nasolacrimal reflex (Schirmer II, <8 mm/5 min)
- Rose bengal / lissamine green staining: identifies corneal/conjunctival epithelial damage; ocular staining score ≥5 (van Bijsterveld ≥4)
Oral dryness:
- Sialometry: Unstimulated whole saliva flow rate ≤0.1 mL/min (Lashley cups over Stensen duct)
- Sialography: demonstrates sialectasis in 85-97% of patients
Histopathology (gold standard):
- Minor salivary gland (labial) biopsy: focal lymphocytic sialadenitis with a focus score ≥1 foci/4 mm². Multiple mononuclear aggregates adjacent to and replacing normal acini. Scored 3 points in the 2016 ACR/EULAR criteria.
- Biopsy should include several glandular lobes from areas with normal overlying mucosa.
Serologic Testing
- Anti-SSA/Ro antibodies (3 points in 2016 criteria)
- Anti-SSB/La antibodies
- Elevated RF (>1:320), ANA (>1:320)
2016 ACR/EULAR Classification Criteria
Applicable to patients with at least one symptom of ocular or oral dryness. A score ≥4 is required for classification.
| Criterion | Score |
|---|---|
| Labial salivary gland biopsy: focal lymphocytic sialadenitis, focus score ≥1/4 mm² | 3 |
| Anti-SSA/Ro positive | 3 |
| Ocular staining score ≥5 (or van Bijsterveld ≥4) in at least one eye | 1 |
| Schirmer test ≤5 mm/5 min in at least one eye | 1 |
| Unstimulated whole saliva flow rate ≤0.1 mL/min | 1 |
Exclusions: Prior head/neck radiation, active hepatitis C (PCR+), AIDS, sarcoidosis, amyloidosis, graft-versus-host disease, IgG4-related disease.
From Shiboski et al., Ann Rheum Dis 2017 - Dermatology 2-Volume Set 5e, Dermatology 2-Volume Set 5e
Differential Diagnosis
- Sarcoidosis (Heerfordt syndrome)
- Lymphoma
- Amyloidosis
- HIV (diffuse infiltrative lymphocytosis syndrome - DILS: massive parotid enlargement, prominent renal/lung/GI manifestations, low autoantibody frequency)
- Hepatitis C infection
- Medications (sedatives, antipsychotics, antidepressants, antihistamines, diuretics)
- Diabetes, cystic fibrosis
Treatment
Treatment is largely symptomatic, though disease-modifying options are emerging.
Sicca Management
Dry mouth:
- Pilocarpine (muscarinic-cholinergic agonist): 5 mg three to four times daily; side effects include sweating, flushing, increased urination
- Cevimeline: another secretagogue
- Sugarless gum/candy (mechanical stimulation of residual gland function)
- Acid maltose lozenges (less expensive, useful for symptom relief)
- Saliva substitutes
- Topical fluoride for dental caries prevention and control
- Antifungals for oral candidiasis
Dry eyes:
- Artificial tears / eye lubricants
- Topical cyclosporine (immunomodulator)
- Pilocarpine also has benefit on subjective eye symptoms
- Eye patching if corneal ulceration develops
Systemic/Disease-Modifying Treatment
| Agent | Indication |
|---|---|
| Hydroxychloroquine | Systemic disease (arthralgia, fatigue); most commonly used |
| Immunosuppressive agents | Depending on severity and type of extraglandular manifestations |
| High-dose corticosteroids | Severe disease |
| Plasma exchange or Rituximab | Cryoglobulinemia; B-cell depletion improves both local and systemic symptoms (xerostomia, fatigue, joint tenderness) |
| TNF inhibitors | Show some promise |
- Rituximab (anti-CD20 monoclonal antibody): depletes B cells peripherally and in salivary glands; evidence for severe/refractory disease
- Systemic corticosteroids or cytotoxic drugs reserved for severe extraglandular complications (glomerulonephritis, necrotizing vasculitis)
Procedural Options
- Sialendoscopy: for recurrent sialadenitis - dilates and washes out affected ducts, reduces intensity/frequency of episodes
- Gland excision: last resort when all other treatments fail
Key Points Summary
- Who: 90% women, 4th-5th decade
- Mechanism: Autoimmune glandular destruction by CD4+ T cells and autoreactive B cells; autoantibodies SS-A/Ro and SS-B/La are characteristic
- Hallmarks: Keratoconjunctivitis sicca + xerostomia (sicca complex)
- Diagnosis: Minor salivary gland biopsy (gold standard) + anti-SSA/Ro + objective sicca tests; 2016 ACR/EULAR score ≥4
- Serious complication: Non-Hodgkin B-cell lymphoma (~44x increased risk vs. general population)
- Treatment: Pilocarpine/cevimeline for sicca, hydroxychloroquine for systemic disease, rituximab for severe B-cell driven disease
Sources: Cummings Otolaryngology Head and Neck Surgery, Goldman-Cecil Medicine International Edition, Textbook of Family Medicine 9e, Andrews' Diseases of the Skin, Dermatology 2-Volume Set 5e (Shiboski 2016 ACR/EULAR criteria)
This is a shared conversation. Sign in to Orris to start your own chat.