Reasons for high blood pressure and fluctuation in cases of very high TSH 72, and low FT3
Reading File
Finding Sources
Finding Sources
Searching PubMed
hypothyroidism hypertension blood pressure TSH
Reading File
Reading File
Finding Sources
Reading Article
PMID: 37967804
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
I now have everything needed for a thorough, well-sourced answer. Here it is:
High Blood Pressure and Its Fluctuations with Very High TSH (72 mIU/L) and Low FT3
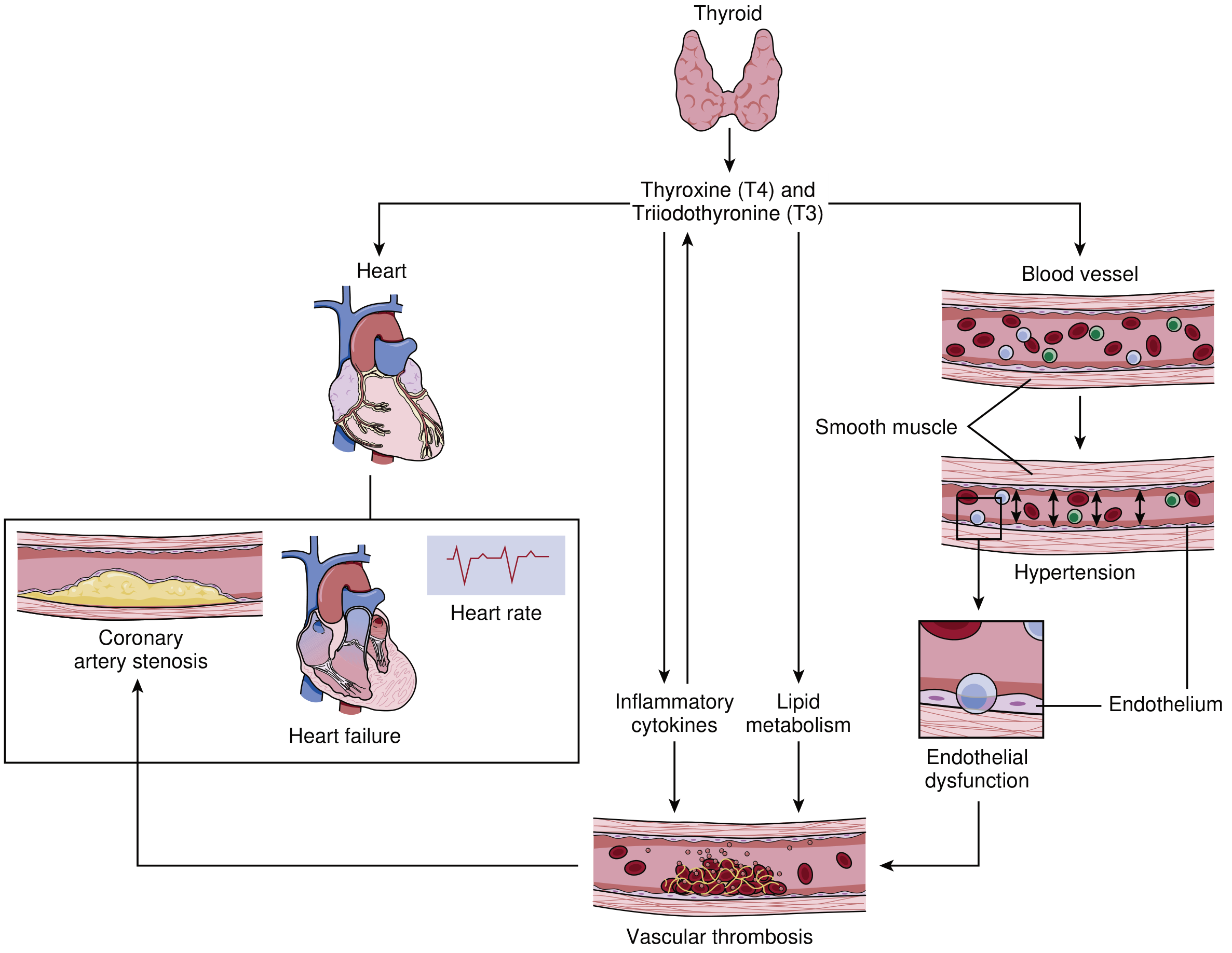
A TSH of 72 with low FT3 represents severe overt hypothyroidism. The pattern of hypertension in this setting is well-characterized, predominantly diastolic hypertension, and it results from several interconnected mechanisms.
Why Blood Pressure Is Elevated
Effects of thyroid hormones on the cardiovascular system - Braunwald's Heart Disease
1. Markedly Increased Systemic Vascular Resistance (SVR)
This is the dominant mechanism. T3 (FT3) normally acts directly on vascular smooth muscle to promote relaxation and vasodilation. When FT3 is critically low:
- Vascular smooth muscle fails to relax properly
- Systemic vascular resistance can increase by up to 30%
- Mean arterial pressure rises, predominantly as diastolic hypertension, in up to 20% of patients
- Braunwald's Heart Disease notes: "Afterload increases in patients with hypothyroidism as a result of increased systemic vascular resistance, arterial stiffness, and endothelial dysfunction."
2. Reduced Nitric Oxide Bioavailability (Endothelial Dysfunction)
FT3/T3 normally stimulates endothelial nitric oxide synthase (eNOS), maintaining nitric oxide (NO) production. With low FT3:
- NO availability is reduced
- The endothelium loses its vasodilatory capacity
- Vascular smooth muscle contracts more readily
- This directly elevates peripheral resistance and diastolic BP
(Braunwald's: "impair relaxation of vascular smooth muscle cells, inducing increases in systemic vascular resistance and arterial stiffness, as well as changes in endothelial function by reducing the availability of nitric oxide")
3. Low Renin - Paradoxical Diastolic Hypertension
This is a distinctive feature: unlike most forms of hypertension, hypothyroid hypertension is associated with low renin levels and decreased hepatic synthesis of renin substrate. The exact mechanism is not fully understood but the volume retention occurs through non-renin-dependent pathways (possibly glycosaminoglycan accumulation and altered renal sodium handling).
4. Arterial Stiffness
Thyroid hormone normally maintains the elasticity of large arteries. Severe FT3 deficiency leads to structural changes in arterial walls, increasing stiffness and reducing compliance. This raises pulse wave velocity and diastolic pressure.
5. Impaired Cardiac Output - Reflex Compensation
With very high TSH and low FT3:
- Cardiac output can fall by 30-40%
- Left ventricular diastolic dysfunction develops
- Heart rate slows (bradycardia)
- The peripheral vasculature compensates by increasing resistance to maintain organ perfusion, which further raises BP
Why Blood Pressure Fluctuates
BP fluctuation (lability) in severe hypothyroidism occurs for these reasons:
A. Mixed Hemodynamic State
In overt hypothyroidism, systolic BP may actually be normal or even low (due to reduced cardiac output and bradycardia), while diastolic BP is elevated. This creates an unusual pattern: isolated diastolic hypertension with a narrow pulse pressure. Goldman-Cecil Medicine specifically lists hypothyroidism as a cause of "isolated diastolic hypertension", in contrast to hyperthyroidism which causes wide pulse pressure. This narrow/variable pulse pressure can make readings appear to fluctuate.
B. Autonomic Dysregulation
T3 modulates sympathetic nervous system sensitivity and adrenergic receptor expression. With severe FT3 deficiency:
- Baroreceptor sensitivity is impaired
- The normal buffering of BP fluctuations is reduced
- Orthostatic changes may be more pronounced
C. Cardiac Contractility Changes
Beat-to-beat variation increases when LV function is impaired (diastolic dysfunction + reduced ejection fraction during exercise). This translates to clinical BP variability.
D. Pericardial Effusion (if present)
In severe/long-standing hypothyroidism, pericardial effusions occur in up to 30% of patients. Even small effusions can alter cardiac filling and output, contributing to variable readings.
E. Antihypertensive Medications Are Ineffective
This is a key clinical point: "Antihypertensive medications are usually ineffective in noneuthyroid individuals" (Rosen's Emergency Medicine). If a patient is being treated for apparent hypertension without recognizing the hypothyroid cause, the underlying vascular resistance is not addressed - which can cause unpredictable responses to medications and apparent fluctuation.
The Role of TSH = 72 Specifically
At TSH levels this high (normal: 0.4-4.5 mIU/L), the degree of thyroid hormone deficiency is severe. Evidence confirms:
- CV risk increases significantly at TSH > 10 mIU/L
- The degree of LDL elevation, vascular resistance increase, and endothelial dysfunction all track proportionally with the TSH level
- A 2024 meta-analysis (Darouei et al., Curr Probl Cardiol) found that levothyroxine therapy reduces both systolic and diastolic BP, and that the effect is greater in patients with higher initial TSH - directly supporting the causal role of severe hypothyroidism in driving hypertension
Summary Table
| Mechanism | Effect on BP | Dominant Pattern |
|---|---|---|
| Increased SVR (FT3 deficiency) | Raises diastolic BP | Isolated diastolic HTN |
| Reduced nitric oxide | Impairs vasodilation | Elevated SVR |
| Low renin state | Sodium retention, diastolic HTN | Diastolic |
| Arterial stiffness | Raises diastolic, narrows pulse pressure | Narrow pulse pressure |
| Reduced cardiac output | May lower systolic | Variable systolic |
| Autonomic dysregulation | BP lability | Fluctuation |
| Bradycardia | Lowers cardiac output | Systolic may be normal/low |
Clinical Implication
The primary treatment is thyroid hormone replacement (levothyroxine) to restore euthyroidism. This progressively:
- Lowers SVR and restores vasodilation
- Improves LV function and cardiac output
- Normalizes BP without the need for antihypertensives in most cases
Standard antihypertensives used alone will typically be inadequate until thyroid status is corrected.
Sources:
- Braunwald's Heart Disease, A Textbook of Cardiovascular Medicine - "Cardiovascular Effects of Overt and Subclinical Hypothyroidism"
- Rosen's Emergency Medicine - "History and Physical Examination" (Hypothyroidism)
- Goldman-Cecil Medicine - "Other Secondary Causes of Hypertension"
- Darouei B et al. (2024). Levothyroxine effect on blood pressure in subclinical hypothyroidism. Current Problems in Cardiology [PMID: 37967804] - Systematic review/meta-analysis confirming BP reduction with treatment, especially in patients with higher baseline TSH.
This is a shared conversation. Sign in to Orris to start your own chat.