What is the role of vasomotor centre role in heart rate and bp
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a thorough answer. Here is the complete explanation:
The Vasomotor Centre (VMC): Role in Heart Rate and Blood Pressure
Location and Basic Anatomy
The vasomotor centre (VMC) is located bilaterally in the reticular substance of the medulla oblongata and the lower one-third of the pons. It is the primary cardiovascular control centre of the central nervous system and integrates signals from throughout the body to regulate both heart rate (HR) and blood pressure (BP).
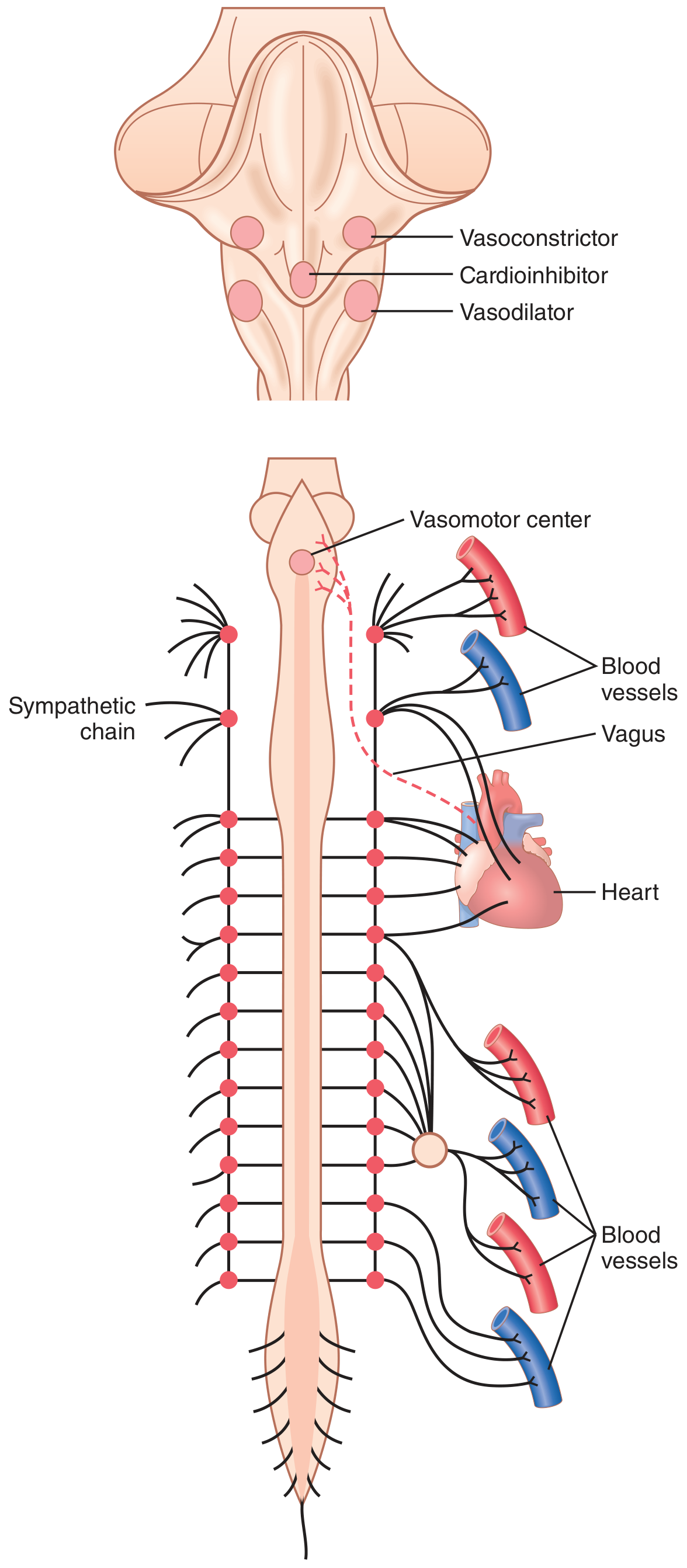
Three Functional Subdivisions
The VMC has three distinct functional areas:
| Subdivision | Location | Action |
|---|---|---|
| Vasoconstrictor area (C1) | Upper medulla / lower pons (lateral) | Transmits sympathetic excitatory impulses - increases HR, contractility, and vascular tone |
| Vasodilator area | Lower medulla (lateral) | Inhibits the vasoconstrictor area, causing vasodilation |
| Sensory/integrating area | Medulla and lower pons | Receives input via CN IX & X; relays to vasoconstrictor and vasodilator areas |
- Guyton and Hall Textbook of Medical Physiology
- Costanzo Physiology 7th Edition
Role in Heart Rate
The VMC controls heart rate through dual autonomic outflow:
1. Sympathetic (Accelerator) Pathway - Increases HR
- The lateral portions of the VMC transmit excitatory impulses through sympathetic nerve fibers.
- These fibers reach the SA node and increase its firing rate, thereby increasing heart rate.
- They also increase AV node conduction velocity and myocardial contractility (positive chronotropic and inotropic effects).
2. Parasympathetic (Decelerator) Pathway - Decreases HR
- The medial portion of the VMC sends signals to the dorsal motor nuclei of the vagus nerve (CN X).
- These parasympathetic impulses travel to the SA node and decrease heart rate.
"The lateral portions of the vasomotor center transmit excitatory impulses through the sympathetic nerve fibers to increase heart rate and contractility. Conversely, the medial portion of the vasomotor center sends signals to the adjacent dorsal motor nuclei of the vagus nerves, which then transmit parasympathetic impulses through the vagus nerves to the heart to decrease heart rate and heart contractility."
- Guyton and Hall Textbook of Medical Physiology
Key principle: Heart rate and strength of contractions ordinarily increase when vasoconstriction occurs and ordinarily decrease when vasoconstriction is inhibited, meaning the VMC coordinates both vascular and cardiac responses together.
Role in Blood Pressure
The VMC regulates BP through multiple mechanisms:
1. Vasomotor Tone (Basal Vascular Tone)
The vasoconstrictor area of the VMC continuously fires at 0.5-2 impulses/second through sympathetic vasoconstrictor fibers throughout the body. This constant low-level firing creates vasomotor tone - maintaining blood vessels in a state of partial constriction. This tone:
- Sets resting BP (~100 mmHg mean arterial pressure)
- Allows BP to be increased or decreased by modulating tone up or down
- If suddenly abolished (e.g., total spinal anesthesia), BP can plummet from ~100 to ~50 mmHg
2. Control of Peripheral Vascular Resistance (TPR)
Sympathetic outflow from the vasoconstrictor area acts on arterioles to alter resistance. Arterioles in skin, kidneys, spleen, and mesentery have heavy sympathetic innervation. Constriction raises total peripheral resistance and therefore raises BP; dilation lowers it.
3. Venous Return and Preload
Sympathetic venoconstriction reduces venous capacitance, mobilizing the ~80% of total blood volume stored in veins. This increases venous return, raises cardiac preload, and increases cardiac output and BP via the Frank-Starling mechanism.
The Baroreceptor Reflex - The Main Feedback Loop
The VMC is the central processing hub of the baroreceptor reflex, the most important short-term BP regulatory system:
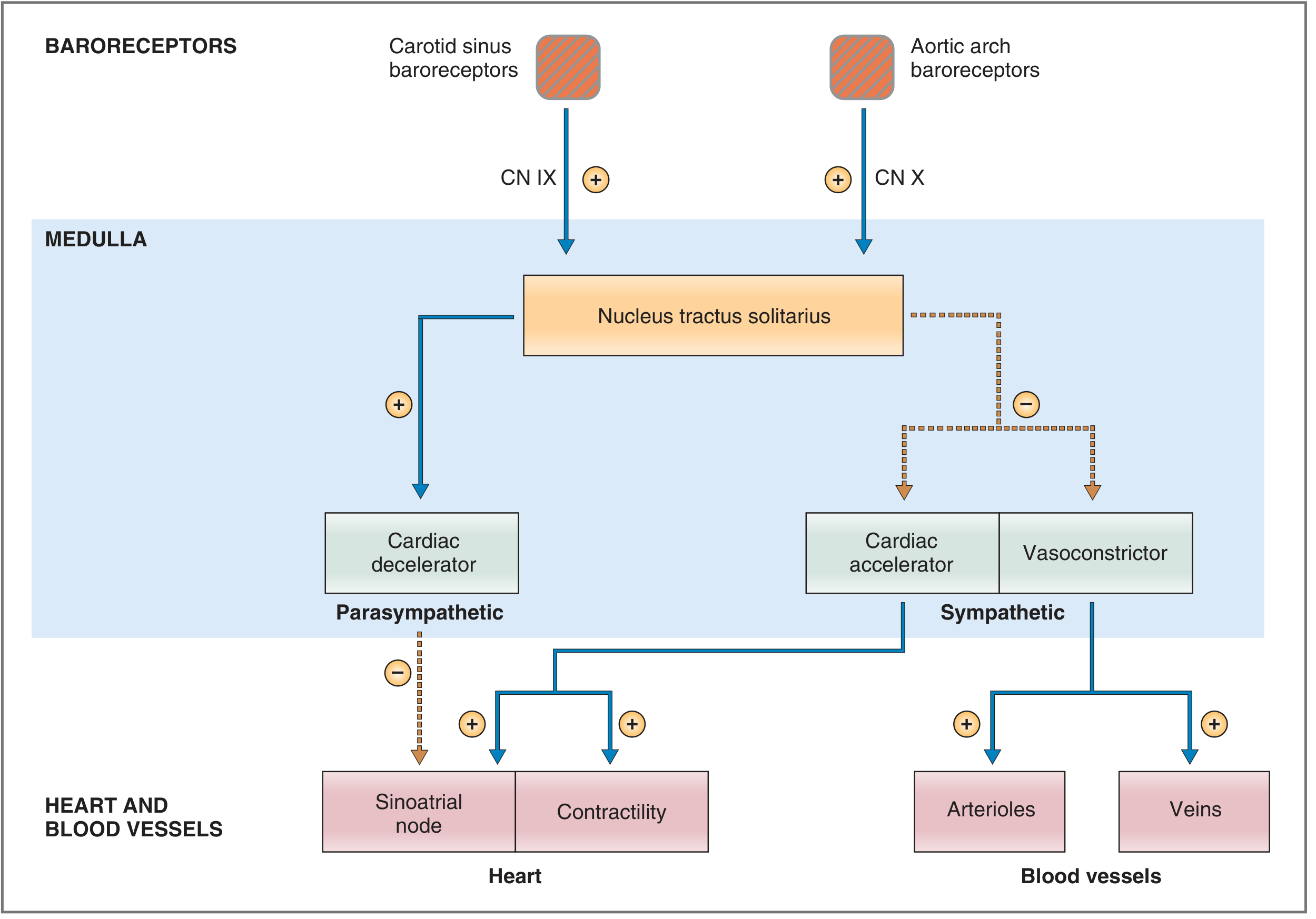
When BP rises:
- Baroreceptors in the carotid sinus (CN IX) and aortic arch (CN X) increase their firing rate
- Afferent signals travel to the nucleus tractus solitarius (NTS) in the medulla
- The NTS inhibits the vasoconstrictor/cardiac accelerator centers and activates the cardiac decelerator center
- Result: decreased sympathetic outflow + increased vagal (parasympathetic) tone → HR decreases, contractility decreases, arterioles dilate → BP falls back to normal
When BP falls (e.g., hemorrhage):
- Baroreceptors reduce firing
- NTS reduces its inhibitory effect on the VMC
- VMC becomes more active - increased sympathetic outflow
- HR and contractility increase, arterioles constrict → BP is restored
Higher Centre Modulation
The VMC does not act in isolation. It receives modulatory inputs from:
- Hypothalamus: Posterolateral areas cause excitation (raise BP/HR); anterior areas may inhibit
- Cerebral cortex: Emotional states (fear, anger) raise BP via cortical-hypothalamic-VMC pathways
- Reticular formation of pons and mesencephalon: Lateral/superior regions excite; medial/inferior regions inhibit
- Chemoreceptors: Hypoxia activates the VMC, raising BP (Cushing reflex at extreme levels)
Summary Table
| VMC Action | Mechanism | Net Effect |
|---|---|---|
| Lateral VMC activation | SNS → SA node, myocardium | HR increases, contractility increases |
| Medial VMC activation | PNS (vagus) → SA node | HR decreases |
| Vasoconstrictor area tone | SNS → arterioles, venules | TPR increases, BP rises |
| Vasodilator area activation | Inhibits vasoconstrictor area | TPR decreases, BP falls |
| Baroreceptor reflex (high BP) | NTS inhibits VMC | HR, contractility, TPR all decrease |
| Baroreceptor reflex (low BP) | NTS activates VMC | HR, contractility, TPR all increase |
The VMC is thus the integrating hub that continuously balances sympathetic and parasympathetic outflow to keep BP and HR within normal limits, responding within seconds to any perturbation.
- Guyton and Hall Textbook of Medical Physiology
- Costanzo Physiology 7th Edition
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e
What is RVLM and CVLM
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have comprehensive textbook content and two high-quality diagrams. Here is the complete answer:
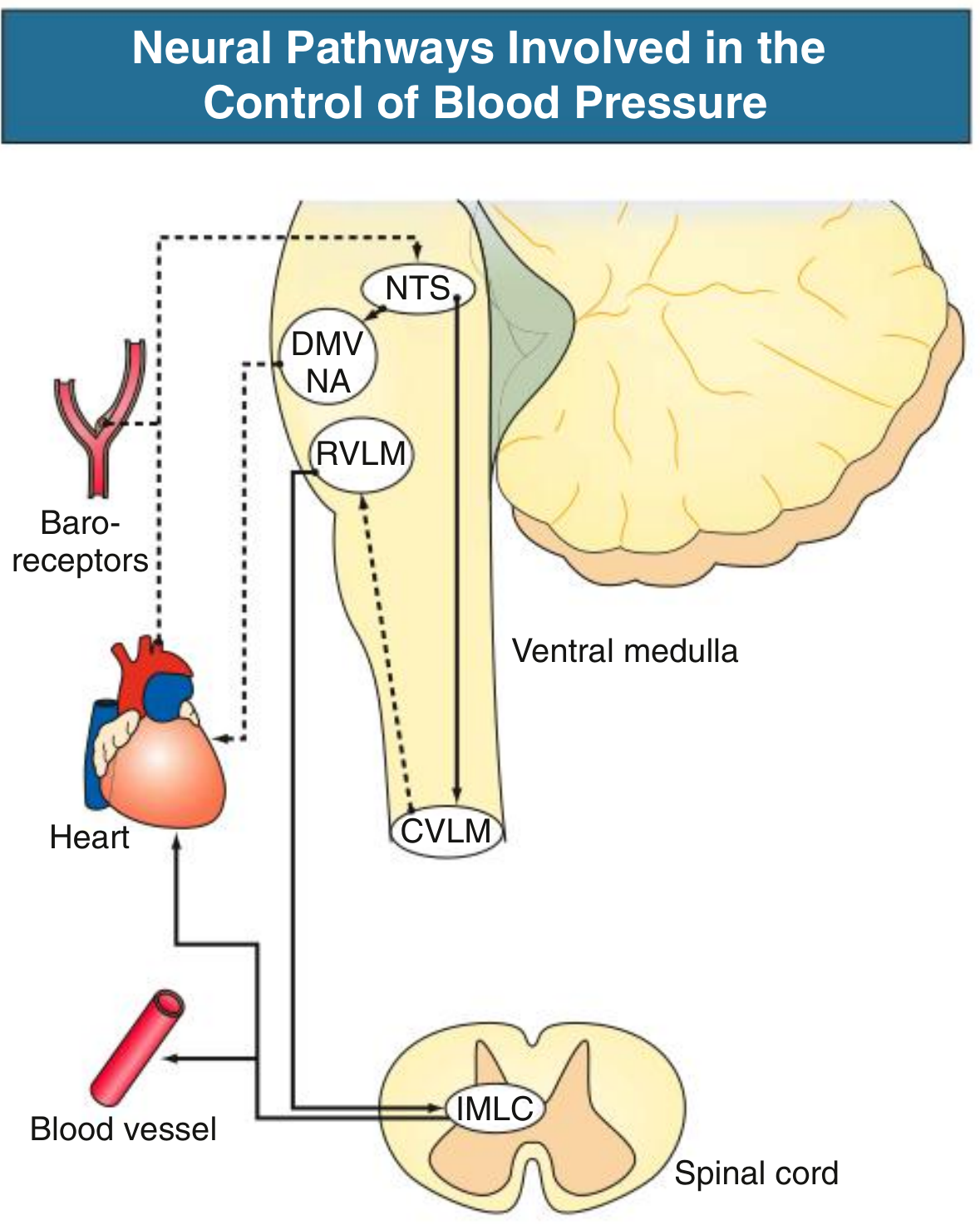
RVLM and CVLM: The Core of Medullary Cardiovascular Control
Overview
The vasomotor centre is not a single homogeneous area - it is organized into functionally distinct subregions. The two most important are:
| Region | Full Name | Functional Role |
|---|---|---|
| RVLM | Rostral Ventrolateral Medulla | Pressor area - drives sympathetic outflow, raises BP and HR |
| CVLM | Caudal Ventrolateral Medulla | Depressor area - inhibits RVLM via GABA, lowers BP |
RVLM - Rostral Ventrolateral Medulla
Location
Neurons are located near the pial surface of the medulla, in the rostral (upper) portion of the ventrolateral medulla.
What It Does
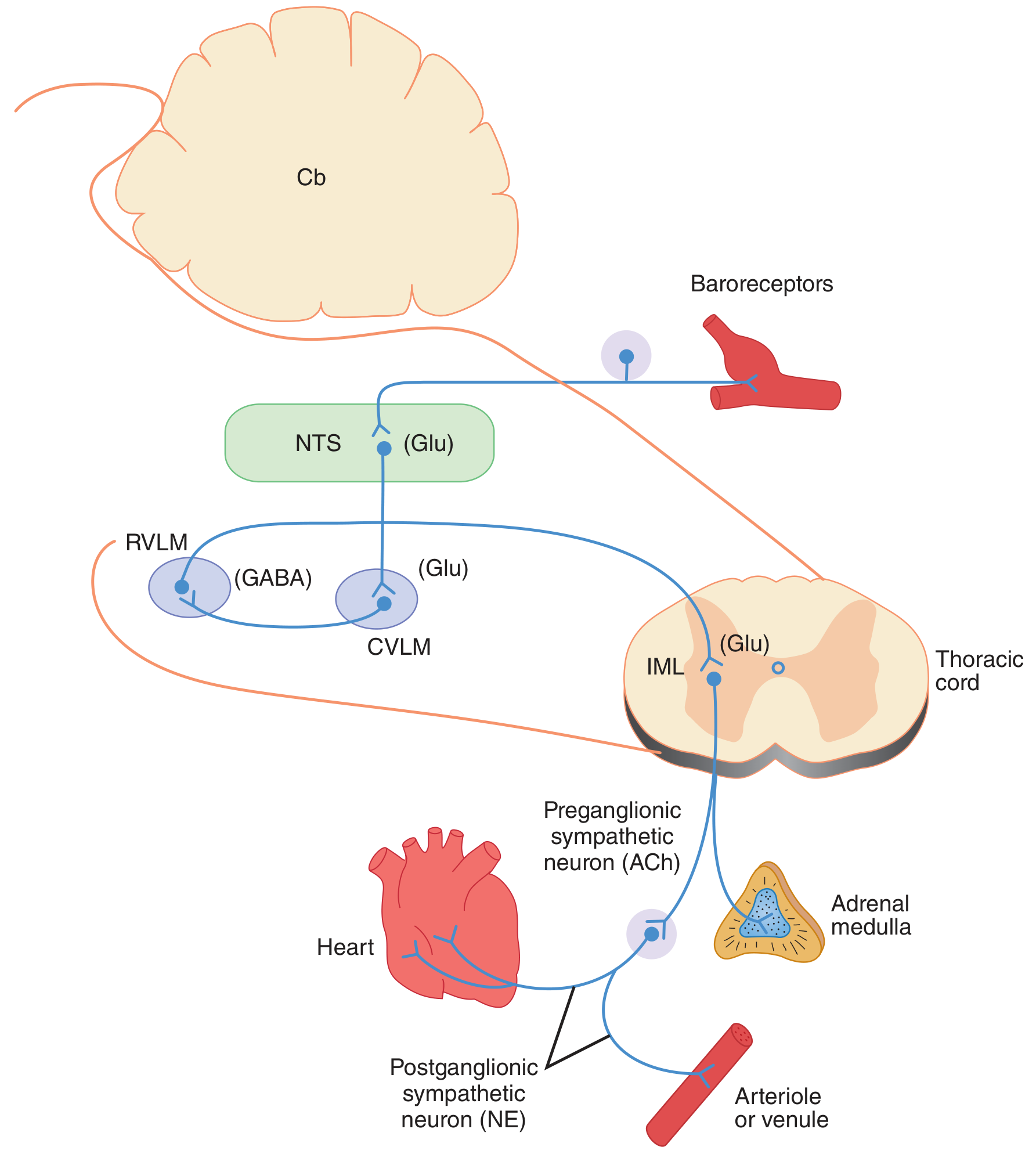
The RVLM is the primary tonic driver of sympathetic outflow to the cardiovascular system. Its neurons:
- Send axons that course dorsally and medially, then descend in the lateral column of the spinal cord to the thoracolumbar intermediolateral cell column (IML)
- Activate preganglionic sympathetic neurons in the IML using glutamate as their excitatory neurotransmitter
- Contain the enzyme phenylethanolamine-N-methyltransferase (PNMT) (marker of adrenergic neurons)
Effects of RVLM Activation
- Increased heart rate (via sympathetic fibers to SA node)
- Increased myocardial contractility (positive inotropy)
- Arteriolar vasoconstriction - raises total peripheral resistance (TPR)
- Venoconstriction - increases venous return and preload
- Net effect: raised blood pressure
"One of the major sources of excitatory input to sympathetic nerves controlling the vasculature is a group of neurons located near the pial surface of the medulla in the rostral ventrolateral medulla (RVLM). The axons of RVLM neurons course dorsally and medially and then descend in the lateral column of the spinal cord to the thoracolumbar intermediolateral cell column (IML)... glutamate is the excitatory transmitter they secrete to activate preganglionic sympathetic neurons."
- Ganong's Review of Medical Physiology, 26th Edition
Inputs to RVLM
The RVLM receives signals from multiple sources:
| Input Source | Effect on RVLM |
|---|---|
| Limbic cortex → Hypothalamus | Excitation (emotions: fear, anger, stress raise BP) |
| Baroreceptors (via CVLM/GABA) | Inhibition (high BP suppresses RVLM) |
| Carotid/aortic chemoreceptors | Excitation (hypoxia activates RVLM) |
| Pain afferents | Usually excitation (acute pain raises BP) |
| Lung inflation (vagal afferents) | Inhibition (causes vasodilation) |
| Exercise muscle afferents | Excitation (somatosympathetic reflex) |
CVLM - Caudal Ventrolateral Medulla
Location
Located in the caudal (lower) portion of the ventrolateral medulla, below the RVLM.
What It Does
The CVLM is an inhibitory relay station interposed between the NTS and the RVLM. Its neurons:
- Receive excitatory (glutamatergic) input from the nucleus tractus solitarius (NTS)
- Release GABA (gamma-aminobutyric acid) onto RVLM neurons - inhibiting them
- Act as the critical "off switch" for sympathetic drive
Effects of CVLM Activation
- Inhibits RVLM → reduces sympathetic outflow
- Decreases HR and contractility
- Produces vasodilation and venodilation
- Net effect: lowered blood pressure
"These NTS neurons then excite neurons in the caudal ventrolateral medulla (CVLM). These CVLM neurons release the inhibitory neurotransmitter γ-aminobutyric acid (GABA) into the RVLM to reduce the firing rate of these [RVLM neurons]."
- Ganong's Review of Medical Physiology, 26th Edition
How They Work Together: The Full Baroreceptor Reflex Circuit
This is the complete neural pathway, with RVLM and CVLM at the core:
When BP Rises (e.g., exercise, stress):
Baroreceptors ↑ firing
↓ (CN IX / X, Glutamate)
NTS activated
↓ (Glutamate - excitatory)
CVLM activated
↓ (GABA - inhibitory)
RVLM inhibited
↓
Sympathetic outflow ↓ + Vagal outflow ↑
↓
HR ↓, Contractility ↓, TPR ↓
↓
BP returns toward normal
When BP Falls (e.g., haemorrhage, standing up):
Baroreceptors ↓ firing
↓
NTS less active
↓
CVLM less active (less GABA onto RVLM)
↓
RVLM disinhibited (becomes more active)
↓
Sympathetic outflow ↑ + Vagal outflow ↓
↓
HR ↑, Contractility ↑, TPR ↑
↓
BP restored
"The activation of RVLM presympathetic neurons in response to hypotension is thus predominantly due to disinhibition."
- Harrison's Principles of Internal Medicine, 22nd Edition
This is a key exam point: when BP drops, RVLM is not directly activated - it is disinhibited (the CVLM brake is released).
Summary Comparison
| Feature | RVLM | CVLM |
|---|---|---|
| Location | Rostral (upper) VLM | Caudal (lower) VLM |
| Also known as | C1 area / Vasoconstrictor area (pressor area) | Depressor area |
| Neurotransmitter released | Glutamate (to IML) | GABA (to RVLM) |
| Effect on sympathetic outflow | Increases it | Decreases it (by inhibiting RVLM) |
| Effect on BP | Raises BP | Lowers BP |
| Receives input from | NTS, hypothalamus, cortex, chemoreceptors | NTS (glutamatergic) |
| Projects to | IML of thoracic spinal cord | RVLM |
| Tonic activity | Yes - maintains resting sympathetic tone | Yes - tonically inhibits RVLM |
| Clinical relevance | Overactive in neurogenic hypertension; target for renal denervation | Dysfunction may contribute to orthostatic hypotension |
- Ganong's Review of Medical Physiology, 26th Edition
- Comprehensive Clinical Nephrology, 7th Edition
- Harrison's Principles of Internal Medicine, 22nd Edition
So VMC present RVLM?
Yes, essentially. Here is the precise relationship:
VMC vs RVLM - Same Region, Different Level of Detail
The Vasomotor Centre (VMC) is the older, broader, classical term used in physiology textbooks (especially Guyton). It refers to the entire medullary cardiovascular control region.
The RVLM is the modern, more precise anatomical term that identifies the specific subregion within the VMC that generates sympathetic pressor drive.
How They Map to Each Other
| Classical VMC Subdivision | Modern Anatomical Term | Function |
|---|---|---|
| Vasoconstrictor area (lateral VMC) | RVLM | Pressor - raises BP, increases HR |
| Vasodilator area (lower VMC) | CVLM | Depressor - inhibits RVLM, lowers BP |
| Sensory/integrating area | NTS (Nucleus Tractus Solitarius) | Receives baroreceptor input, relays to CVLM/RVLM |
So when Guyton says:
"The lateral portions of the vasomotor center transmit excitatory impulses through sympathetic nerve fibers to increase heart rate and contractility"
...he is describing what Ganong calls the RVLM.
Think of It This Way
VMC (broad classical term)
├── Vasoconstrictor area = RVLM (pressor, sympathetic driver)
├── Vasodilator area = CVLM (depressor, GABAergic brake)
└── Sensory area = NTS (baroreceptor integrator)
- Older textbooks (Guyton, Sembulingam) use VMC and its subdivisions
- Newer/research-oriented texts (Ganong, Harrison's) use RVLM/CVLM as specific anatomical labels
Both are correct - the RVLM is the vasoconstrictor area of the VMC, described with greater anatomical precision.
This is a shared conversation. Sign in to Orris to start your own chat.