post antibiotics effect
Reading File
Searching the Web
post-antibiotic effect mechanism clinical significance
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a thorough breakdown of the Post-Antibiotic Effect (PAE):
Post-Antibiotic Effect (PAE)
Definition
PAE is the persistent suppression of bacterial growth that continues after antibiotic concentrations fall below the Minimum Inhibitory Concentration (MIC). It reflects lingering bacteriostatic or bactericidal activity even when the drug is no longer present at inhibitory levels.
Mathematical Formula:
PAE = T - C
- T = time for the viable bacterial count in the drug-exposed culture to increase 10-fold above the count immediately after drug removal
- C = time for the count in an untreated control culture to increase 10-fold
The PAE thus quantifies how long bacteria are delayed in returning to logarithmic growth after drug exposure.
(Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 1417)
Proposed Mechanisms
Three main mechanisms have been identified:
- Slow recovery from reversible, non-lethal damage to bacterial cell structures (e.g., membrane disruption, ribosomal injury)
- Persistence of the drug at a binding site or within the periplasmic space, continuing to exert effect even after serum levels drop
- Need to synthesize new enzymes before bacterial growth can resume (e.g., after drug has inhibited transcription or translation machinery)
(Katzung's, p. 1417-1418)
In Vitro vs. In Vivo PAE
| Setting | Duration |
|---|---|
| In vitro | Shorter |
| In vivo | Longer (often significantly) |
Why is in vivo PAE longer?
Two additional factors amplify PAE in the body:
- Post-Antibiotic Leukocyte Enhancement (PALE): Bacteria weakened by the antibiotic are more susceptible to phagocytosis by white blood cells
- Subinhibitory antibiotic concentrations: Even after falling below MIC, residual drug concentrations continue to contribute to bacterial suppression
Relationship to Kill Characteristics
| Kill Pattern | PAE |
|---|---|
| Concentration-dependent (aminoglycosides, fluoroquinolones) | Strong, prolonged PAE |
| Time-dependent (beta-lactams, carbapenems) | Minimal to moderate PAE |
| AUC/MIC-dependent (vancomycin, daptomycin) | Variable |
Note: Macrolides (e.g., azithromycin) are an exception - they are time-dependent killers but have a long PAE, likely because they suppress bacterial growth rather than causing cell lysis. (Goldman-Cecil Medicine)
Antibiotics with PAE >= 1.5 Hours (In Vitro)
Against Gram-Positive Cocci:
Aminoglycosides, Carbapenems, Cephalosporins, Chloramphenicol, Clindamycin, Daptomycin, Glycopeptides (vancomycin), Ketolides, Macrolides, Oxazolidinones, Penicillins, Quinolones, Rifampin, Streptogramins, Sulfonamides, Tetracyclines, Tigecycline, Trimethoprim
Against Gram-Negative Bacilli (more selective):
Aminoglycosides, Carbapenems, Chloramphenicol, Quinolones, Rifampin, Tetracyclines, Tigecycline
(Katzung's, p. 1418)
Clinical Significance - Dosing Implications
The PAE is a key pharmacodynamic concept that directly informs dosing schedules:
-
Once-daily aminoglycosides: Exploit both concentration-dependent killing and prolonged PAE. A high peak dose achieves maximal bacterial kill; then the PAE maintains suppression even as serum levels drop below MIC. This also reduces the trough concentration, minimizing nephrotoxicity. (Goodman & Gilman's; Fishman's Pulmonary Diseases, p.)
-
Fluoroquinolones: Concentration-dependent PAE against both Gram-positive and Gram-negative organisms allows once- or twice-daily dosing.
-
Beta-lactams: Have minimal or no PAE against Gram-negatives. Therefore, they must be dosed frequently or given as continuous/extended infusions to keep concentrations above MIC throughout the dosing interval.
-
Rifampin: Shows long, concentration-dependent PAE because its macrocyclic ring binds stably and irreversibly to the beta subunit of DNA-dependent RNA polymerase (rpoB) - the complex is slowly reversed. (Goodman & Gilman's, p. 1152)
-
TB intermittent dosing: Takes advantage of the slow growth of M. tuberculosis and PAE of anti-TB drugs to allow intermittent regimens (though acquired resistance is a risk, especially in HIV). (Fishman's)
Post-Antibiotic Sub-MIC Effect (PA SME)
A related concept - bacteria exposed to sub-inhibitory concentrations of antibiotics (concentrations below MIC but above zero) after a full drug exposure show enhanced susceptibility to the drug. This further extends the effective duration of bacterial suppression beyond even the PAE window.
Summary Table
| Feature | Details |
|---|---|
| Definition | Persistent bacterial suppression after drug falls below MIC |
| Formula | PAE = T - C |
| Mechanisms | Cell structure damage, drug persistence at binding site, need for new enzyme synthesis |
| Strongest PAE | Aminoglycosides, Fluoroquinolones, Rifampin |
| Weakest PAE vs. GNR | Beta-lactams (penicillins, cephalosporins) |
| In vivo amplifiers | PALE (leukocyte enhancement), sub-MIC residual drug |
| Clinical use | Guides once-daily dosing; extends dosing intervals safely |
MOA of chloroquine
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Here is a detailed breakdown of the Mechanism of Action of Chloroquine, sourced from authoritative pharmacology textbooks:
Mechanism of Action of Chloroquine
Drug Class
Chloroquine is a synthetic 4-aminoquinoline that acts primarily on the erythrocytic (blood) stage of Plasmodium infection.
Step-by-Step Mechanism
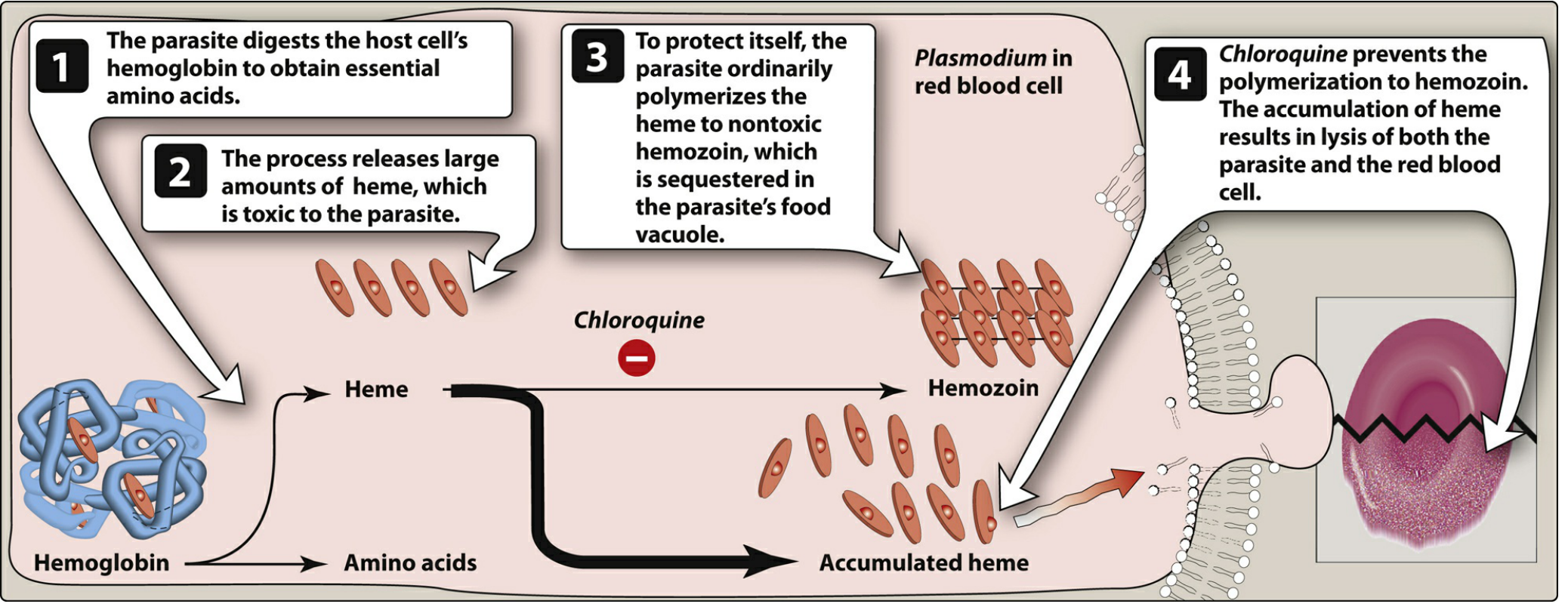
Figure: Action of chloroquine on the formation of hemozoin by Plasmodium species (Lippincott Pharmacology)
Step 1 - Hemoglobin digestion:
The Plasmodium parasite (inside the red blood cell) digests the host cell's hemoglobin in its food vacuole to obtain the essential amino acids it needs for growth and replication.
Step 2 - Toxic heme release:
This digestion releases large amounts of free heme (ferriprotoporphyrin IX), which is highly toxic to the parasite itself - it disrupts membranes and generates reactive oxygen species.
Step 3 - Normal parasite defense (hemozoin formation):
To protect itself, the parasite normally polymerizes heme into hemozoin (malaria pigment) - a non-toxic, insoluble crystal that is safely sequestered within the food vacuole.
Step 4 - Chloroquine's action:
Chloroquine, being a diprotic weak base, enters the erythrocyte and crosses into the parasite. It becomes ion-trapped and concentrated in the acidic food vacuole (pH ~5.0), reaching concentrations many times higher than in the plasma. There, it binds specifically to free heme, physically blocking its polymerization into hemozoin.
Result:
- Free heme accumulates in the food vacuole
- Heme causes oxidative damage to the phospholipid membranes
- This leads to lysis of both the parasite and the red blood cell
(Lippincott Illustrated Reviews: Pharmacology, p. 1170-1171)
Key Pharmacodynamic Concept: Ion Trapping
Chloroquine is a weak diprotic base (pKa ~8.1 and 10.2). In the acidic food vacuole of the parasite:
- It becomes di-protonated (charged)
- Charged molecules cannot cross lipid membranes back out
- This results in concentration 1000x higher inside the vacuole than in the surrounding cytoplasm
This ion-trapping mechanism is also responsible for raising the pH of the vacuole, which itself impairs hemoglobin digestion.
Additional MOA: Immunomodulation (Non-malarial Uses)
When used in autoimmune diseases (SLE, rheumatoid arthritis), chloroquine and its analogue hydroxychloroquine work by:
- Inhibiting lysosomal enzymes - by raising lysosomal pH, it impairs antigen processing and presentation
- Blocking Toll-like receptor (TLR) signaling - particularly TLR7 and TLR9, which recognize nucleic acids and drive autoimmune inflammation
- Suppressing pro-inflammatory cytokines (IL-1, IL-6, TNF-alpha) by inhibiting cytokine release from monocytes
- Reducing antigen-antibody complex formation and complement activation
(Firestein & Kelley's Textbook of Rheumatology)
Resistance Mechanism
P. falciparum resistance to chloroquine is due to mutations in the PfCRT gene (Plasmodium falciparum Chloroquine Resistance Transporter). The mutant CRT protein pumps chloroquine out of the food vacuole, preventing it from accumulating to toxic concentrations. This is the primary mechanism behind widespread chloroquine resistance, now seen in almost all malaria-endemic areas.
Summary Table
| Feature | Detail |
|---|---|
| Drug class | 4-aminoquinoline |
| Target stage | Erythrocytic (blood) stage of Plasmodium |
| Site of action | Acidic food vacuole of the parasite |
| Primary target | Heme polymerization (hemozoin formation) |
| Key mechanism | Ion trapping → heme accumulation → oxidative membrane lysis |
| Secondary (autoimmune) | Lysosomal pH raising, TLR inhibition, cytokine suppression |
| Resistance | PfCRT mutation - efflux pump removes drug from food vacuole |
| Active against | P. vivax, P. ovale, P. malariae; NOT resistant P. falciparum |
This is a shared conversation. Sign in to Orris to start your own chat.