Create an answer for md forensic medicine exam , on the topic “ foetal development and its Medicolegal significance for 20 marks and foetal circulation and its Medicolegal importance for 20 marks “ . Suggest diagrams and flow charts and skeletal diagrams
MD Forensic Medicine Exam Answer
QUESTION 1: Foetal Development and Its Medicolegal Significance (20 Marks)
INTRODUCTION
PART A: FOETAL DEVELOPMENT - STAGES AND MILESTONES
1. Embryonic Period (Weeks 1-8)
2. Foetal Period (Weeks 9 to Birth)
DIAGRAM 1: Suggested Flow Chart - Foetal Development Milestones
FERTILISATION (Week 0)
│
▼
ZYGOTE → MORULA → BLASTOCYST (Week 1)
│
▼
IMPLANTATION (Week 2)
│
▼
EMBRYONIC DISC formed (Week 3)
│
▼
ALL ORGAN SYSTEMS initiated (Weeks 4-8)
Heart beats, limb buds appear, crown-rump length ~3 cm
│
▼
FOETAL PERIOD BEGINS (Week 9)
│
┌────┴──────────────────────────────────────────────────────┐
│ MILESTONES TABLE │
├──────────────┬───────────┬───────────┬────────────────────┤
│ Age (weeks) │ Length │ Weight │ Key Milestone │
├──────────────┼───────────┼───────────┼────────────────────┤
│ 12 │ 8 cm │ 45 g │ Ossification begins│
│ │ │ │ Sex determinable │
├──────────────┼───────────┼───────────┼────────────────────┤
│ 16 │ 14 cm │ 110 g │ Quickening felt │
│ │ │ │ Scalp hair appears │
├──────────────┼───────────┼───────────┼────────────────────┤
│ 20 │ 20 cm │ 340 g │ Vernix caseosa │
│ │ │ │ Lanugo hair │
│ │ │ │ Eyebrows, lashes │
├──────────────┼───────────┼───────────┼────────────────────┤
│ 24 │ 28 cm │ 600 g │ Eyelids fused │
│ │ │ │ Viable (limit) │
├──────────────┼───────────┼───────────┼────────────────────┤
│ 28 │ 35 cm │ 1200 g │ Eyes open │
│ │ │ │ Legally viable │
├──────────────┼───────────┼───────────┼────────────────────┤
│ 32 │ 40 cm │ 1800 g │ Testes descend │
│ │ │ │ (Males) │
├──────────────┼───────────┼───────────┼────────────────────┤
│ 36 │ 45 cm │ 2400 g │ Subcutaneous fat │
│ │ │ │ Nails reach tips │
├──────────────┼───────────┼───────────┼────────────────────┤
│ 38 (Term) │ 50 cm │ 3200 g │ Full-term baby │
└──────────────┴───────────┴───────────┴────────────────────┘
Memory Aid (Haase's Rule): Crown-to-heel length = Month² (for months 1-5) and Month × 5 (for months 5-10). E.g., at month 5: length = 5 × 5 = 25 cm.
PART B: OSSIFICATION CENTRES - KEY FOR AGE ESTIMATION
DIAGRAM 2: Suggested Skeletal Diagram - Ossification Centres (Medicolegal Importance)
OSSIFICATION CENTRE CHART
┌──────────────────────────────────────────────────────────┐
│ AGE │ OSSIFICATION CENTRE │ SIGNIFICANCE │
├──────────────┼───────────────────────────┼───────────────┤
│ 7th month │ Lower femoral epiphysis │ Proof of 7+ │
│ (28 weeks) │ (Béclard's point) │ months, legal │
│ │ Size: 5-6 mm │ viability │
├──────────────┼───────────────────────────┼───────────────┤
│ 9th month │ Upper tibial epiphysis │ Proof of 9+ │
│ (36 weeks) │ (Poland's point) │ months, near │
│ │ Size: 3-4 mm │ term │
├──────────────┼───────────────────────────┼───────────────┤
│ Birth │ Calcaneus, talus, │ Maturity │
│ │ cuboid present │ │
├──────────────┼───────────────────────────┼───────────────┤
│ 3-6 months │ Head of humerus appears │ Postnatal age │
└──────────────┴───────────────────────────┴───────────────┘
KEY FORENSIC OSSIFICATION POINTS:
Skull
├── Frontal bone (2 centres, ossification by 8th month)
├── Parietal bones (present from 3rd month)
└── Sphenoid (partially ossified at term)
Long Bones
├── Femur shaft ossifies: 7th week of embryonic life
├── Lower femoral epiphysis: 36 weeks (BÉCLARD'S POINT ★)
└── Upper tibial epiphysis: 38-40 weeks (POLAND'S POINT ★)
★ = most important medicolegal ossification landmarks
PART C: EXTERNAL FEATURES FOR ESTIMATING FOETAL AGE
| Feature | Approx. Age |
|---|---|
| Eyelids sealed (fused) | 9-26 weeks |
| Eyelids open | 26-28 weeks |
| Lanugo (fine downy hair) | 20-28 weeks; shed by 36 weeks |
| Vernix caseosa appears | 20 weeks; shed by 40 weeks |
| Ear cartilage soft/absent | <36 weeks |
| Ear cartilage firm, springs back | >36 weeks (maturity) |
| Sole creases (deep) | >38 weeks |
| Nails reaching fingertips | >36 weeks |
| Testes in scrotum | >36 weeks (male) |
| Labia majora covering minora | >36 weeks (female) |
| Breast nodule >5 mm | Term (>38 weeks) |
PART D: MEDICOLEGAL SIGNIFICANCE OF FOETAL DEVELOPMENT
1. Determination of Gestational Age
- Viability - whether a born child could have lived (legally defined as >28 weeks or >1000 g in most jurisdictions)
- Maturity - relevant in infanticide cases (was the child capable of independent existence?)
- Date of conception - relevant to legitimacy, paternity disputes, and cases of sexual assault
2. Proof of Live Birth vs. Stillbirth
3. Infanticide
- The infant was alive and term
- It was a newborn and not an older infant
4. Abortion - Criminal and Legal Aspects
FLOW CHART: ABORTION - MEDICOLEGAL FRAMEWORK
┌─────────────────────────────────────────────────────────┐
│ ABORTION │
│ (Expulsion of conceptus before viability) │
│ i.e., before 28 weeks │
└───────────────────┬─────────────────────────────────────┘
│
┌─────────┴─────────┐
▼ ▼
SPONTANEOUS INDUCED/CRIMINAL
(Miscarriage)
│
┌───────────────┼───────────────┐
▼ ▼ ▼
LEGAL ILLEGAL THERAPEUTIC
(MTP Act) (Criminal) (Medical grounds)
<20 weeks Any time <20 weeks
<24 weeks
(RCH 2021)
│
▼
FORENSIC EVIDENCE SOUGHT:
- Foetal parts in uteri/drains
- Age of foetus (to confirm abortion)
- Signs of instrumentation
- Drugs/chemicals used
- Products of conception
5. Viability
- Crown-heel length (>35 cm suggests >28 weeks)
- Weight (>1000 g for viability)
- Béclard's ossification centre (lower femoral epiphysis, 36 weeks)
- Lung maturity markers (lecithin:sphingomyelin ratio)
6. Legitimacy and Paternity
- Minimum gestation: 210 days (7 months) - the "viable minimum"
- Maximum gestation: 280-300 days (10 months); courts have accepted up to 349 days in exceptional circumstances (British case of Hadlum v Hadlum, 1949)
- Foetal age assessment helps determine whether conception occurred within a marriage, helping or refuting legitimacy claims
7. Concealment of Birth
8. Exhumation Cases
- They survive putrefaction
- They are not affected by maceration
- Béclard's and Poland's points can be detected even in skeletonised remains
9. Battered Baby Syndrome / Non-Accidental Injury
- Multiple healing fractures at different stages
- Metaphyseal chip fractures
- Subdural haemorrhage Age of fractures can be estimated from callus formation, helping reconstruct the timeline of abuse.
10. Determination of Full Term vs. Premature Birth
QUESTION 2: Foetal Circulation and Its Medicolegal Importance (20 Marks)
INTRODUCTION
DIAGRAM 3: Foetal Circulation (Textbook Diagram)
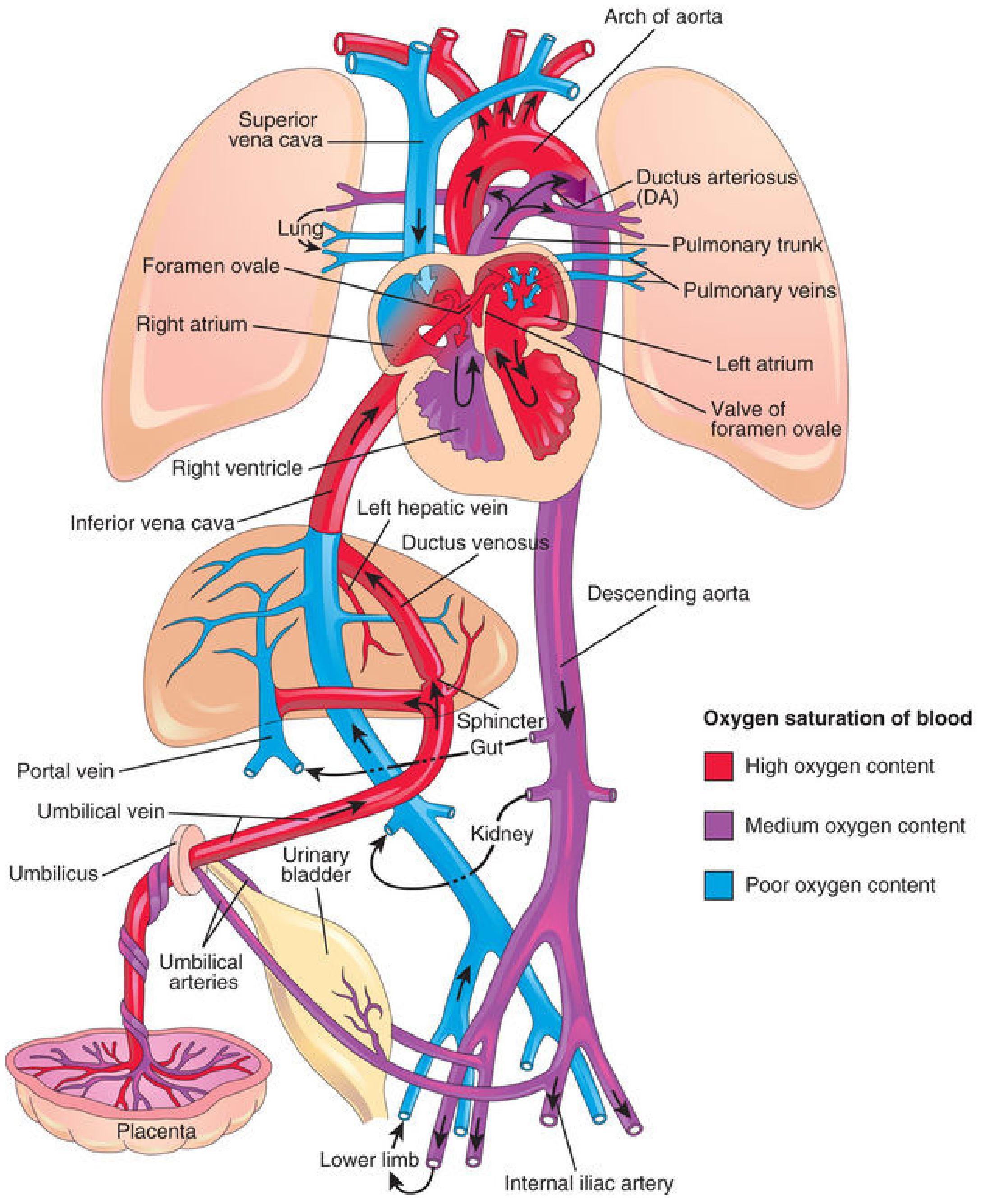
PART A: ANATOMY AND PHYSIOLOGY OF FOETAL CIRCULATION
Blood Flow Pathway
FLOW CHART: FOETAL CIRCULATION
PLACENTA
(Gas exchange occurs here)
│
▼ (Oxygenated blood)
UMBILICAL VEIN (1 vein, O₂-rich)
│
┌───────┴───────────┐
▼ (50%) ▼ (50%)
DUCTUS VENOSUS HEPATIC SINUSOIDS
(bypasses liver) (portal circulation)
│ │
└─────────┬──────────┘
▼
INFERIOR VENA CAVA (IVC)
(mixed blood - medium O₂)
│
▼
RIGHT ATRIUM
│
┌──────────┴──────────────┐
▼ ▼
FORAMEN OVALE RIGHT VENTRICLE
(2/3 blood shunts (1/3 blood)
to left atrium) │
│ ▼
▼ PULMONARY TRUNK
LEFT ATRIUM │
│ ┌─────────┴──────────┐
▼ ▼ (10%) ▼ (90%)
LEFT VENTRICLE LUNGS DUCTUS ARTERIOSUS
│ (minimal flow) (bypasses lungs)
▼ │
ASCENDING AORTA ▼
│ DESCENDING AORTA
▼ │
Head, Neck, ┌──────────────┼─────────────┐
Upper limbs ▼ ▼ ▼
(Well-oxygenated) VISCERA LOWER LIMBS UMBILICAL ARTERIES (2)
│
▼
PLACENTA
(Deoxygenated blood
returns for re-oxygenation)
The Three Shunts - Detail
| Shunt | Connects | Function | Adult Remnant |
|---|---|---|---|
| Ductus venosus | Umbilical vein → IVC | Bypasses liver; delivers oxygenated blood directly to heart | Ligamentum venosum |
| Foramen ovale | Right atrium → Left atrium | Shunts oxygenated IVC blood to systemic circulation, bypassing lungs | Fossa ovalis |
| Ductus arteriosus | Pulmonary trunk → Descending aorta | Diverts right ventricular output away from vasoconstricted lungs | Ligamentum arteriosum |
Umbilical Vessels
| Vessel | Number | Contents | Adult Remnant |
|---|---|---|---|
| Umbilical vein | 1 | Oxygenated blood FROM placenta | Ligamentum teres hepatis (round ligament of liver) |
| Umbilical arteries | 2 | Deoxygenated blood TO placenta | Medial umbilical ligaments (superior vesical arteries retain patency) |
Mnemonic: "AVA" in the umbilical cord - Artery, Vein, Artery (2 arteries, 1 vein)
PART B: TRANSITIONAL CIRCULATION AT BIRTH
Diagram 4: Neonatal Circulation (Textbook Diagram)
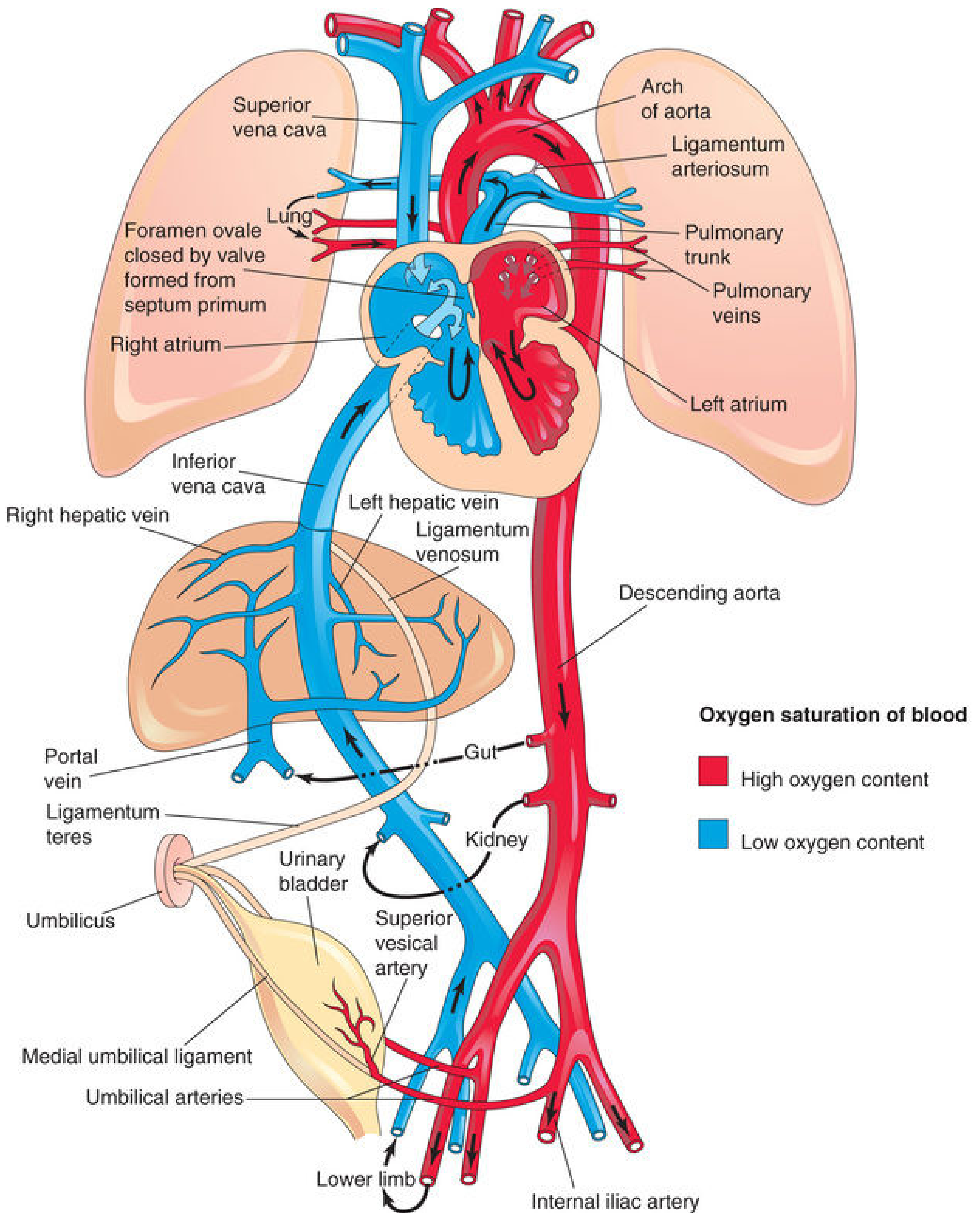
Changes at Birth - Flow Chart
FIRST BREATH
│
▼
Lungs expand → Pulmonary vascular resistance FALLS markedly
│
▼
Pulmonary blood flow INCREASES
│
▼
Left atrial pressure > Right atrial pressure
│
┌──────┴──────┐
▼ ▼
FORAMEN OVALE DUCTUS ARTERIOSUS
functionally blood flow REVERSES
closes (aorta → pulmonary trunk)
(valve pressed High O₂ + Low PGE₂ →
against septum muscular constriction
secundum) │
▼
Permanent fibrous closure
by 2-3 months (becomes
Ligamentum arteriosum)
UMBILICAL CIRCULATION:
│
▼
Cord clamped → Umbilical arteries constrict immediately
Umbilical vein closes within minutes
Ductus venosus sphincter constricts
│
▼
All placental blood now enters hepatic sinusoids
Timeline of Shunt Closure
| Event | Timing |
|---|---|
| Foramen ovale - functional closure | At birth (first breath) |
| Foramen ovale - anatomical closure | 3 months to 1 year |
| Patent Foramen Ovale (PFO) persists | 25-30% of adults (normal variant) |
| Ductus arteriosus - functional closure | 24-48 hours post-birth |
| Ductus arteriosus - 20% closed | End of 24 hours |
| Ductus arteriosus - 80% closed | End of 48 hours |
| Ductus arteriosus - 100% closed | 96 hours (4 days) |
| Ductus arteriosus - permanent (ligamentum arteriosum) | 2-3 months |
| Ductus venosus | Within hours of birth |
| Umbilical vein | Within minutes of birth |
PART C: MEDICOLEGAL IMPORTANCE OF FOETAL CIRCULATION
1. HYDROSTATIC TEST (DOCIMASIA PULMONUM) - Most Important Forensic Application
HYDROSTATIC TEST - FLOW CHART
Take lungs from dead neonate
│
▼
Place in water
│
┌──────┴──────────┐
▼ ▼
FLOAT SINK
│ │
▼ ▼
Child BREATHED Child DID NOT
after birth BREATHE / stillborn
(Live birth (Suggests intrauterine
established) death or stillbirth)
│
▼
Subdivide lung lobes
│
▼
Each subdivision floats? → Confirms aeration
│
▼
Microscopy: alveoli expanded?
→ Confirms liveborn
- Putrefaction gases can cause a stillborn's lung to float (false positive)
- Manual compression can squeeze air out of a liveborn's lung (false negative)
- Resuscitation attempts (CPR) can introduce air even without birth
2. Patent Ductus Arteriosus (PDA) - Neonatal Death
- Causes left-to-right shunting → pulmonary oedema → respiratory failure
- A premature neonate dying of respiratory distress syndrome (RDS) will show a patent DA at autopsy
- This finding establishes prematurity and may be relevant in negligence cases (failure to close DA pharmacologically with indomethacin)
3. Persistent Foetal Circulation (PFC) / Persistent Pulmonary Hypertension of the Newborn (PPHN)
- Ductus arteriosus remains open with right-to-left shunting
- Foramen ovale may reopen with right-to-left shunting
- Severe hypoxaemia and metabolic acidosis ensue
PPHN - FORENSIC SIGNIFICANCE CHART:
PPHN found at autopsy
│
▼
CAUSES:
├── Meconium aspiration (birth asphyxia)
├── Sepsis (Group B Streptococcus)
├── Congenital heart disease
├── Diaphragmatic hernia
└── Idiopathic
│
▼
MEDICOLEGAL IMPLICATION:
Was PPHN due to negligent management?
- Failure to resuscitate → birth asphyxia → PPHN
- Missed sepsis → uncontrolled infection → PPHN
4. Live Birth vs. Stillbirth - Umbilical Cord Evidence
| Finding | Significance |
|---|---|
| Fresh cut / torn cord | Live birth possible; infanticide suspected |
| Naturally separated / ligated cord | Normal neonatal care occurred |
| Thrombosis in umbilical vessels | Intrauterine death |
| Wharton's jelly intact | Recent birth |
| Cord blood available | DNA identification, metabolic disorders |
| Single umbilical artery (only one artery) | Associated with renal agenesis; Potter sequence |
5. Sudden Unexpected Death in Infancy (SUDI) / SIDS
- HbF present in blood in the first months of life: can establish age at death
- PFO present in ~25% of the population and is NOT considered a cause of SIDS in isolation
- Right-to-left shunting via PFO during hypoxic/cyanotic episodes may contribute to paradoxical embolism
6. Congenital Heart Disease (CHD) and Neonatal Death
| CHD | Reason tolerated in utero | What happens at birth |
|---|---|---|
| Transposition of great arteries | Both circuits deliver mixed blood via shunts | Shunts close → no mixing → death |
| Hypoplastic left heart | Right ventricle handles all output | Left ventricle must function → cardiac failure |
| Coarctation of aorta | Ductus arteriosus maintains lower body perfusion | DA closes → lower body ischaemia |
| Pulmonary atresia | DA feeds pulmonary circulation | DA closes → severe hypoxia |
7. Erythroblastosis Fetalis / Haemolytic Disease of the Newborn (HDN)
- Severe haemolysis causes hydrops fetalis (severe foetal oedema)
- High-output cardiac failure with massive hepatosplenomegaly
- The placenta shows villous oedema and hyperplasia
- Autopsy findings: enlarged heart, oedematous organs, pale liver, severe anaemia
8. Birth Asphyxia and Foetal Circulation
- Pulmonary vasoconstriction → persistent foetal circulation
- Hypoxic-ischaemic encephalopathy (HIE) → brain injury
- Meconium passage (foetal distress marker)
- Right-to-left shunting perpetuates hypoxia
- Bilateral adrenal haemorrhage (stress response)
- Petechiae on thymic surface (classic Tardieu's spots)
- Pulmonary haemorrhage / haemorrhagic congestion
- Patent DA (sign of persistence of foetal pattern)
SUMMARY TABLES
Table 1: Foetal Structures and Adult Remnants
| Foetal Structure | Function | Adult Remnant |
|---|---|---|
| Ductus venosus | Bypasses liver | Ligamentum venosum |
| Foramen ovale | Bypasses lungs (R→L shunt) | Fossa ovalis |
| Ductus arteriosus | Bypasses lungs (pulm trunk→aorta) | Ligamentum arteriosum |
| Umbilical vein | O₂-rich blood from placenta | Ligamentum teres hepatis |
| Umbilical arteries | Deoxygenated blood to placenta | Medial umbilical ligaments |
| Allantois | Urine drainage | Median umbilical ligament (urachus) |
Table 2: Summary of Medicolegal Significance
| Topic | Medicolegal Issue |
|---|---|
| Foetal age/development | Abortion law, viability, legitimacy, identification |
| Béclard's ossification point | 36 weeks gestation (maturity, legal viability) |
| Hydrostatic test | Live birth vs. stillbirth (infanticide charges) |
| Umbilical cord findings | Live birth, infanticide, intrauterine death |
| Patent DA at autopsy | Prematurity, negligence, RDS |
| PPHN | Birth asphyxia, medical negligence |
| Congenital heart disease | Antenatal care negligence, neonatal death |
| Foetal haemoglobin | Age at death (forensic biochemistry) |
IMPORTANT MEDICOLEGAL DEFINITIONS
- Viability: The capacity of the foetus to survive independently outside the uterus. In India (MTP Act): 20 weeks; legally: 28 weeks; WHO: 22-24 weeks.
- Stillbirth: Birth of a baby after 28 weeks of gestation with no signs of life. Must be registered but no birth certificate.
- Live birth (WHO): Any product of conception that, after expulsion, shows any evidence of life (heartbeat, respiratory effort, pulsation of cord, voluntary muscle movement).
- Infanticide: Unlawful killing of a newborn child. If done by the mother within 12 months of birth, it may be charged under the Infanticide Act.
- Béclard's ossification centre: Ossification centre in the lower femoral epiphysis, appears at 36 weeks. Its presence confirms a gestational age of at least 8-9 months.
TIPS FOR DIAGRAMS TO DRAW IN EXAM
- Foetal circulation flowchart (umbilical vein → ductus venosus → IVC → right atrium → foramen ovale → left side OR ductus arteriosus → aorta → umbilical arteries)
- Skeleton diagram showing Béclard's (lower femoral epiphysis) and Poland's (upper tibial epiphysis) ossification centres with ages
- Hydrostatic test flowchart (lung floats/sinks → live birth/stillbirth)
- Foetal to neonatal transition table (ductus venosus → ligamentum venosum, etc.)
- PPHN cycle diagram (hypoxia → pulmonary vasoconstriction → right-to-left shunt → more hypoxia)
- Haase's rule diagram on a timeline (cm length vs. gestational month)
Create a quick reference PDF cheat sheet on ossification centres and medicolegal definitions
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace not found"
mkdir -p /home/daytona/workspace/forensic-cheatsheet && python3 -c "import reportlab; print('reportlab ok')"
~/forensic-cheatsheet/make_cheatsheet.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import mm, cm
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether
)
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.platypus import PageBreak
OUTPUT = "/home/daytona/workspace/forensic-cheatsheet/Forensic_Ossification_Cheatsheet.pdf"
# ── Colour palette ──────────────────────────────────────────────────────────
NAVY = colors.HexColor("#0D2B55")
CRIMSON = colors.HexColor("#B22222")
GOLD = colors.HexColor("#C8960C")
LTBLUE = colors.HexColor("#D6E8F7")
LTGOLD = colors.HexColor("#FFF8E1")
LTGREEN = colors.HexColor("#E8F5E9")
LTRED = colors.HexColor("#FFEBEE")
WHITE = colors.white
GREY = colors.HexColor("#F0F0F0")
DARKGREY = colors.HexColor("#555555")
MIDBLUE = colors.HexColor("#1A4F8A")
TEAL = colors.HexColor("#00695C")
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
leftMargin=12*mm, rightMargin=12*mm,
topMargin=12*mm, bottomMargin=12*mm,
title="Forensic Medicine Quick Reference – Ossification & Medicolegal Definitions",
author="Orris MD Forensics"
)
styles = getSampleStyleSheet()
def S(name, **kw):
"""Helper: clone a base style with overrides."""
base = styles["Normal"]
return ParagraphStyle(name, parent=base, **kw)
# ── Custom styles ────────────────────────────────────────────────────────────
TITLE_STYLE = S("Title",
fontSize=18, leading=22, textColor=WHITE,
fontName="Helvetica-Bold", alignment=TA_CENTER)
SUBTITLE_STYLE = S("Subtitle",
fontSize=10, leading=13, textColor=LTBLUE,
fontName="Helvetica", alignment=TA_CENTER)
SECTION_STYLE = S("Section",
fontSize=11, leading=14, textColor=WHITE,
fontName="Helvetica-Bold", alignment=TA_LEFT,
leftIndent=4, spaceBefore=6, spaceAfter=2)
SUBSECTION_STYLE = S("Subsection",
fontSize=9.5, leading=12, textColor=NAVY,
fontName="Helvetica-Bold", spaceBefore=4, spaceAfter=2)
BODY_STYLE = S("Body",
fontSize=8.5, leading=11.5, textColor=colors.black,
fontName="Helvetica", spaceAfter=2)
BULLET_STYLE = S("Bullet",
fontSize=8.5, leading=11.5, textColor=colors.black,
fontName="Helvetica", leftIndent=10, spaceAfter=1,
bulletIndent=4)
NOTE_STYLE = S("Note",
fontSize=7.5, leading=10, textColor=DARKGREY,
fontName="Helvetica-Oblique", leftIndent=6)
MNEMONIC_STYLE = S("Mnemonic",
fontSize=8.5, leading=11, textColor=TEAL,
fontName="Helvetica-Bold", leftIndent=6, spaceAfter=2)
HIGHLIGHT_STYLE = S("Highlight",
fontSize=8.5, leading=11.5, textColor=CRIMSON,
fontName="Helvetica-Bold")
TABLE_HDR = S("TableHdr",
fontSize=8, leading=10, textColor=WHITE,
fontName="Helvetica-Bold", alignment=TA_CENTER)
TABLE_CELL = S("TableCell",
fontSize=7.8, leading=10, textColor=colors.black,
fontName="Helvetica")
TABLE_CELL_BOLD = S("TableCellBold",
fontSize=7.8, leading=10, textColor=NAVY,
fontName="Helvetica-Bold")
TABLE_CELL_RED = S("TableCellRed",
fontSize=7.8, leading=10, textColor=CRIMSON,
fontName="Helvetica-Bold", alignment=TA_CENTER)
# ── Helpers ──────────────────────────────────────────────────────────────────
def section_header(title, bg=NAVY):
data = [[Paragraph(f" {title}", SECTION_STYLE)]]
t = Table(data, colWidths=[186*mm])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("ROWPADDING", (0,0), (-1,-1), 4),
("BOX", (0,0), (-1,-1), 0.5, GOLD),
]))
return t
def mini_header(title, bg=MIDBLUE):
data = [[Paragraph(f" {title}", S("mh", parent=SECTION_STYLE, fontSize=9, leading=12))]]
t = Table(data, colWidths=[186*mm])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("ROWPADDING", (0,0), (-1,-1), 3),
("BOX", (0,0), (-1,-1), 0.3, GOLD),
]))
return t
def make_table(headers, rows, col_widths, row_colors=None, stripe=True):
hdr_row = [Paragraph(h, TABLE_HDR) for h in headers]
data = [hdr_row]
for i, row in enumerate(rows):
styled = []
for j, cell in enumerate(row):
if isinstance(cell, tuple):
styled.append(Paragraph(cell[0], cell[1]))
else:
styled.append(Paragraph(str(cell), TABLE_CELL))
data.append(styled)
t = Table(data, colWidths=col_widths, repeatRows=1)
base_style = [
("BACKGROUND", (0,0), (-1,0), NAVY),
("GRID", (0,0), (-1,-1), 0.3, colors.HexColor("#CCCCCC")),
("ROWPADDING", (0,0), (-1,-1), 3),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
]
if stripe:
for i in range(1, len(data)):
bg = LTBLUE if i % 2 == 0 else WHITE
base_style.append(("BACKGROUND", (0,i), (-1,i), bg))
t.setStyle(TableStyle(base_style))
return t
def hr():
return HRFlowable(width="100%", thickness=0.5, color=GOLD, spaceAfter=3, spaceBefore=3)
# ─────────────────────────────────────────────────────────────────────────────
# PAGE 1 BUILD
# ─────────────────────────────────────────────────────────────────────────────
story = []
# ── Cover banner ─────────────────────────────────────────────────────────────
banner_data = [[
Paragraph("FORENSIC MEDICINE", TITLE_STYLE),
Paragraph("QUICK REFERENCE CHEAT SHEET", TITLE_STYLE),
]]
banner = Table([[Paragraph("FORENSIC MEDICINE | QUICK REFERENCE CHEAT SHEET", TITLE_STYLE)]],
colWidths=[186*mm])
banner.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), NAVY),
("ROWPADDING", (0,0), (-1,-1), 10),
("BOX", (0,0), (-1,-1), 1.5, GOLD),
]))
story.append(banner)
story.append(Paragraph(
"Ossification Centres for Age Estimation • Foetal Development Milestones • Medicolegal Definitions",
SUBTITLE_STYLE))
story.append(Spacer(1, 4*mm))
# ═══════════════════════════════════════════════════════════════════════════
# SECTION 1 – HAASE'S RULE
# ═══════════════════════════════════════════════════════════════════════════
story.append(section_header("1. HAASE'S RULE — Crown-to-Heel Length Estimation"))
story.append(Spacer(1, 2*mm))
story.append(Paragraph(
"For the first 5 months: <b>Length (cm) = Month²</b> | "
"For months 5–10: <b>Length (cm) = Month × 5</b>",
BODY_STYLE))
story.append(Spacer(1,1*mm))
haase_headers = ["Month", "Length (cm)", "Weight (approx)", "Key Feature"]
haase_rows = [
["1", "1", "—", "Embryo; heart begins to beat"],
["2", "4", "—", "Limb buds; all organs forming"],
["3", "9", "~45 g", "Ossification begins; sex determinable"],
["4", "16", "~110 g", "Quickening felt; scalp hair"],
["5 ★", "25", "~340 g", "Vernix caseosa; lanugo; eyebrows"],
["6", "30", "~600 g", "Eyelids fused; limit of viability"],
["7 ★", "35", "~1200 g", "Eyes open; Béclard's centre (lower femur)"],
["8", "40", "~1800 g", "Testes begin descent (male)"],
["9 ★", "45", "~2400 g", "Poland's centre (upper tibia); nails reach tips"],
["10 (Term)", "50", "~3200 g", "Ear cartilage firm; sole creases; term"],
]
haase_widths = [18*mm, 28*mm, 36*mm, 104*mm]
story.append(make_table(haase_headers, haase_rows, haase_widths))
story.append(Paragraph("★ = critical medicolegal age points", NOTE_STYLE))
story.append(Spacer(1, 3*mm))
# ═══════════════════════════════════════════════════════════════════════════
# SECTION 2 – OSSIFICATION CENTRES TABLE
# ═══════════════════════════════════════════════════════════════════════════
story.append(section_header("2. OSSIFICATION CENTRES — Medicolegal Significance", bg=CRIMSON))
story.append(Spacer(1, 2*mm))
osc_headers = ["Centre", "Location", "Age Appears", "Size at Term", "Medicolegal Significance"]
osc_rows = [
[
("BÉCLARD'S POINT ★★★", TABLE_CELL_RED),
"Lower femoral epiphysis",
"36 weeks (9th month)",
"5–6 mm",
"Proves ≥36 weeks gestation; legal viability established; survives putrefaction"
],
[
("POLAND'S POINT ★★", TABLE_CELL_RED),
"Upper tibial epiphysis",
"38–40 weeks (10th month)",
"3–4 mm",
"Confirms near-term / full-term; used with Béclard's for corroboration"
],
["Calcaneus", "Heel bone", "5th–6th foetal month", "Present at birth", "Confirms >24 weeks; seen on X-ray in foetal remains"],
["Talus", "Ankle bone", "7th–8th foetal month", "Present at birth", "Part of maturity assessment"],
["Cuboid", "Lateral mid-foot", "Near term (38–40 wks)", "Small at birth", "Confirms term birth"],
["Head of humerus", "Proximal humerus", "1st postnatal year (3–6 mo)", "—", "Postnatal age estimation"],
["Capitulum of humerus", "Lateral condyle", "1–2 years postnatal", "—", "Child age estimation in abuse cases"],
["Femoral head", "Proximal femur", "4–6 months postnatal", "—", "Postnatal age / neglect / AVN"],
["Iliac crest", "Pelvis", "Adolescence (~15 yrs)", "—", "Age estimation 15–23 yrs"],
["Medial clavicle epiphysis", "Sternoclavicular joint", "18–20 years", "Fused by 25–30 yrs", "Age 18–30 estimation; most reliable adult marker"],
]
osc_widths = [38*mm, 32*mm, 28*mm, 20*mm, 68*mm]
story.append(make_table(osc_headers, osc_rows, osc_widths))
story.append(Paragraph(
"★★★ BÉCLARD'S POINT is the single most important ossification centre in forensic practice.",
MNEMONIC_STYLE))
story.append(Spacer(1, 2*mm))
# ═══════════════════════════════════════════════════════════════════════════
# SECTION 3 – EXTERNAL MATURITY SIGNS
# ═══════════════════════════════════════════════════════════════════════════
story.append(section_header("3. EXTERNAL SIGNS OF FOETAL MATURITY"))
story.append(Spacer(1, 2*mm))
ext_headers = ["Feature", "Preterm (<36 wks)", "Term (≥38 wks)", "Medicolegal Note"]
ext_rows = [
["Ear cartilage", "Soft, folds easily, stays folded", "Firm, springs back instantly", "Key maturity marker at autopsy"],
["Sole creases", "Absent or only anterior creases", "Deep creases covering entire sole", "Score-based maturity grading"],
["Lanugo hair", "Abundant over body", "Only on shoulders/back", "Shed by 36–38 weeks"],
["Vernix caseosa", "Thick coating", "Minimal or absent", "Protective, shed near term"],
["Nails", "Soft, do not reach fingertips", "Reach or exceed fingertips", "Maturity + overdue if beyond tips"],
["Breast nodule", "<5 mm or absent", "≥7 mm diameter", "Ballard/New Ballard score"],
["Genitalia (M)", "Testes undescended; empty scrotum", "Testes in scrotum; rugae present", "Testes descend ~36 wks"],
["Genitalia (F)", "Labia minora prominent", "Labia majora cover minora completely", "Fat deposition in majora at term"],
["Skin", "Thin, gelatinous, transparent", "Thick, opaque, peeling", "Premature = thin, veins visible"],
["Eyelids", "Fused shut <26 wks", "Open by 26–28 wks", "Fused = severe prematurity"],
]
ext_widths = [28*mm, 42*mm, 42*mm, 74*mm]
story.append(make_table(ext_headers, ext_rows, ext_widths))
story.append(Spacer(1, 3*mm))
story.append(PageBreak())
# ═══════════════════════════════════════════════════════════════════════════
# SECTION 4 – MEDICOLEGAL DEFINITIONS
# ═══════════════════════════════════════════════════════════════════════════
story.append(section_header("4. ESSENTIAL MEDICOLEGAL DEFINITIONS"))
story.append(Spacer(1, 2*mm))
definitions = [
("VIABILITY",
"Capacity of a foetus to survive independently after delivery. "
"India (MTP Act): 20 weeks (24 wks for special categories under 2021 Amendment). "
"UK: 24 weeks. WHO: 22–24 weeks. Legal (India courts): 28 weeks / ≥1000 g."),
("LIVE BIRTH (WHO)",
"Complete expulsion/extraction from mother of a product of conception that, AFTER separation, "
"breathes OR shows any other evidence of life (heartbeat, pulsation of cord, voluntary muscle movement), "
"regardless of gestational age."),
("STILLBIRTH",
"Birth after 28 completed weeks of gestation of a baby that shows NO sign of life (no breathing, "
"no heartbeat, no voluntary movement). Must be registered. No birth certificate issued (India). "
"Macerated stillbirth = intrauterine death; Fresh stillbirth = intrapartum death."),
("INFANTICIDE",
"Unlawful killing of a newborn infant by wilful act or omission. Under Infanticide Act (UK): "
"mother who kills her child within 12 months of birth while balance of mind disturbed by effects "
"of birth/lactation is guilty of infanticide (not murder). India: Sections 302/304 IPC apply."),
("CONCEALMENT OF BIRTH",
"Disposal of the body of a child after birth to conceal the fact of its birth, whether the child "
"was born alive or dead. India: Section 318 IPC (now Section 319 BNS 2023). Punishable by up to "
"2 years imprisonment ± fine. No need to prove child was born alive."),
("FOETICIDE",
"Willful destruction of a foetus in the uterus. Includes criminal abortion. "
"India: Punishable under Section 312 IPC (illegal abortion) with up to 7 years imprisonment."),
("ABORTION",
"Expulsion of products of conception before viability (before 20–28 weeks depending on jurisdiction). "
"Spontaneous = miscarriage. Induced = may be legal (MTP Act) or illegal (criminal). "
"MTP Act 1971 (amended 2021): Legal abortion up to 20 weeks (routine), up to 24 weeks (special categories)."),
("LEGITIMACY",
"A child is legitimate if born within a valid marriage or within 280 days after dissolution of marriage "
"(presumption). Minimum gestation 210 days (7 months). Maximum accepted by courts: 280–300 days (some "
"courts accepted up to 349 days). DNA testing now definitive."),
("GESTATIONAL AGE",
"Duration of pregnancy calculated from the FIRST DAY of the last menstrual period (LMP). "
"Normal = 280 days (40 weeks) from LMP or 266 days from ovulation/fertilisation. "
"Established by: USG, fundal height, foetal parameters, ossification centres at autopsy."),
("HYDROSTATIC TEST (Docimasia Pulmonum)",
"Medicolegal test for live birth. Principle: foetal lungs are atelectatic (density >1, SINK). "
"After breathing, air expands alveoli (density <1, FLOAT). "
"Positive (floats) = baby breathed after birth. "
"Limitations: putrefaction causes false +ve; CPR/resuscitation causes false +ve; forcible compression causes false -ve."),
("BIRTH ASPHYXIA",
"Failure to establish adequate respiration at birth due to insufficient oxygen (hypoxia) and/or "
"accumulation of CO2 (hypercapnia) and lactic acid. Causes: cord prolapse, placental abruption, "
"obstructed labour, meconium aspiration. Leads to HIE. Medicolegal: major cause of medical negligence claims."),
("MACERATION",
"Post-mortem autolysis of a stillborn foetus retained in utero after intrauterine death. "
"Features: skin slippage, discolouration (reddish-brown), softening of tissues, overlapping skull bones. "
"Takes 12–24 hours to begin; full maceration in 3–5 days. Confirms intrauterine death."),
("MUMMIFICATION (FOETAL)",
"Drying and shrinkage of a foetus retained in utero for prolonged period. "
"Seen in lithopedion (calcified ectopic foetus, years to decades). "
"Forensic importance: establishes retained dead foetus vs. recent delivery."),
("CAPUT SUCCEDANEUM",
"Diffuse oedematous swelling of the scalp crossing suture lines, formed during labour due to "
"pressure of the presenting part. Present at birth, resolves in 1–2 days. "
"Distinguish from cephalhaematoma (subperiosteal, does NOT cross sutures, blood takes weeks to resolve)."),
("BIRTH INJURY",
"Physical injury sustained by neonate during labour and delivery. Includes: cephalhaematoma, "
"intracranial haemorrhage, clavicular fracture (most common), brachial plexus injury (Erb's palsy), "
"facial nerve palsy. Medicolegal: relevant in obstetric negligence claims."),
("TARDIEU'S SPOTS",
"Petechial haemorrhages on visceral pleura, epicardium, and thymic surface due to increased venous "
"pressure during asphyxia. Classic sign of asphyxial death. Also seen in birth asphyxia. "
"Must be distinguished from post-mortem hypostasis."),
("UMBILICAL CORD — FORENSIC",
"Normal cord: 50–55 cm long, 2 arteries + 1 vein (AVA). "
"Single umbilical artery: associated with renal agenesis, trisomy 18. "
"True knot: may cause foetal death. "
"Cord around neck (nuchal cord): present in 20–30% deliveries, usually harmless. "
"Fresh cut/torn cord with live birth features: infanticide suspected."),
("MTP ACT 1971 (AMENDED 2021)",
"Medical Termination of Pregnancy Act (India). "
"Up to 20 weeks: one registered medical practitioner's opinion. "
"20–24 weeks: two practitioners required; only for special categories (rape, incest, foetal abnormality, disability). "
"Beyond 24 weeks: only for substantial foetal abnormality — requires Medical Board approval. "
"Violation: criminal abortion (Section 312–316 IPC)."),
]
def_widths = [42*mm, 144*mm]
def_data = [[Paragraph("TERM", TABLE_HDR), Paragraph("DEFINITION", TABLE_HDR)]]
for i, (term, defn) in enumerate(definitions):
bg = LTGOLD if i % 2 == 0 else WHITE
def_data.append([
Paragraph(term, TABLE_CELL_BOLD),
Paragraph(defn, TABLE_CELL)
])
def_table = Table(def_data, colWidths=def_widths, repeatRows=1)
def_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), NAVY),
("GRID", (0,0), (-1,-1), 0.3, colors.HexColor("#CCCCCC")),
("ROWPADDING", (0,0), (-1,-1), 4),
("VALIGN", (0,0), (-1,-1), "TOP"),
*[("BACKGROUND", (0, i+1), (-1, i+1), LTGOLD if i % 2 == 0 else WHITE)
for i in range(len(definitions))]
]))
story.append(def_table)
story.append(Spacer(1, 4*mm))
# ═══════════════════════════════════════════════════════════════════════════
# SECTION 5 – KEY MNEMONICS
# ═══════════════════════════════════════════════════════════════════════════
story.append(section_header("5. MNEMONICS & QUICK RECALL", bg=TEAL))
story.append(Spacer(1, 2*mm))
mnem_headers = ["Mnemonic", "What it covers"]
mnem_rows = [
['"Béclard Proves Birth" (BPB)', "Béclard = Proves ≥8 months; Poland = near-Birth (10th month)"],
['"AVA in the cord"', "2 Arteries, 1 Vein, Arteries (single umbilical artery = renal agenesis risk)"],
['"FAVE" shunts', "Foramen ovale, Arteriosus ductus, Venosus ductus = three foetal bypasses"],
['"DV → LV → RA → FO → LA" for oxygenated blood', "Ductus Venosus → IVC → Right Atrium → Foramen Ovale → Left Atrium → Systemic"],
['Haase rule: "Square then Times 5"', "Months 1–5: month², Months 5–10: month × 5 (crown-heel in cm)"],
['"SWIM test" (Hydrostatic test)', "Lungs Swim = baby breathed (live birth); Lungs Sink = stillborn/did not breathe"],
['"Ear springs back at 36"', "Firm ear cartilage that springs back = ≥36 weeks gestation"],
['"210 to 300" gestation window', "Min viability 210 days; normal 280 days; max accepted ~300 days (legitimacy)"],
['"MTP 20-24 Rule"', "Routine abortion ≤20 wks; special categories up to 24 wks (MTP Amendment 2021)"],
['"CAPS" for external maturity', "Creases (sole), Areola, Posture/lanugo, Skin texture = Ballard score components"],
]
mnem_widths = [58*mm, 128*mm]
story.append(make_table(mnem_headers, mnem_rows, mnem_widths))
story.append(Spacer(1, 3*mm))
# ═══════════════════════════════════════════════════════════════════════════
# SECTION 6 – ADULT AGE ESTIMATION FROM BONE
# ═══════════════════════════════════════════════════════════════════════════
story.append(section_header("6. ADULT AGE ESTIMATION — KEY SKELETAL MARKERS", bg=colors.HexColor("#4A148C")))
story.append(Spacer(1, 2*mm))
adult_headers = ["Age Range", "Skeletal Marker", "Description"]
adult_rows = [
["15–17 yrs", "Iliac crest epiphysis appears", "Ring apophysis begins ossification"],
["18–20 yrs", "Medial clavicle epiphysis appears", "Most reliable marker for 18+ yrs"],
["20–23 yrs", "Vertebral ring apophysis fuses", "Last vertebral fusion"],
["25–30 yrs", "Medial clavicle fuses completely", "Fusion = >25 yrs; most reliable upper limit"],
["25–35 yrs", "Skull sutures begin closing", "Coronal and sagittal first; unreliable alone"],
["30–45 yrs", "Pubic symphysis changes", "Todd / Suchey-Brooks phases 1–6"],
["35–50 yrs", "Sternal end 4th rib changes", "İşcan method for rib metamorphosis"],
[">40 yrs", "Osteoarthritis changes appear", "Lipping, eburnation, narrowing joint spaces"],
[">50 yrs", "Osteoporosis, trabecular loss", "Cortical thinning; DEXA relevant"],
["Any age", "Dental eruption & wear", "Third molar: >17 yrs; wear pattern for 30+ yrs"],
]
adult_widths = [22*mm, 58*mm, 106*mm]
story.append(make_table(adult_headers, adult_rows, adult_widths))
story.append(Spacer(1, 3*mm))
# ═══════════════════════════════════════════════════════════════════════════
# SECTION 7 – FOETAL CIRCULATION QUICK REF
# ═══════════════════════════════════════════════════════════════════════════
story.append(section_header("7. FOETAL CIRCULATION — SHUNTS & CLOSURE TIMELINE", bg=CRIMSON))
story.append(Spacer(1, 2*mm))
shunt_headers = ["Shunt", "Connects", "Function", "Functional Closure", "Adult Remnant"]
shunt_rows = [
["Ductus venosus", "Umbilical vein → IVC", "Bypasses liver; delivers O₂-rich blood to heart", "Within hours of birth (sphincter)", "Ligamentum venosum"],
["Foramen ovale", "Right atrium → Left atrium", "Bypasses lungs; shunts O₂-rich IVC blood to systemic", "At first breath (L>R atrial pressure)", "Fossa ovalis"],
["Ductus arteriosus", "Pulmonary trunk → Descending aorta", "Bypasses lungs; right ventricular output to aorta", "20% by 24h; 80% by 48h; 100% by 96h", "Ligamentum arteriosum"],
["Umbilical vein", "Placenta → foetal liver/IVC", "Carries oxygenated blood from placenta", "Within minutes of birth", "Ligamentum teres hepatis"],
["Umbilical arteries (×2)", "Foetal iliac arteries → placenta", "Return deoxygenated blood to placenta", "Immediately on cord clamping", "Medial umbilical ligaments"],
]
shunt_widths = [28*mm, 36*mm, 46*mm, 36*mm, 40*mm]
story.append(make_table(shunt_headers, shunt_rows, shunt_widths))
story.append(Spacer(1, 3*mm))
# ═══════════════════════════════════════════════════════════════════════════
# SECTION 8 – IMPORTANT LEGAL PROVISIONS
# ═══════════════════════════════════════════════════════════════════════════
story.append(section_header("8. KEY LEGAL PROVISIONS — INDIA", bg=colors.HexColor("#1B5E20")))
story.append(Spacer(1, 2*mm))
legal_headers = ["Section", "Act", "Offence / Subject", "Punishment"]
legal_rows = [
["312 IPC / 88 BNS", "IPC 1860 / BNS 2023", "Causing miscarriage (criminal abortion)", "Up to 3 yrs; up to 7 yrs if woman objects"],
["313 IPC / 89 BNS", "IPC 1860 / BNS 2023", "Causing miscarriage without woman's consent", "Life imprisonment or 10 yrs + fine"],
["314 IPC / 90 BNS", "IPC 1860 / BNS 2023", "Death caused by abortion attempt", "Up to 10 yrs + fine; life if without consent"],
["315 IPC / 91 BNS", "IPC 1860 / BNS 2023", "Act to prevent child being born alive / causing post-birth death", "Up to 10 yrs + fine"],
["316 IPC / 92 BNS", "IPC 1860 / BNS 2023", "Causing death of quick unborn child (culpable homicide)", "Up to 10 yrs + fine"],
["318 IPC / 94 BNS", "IPC 1860 / BNS 2023", "Concealment of birth by disposal of body", "Up to 2 yrs + fine"],
["302 IPC / 101 BNS", "IPC 1860 / BNS 2023", "Infanticide (murder)", "Death or life imprisonment"],
["MTP Act 1971 (Amended 2021)", "Central Act", "Legal termination of pregnancy", "Legal: ≤20 wks; ≤24 wks (special); >24 wks Board only"],
["PCPNDT Act 1994", "Central Act", "Prohibition of sex determination of foetus", "Up to 3 yrs + fine; 5 yrs repeat offence"],
["Registration of Births & Deaths Act 1969", "Central Act", "Registration of stillbirths and live births", "Mandatory; stillbirth ≥28 wks must be registered"],
]
legal_widths = [32*mm, 30*mm, 72*mm, 52*mm]
story.append(make_table(legal_headers, legal_rows, legal_widths))
story.append(Spacer(1, 3*mm))
# ── Footer note ──────────────────────────────────────────────────────────────
hr()
story.append(hr())
story.append(Paragraph(
"References: Moore – The Developing Human (Clinically Oriented Embryology) | "
"Parikh's Textbook of Medical Jurisprudence, Forensic Medicine & Toxicology | "
"Reddy's Essentials of Forensic Medicine & Toxicology | MTP Act 1971 (Amended 2021) | IPC / BNS 2023",
NOTE_STYLE))
story.append(Paragraph(
"Prepared as exam quick reference only. Always verify against current legislation and standard references.",
NOTE_STYLE))
# ── Build ─────────────────────────────────────────────────────────────────────
doc.build(story)
print(f"PDF generated: {OUTPUT}")
cd /home/daytona/workspace/forensic-cheatsheet && python3 make_cheatsheet.py 2>&1
ls -lh /home/daytona/workspace/forensic-cheatsheet/Forensic_Ossification_Cheatsheet.pdf
Forensic Ossification Cheatsheet
PDF Document · PDF
- Haase's Rule table - all 10 months with length, weight, and key developmental milestone for each
- Ossification Centres table - Béclard's point (★★★), Poland's point (★★), calcaneus, talus, cuboid, head of humerus, medial clavicle, iliac crest - each with age, size, and medicolegal significance
- External Maturity Signs table - preterm vs. term comparison for ear cartilage, sole creases, lanugo, vernix, nails, breast nodule, genitalia, skin, eyelids
- 18 Medicolegal Definitions - viability, live birth (WHO), stillbirth, infanticide, concealment of birth, foeticide, abortion, legitimacy, gestational age, hydrostatic test, birth asphyxia, maceration, mummification, caput succedaneum, birth injury, Tardieu's spots, umbilical cord forensics, MTP Act 2021
- 10 Mnemonics - including "Béclard Proves Birth", "AVA in the cord", "SWIM test", "FAVE shunts", Haase's rule shortcut
- Adult age estimation skeletal markers - 15 yrs through >50 yrs
- Foetal circulation shunts and closure timeline - all 5 structures with adult remnants
- Key Indian legal provisions - IPC/BNS sections 312-318, MTP Act, PCPNDT Act, with punishments