In detail about femoroacetabular impingement for Orthopaedic postgraduate exam don't miss any points
Reading File
Finding Sources
Searching the Web
femoroacetabular impingement FAI orthopaedic exam complete notes classification diagnosis treatment
Searching PubMed
"femoroacetabular impingement"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile the definitive answer:
Femoroacetabular Impingement (FAI) - Complete Orthopaedic PG Notes
1. DEFINITION
Femoroacetabular impingement (FAI) is a condition where abnormal contact between the proximal femur and the acetabulum - caused by morphological variation of either or both structures - results in impingement of the hip joint during functional range of motion. This leads to labral, chondral, and soft-tissue damage, and predisposes the hip to early osteoarthritis.
- First described and popularized by Ganz et al.
- Consensus on FAIS (FAI Syndrome) established in 2016 (Warwick Agreement)
- FAIS is a triad: symptoms + clinical signs + bony deformity (all three required)
2. CLASSIFICATION / TYPES
Three types exist; combined type is the most common in clinical practice.
A. CAM Impingement (Femoral-sided)
- Abnormal bony prominence at the anterosuperior femoral head-neck junction (reduced offset / non-spherical head)
- During flexion + internal rotation, the non-spherical portion rotates into the acetabulum
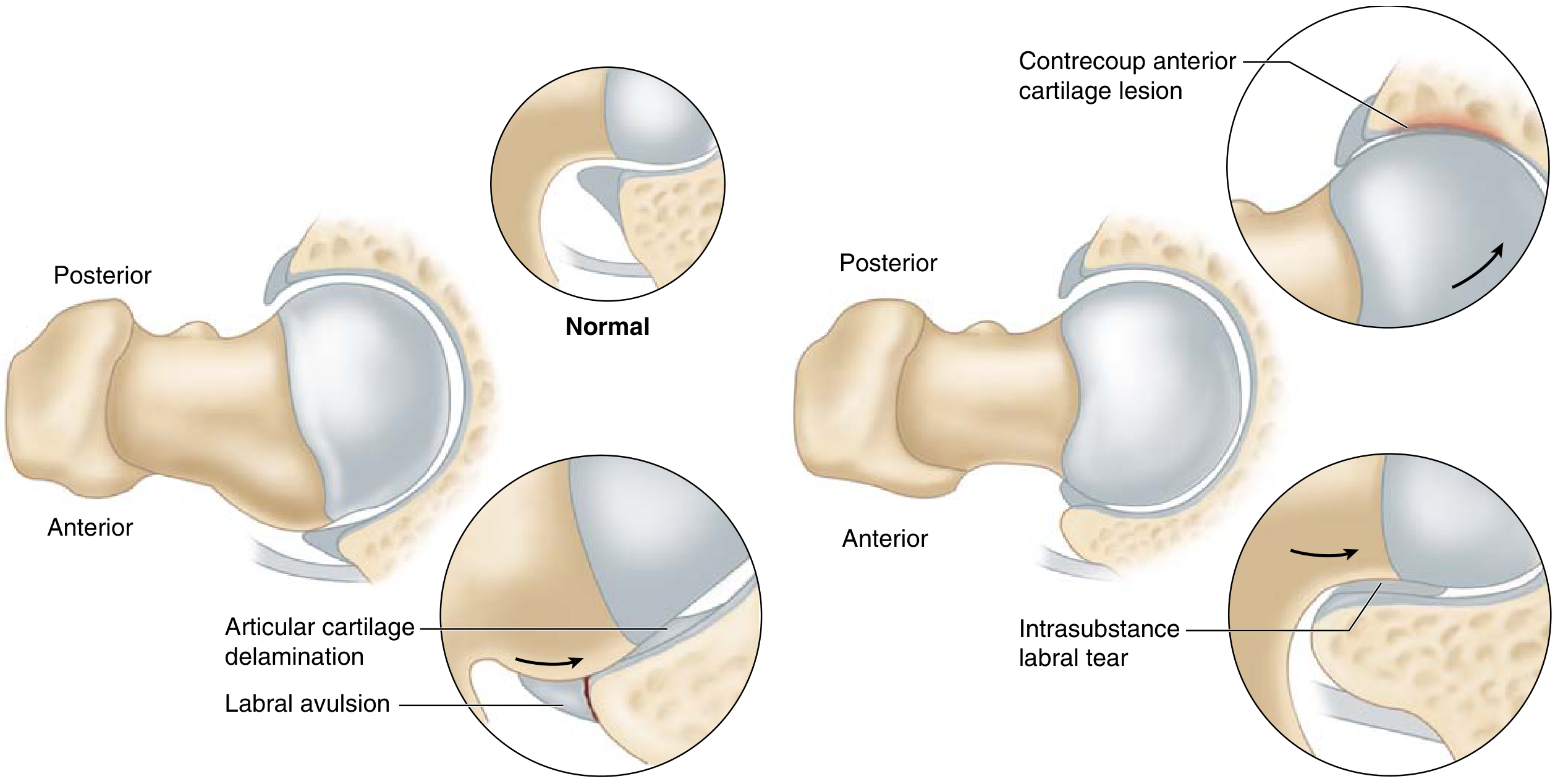
- Results in labral avulsion at the labro-chondral junction and articular cartilage delamination (carpet lesion) progressing from the acetabular rim inward
- The labrum is relatively spared in cam impingement; cartilage damage predominates
- More common in young athletic males
- Etiology: possibly a developmental abnormality of the lateral femoral physis related to high-intensity sports during adolescence
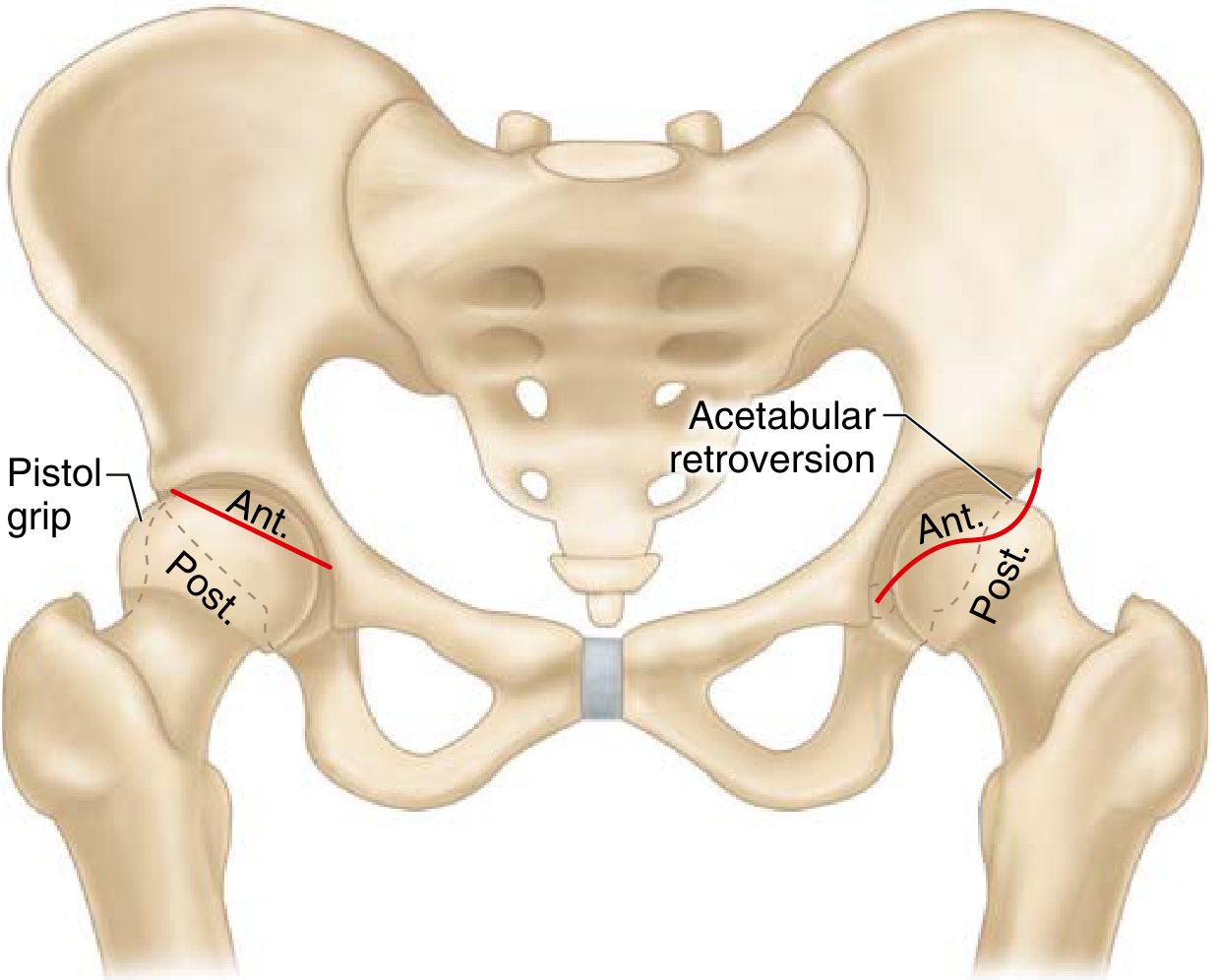
- Pistol-grip deformity = non-spherical femoral head on AP radiograph
B. PINCER Impingement (Acetabular-sided)
- Overcoverage of the femoral head by the acetabulum causes the femoral neck to abut the acetabular rim during motion
- Causes:
- Acetabular retroversion (crossover sign)
- Coxa profunda (acetabular fossa medial to ilioischial line)
- Protrusio acetabuli (femoral head crosses ilioischial line)
- Global overcoverage / deep acetabulum
- Results in intrasubstance labral tears (typically anterosuperior quadrant); labrum is primarily injured
- Contrecoup injury = posteroinferior acetabular cartilage damage from levering of femoral neck on rim
- More common in middle-aged women
- Worsens with time due to reactive bone growth / labral calcification increasing overcoverage
C. Combined CAM + PINCER (Most Common)
- Both morphologies coexist
- Damages both acetabular rim cartilage and labrum to varying degrees
- Worst clinical prognosis of all three types
D. Femoral Retrotorsion
- Contributes to anterior hip impingement as an additional mechanism
3. EPIDEMIOLOGY & RISK FACTORS
- Young to middle-aged adults (teens to 50s)
- Male sex (cam type); Female sex (pincer type)
- Athletes in high-intensity sports: hockey, soccer, football, tennis, ballet, cycling
- Caucasian ethnicity
- Familial FAI morphology
- High-impact activities during adolescent skeletal development
- Cam morphology prevalence in elite athletes approaches 60-70%
4. PATHOANATOMY
The anterosuperior labrum and cartilage are the primary sites of injury.
| Type | Primary lesion | Secondary lesion |
|---|---|---|
| Cam | Cartilage delamination (acetabular rim → central) | Labral avulsion |
| Pincer | Labral intrasubstance tear (anterosuperior) | Contrecoup posterior cartilage lesion |
| Combined | Both cartilage + labrum | Worse outcomes |
- Labral tear site: anterosuperior quadrant is most frequently affected in both types
- Carpet lesion: acetabular cartilage delamination from subchondral bone - specific to cam FAI
- FAI is a leading cause of secondary hip osteoarthritis in young adults
5. CLINICAL FEATURES
Symptoms
- Groin pain - the most common presentation; typically slow onset, persistent
- Pain worsens with: deep hip flexion, prolonged sitting, twisting, sporting activity
- C-sign: Patient cups the hand over the lateral hip in a "C" shape to describe pain location
- Hip stiffness and limited range of motion
Clinical Signs
- Limited internal rotation in flexion (most consistent finding)
- Patients have more passive external rotation than internal rotation
- Positive anterior impingement test (FADIR test): Flexion + ADduction + Internal Rotation reproduces groin pain
- Most sensitive test for FAI (~95% sensitive but low specificity)
- FABER test (Flexion + ABduction + External Rotation): assesses posterior impingement and labral tears; pain = positive
- Posterior impingement test: Extension + external rotation reproduces posterior hip pain
- Log roll test: patient supine, passive internal/external rotation - pain suggests intraarticular pathology
- Stinchfield test: resisted hip flexion at 30° reproduces pain
6. IMAGING
A. Plain Radiographs
Views required:
- AP pelvis (gold standard initial view)
- 45° Dunn lateral view (preferred by most hip arthroscopists - best for measuring alpha angle; identifies subtle cam deformities not visible on AP)
- Cross-table lateral
- False-profile view: evaluates anterior coverage, subspine deformities, posterior joint space narrowing
Radiographic indicators for FAI:
| Sign | Type | Description |
|---|---|---|
| Alpha angle >55° | Cam | Angle measuring loss of femoral head sphericity on Dunn/lateral view |
| Pistol-grip deformity | Cam | Non-spherical femoral head on AP view |
| Head-neck offset ratio reduced | Cam | <0.17 indicates loss of offset |
| Crossover sign | Pincer | Anterior acetabular wall line crosses lateral to posterior wall = acetabular retroversion |
| Figure-of-8 sign | Pincer | Exaggerated crossover |
| Coxa profunda | Pincer | Acetabular fossa medial to ilioischial line (may be normal variant in women) |
| Protrusio acetabuli | Pincer | Femoral head crosses the ilioischial line |
| Lateral centre-edge angle >40° | Pincer | Overcoverage (normal: 25-40°) |
| Sclerosis/cysts at anterolateral head-neck junction | Both | Present in ~1/3 of symptomatic patients |
| Calcified labrum | Pincer | Worsens overcoverage |
Caveat: >90% of asymptomatic adolescents have at least one radiographic parameter suggesting FAI; 50% have two - correlation with symptoms is essential.
B. CT Scan / 3D-CT
- Best for assessing bony morphology and version of femur and acetabulum
- 3D reconstruction guides surgical planning for amount of bony resection
- Delineates extent of cam and pincer deformity
- Measures femoral version and acetabular version accurately
C. MRI / MR Arthrography (MRA)
- MRA (intraarticular gadolinium) is the gold standard for labral pathology
- Sensitivity increases from ~60% (plain MRI) to >90% with contrast
- Reveals labral tears, cartilage delamination, paralabral cysts
- Axial oblique sequence: alpha angle measured on MRI (see diagram below)
- Contrast tracking beneath articular cartilage suggests delamination
- Higher-resolution 3T MRI may eventually replace MRA
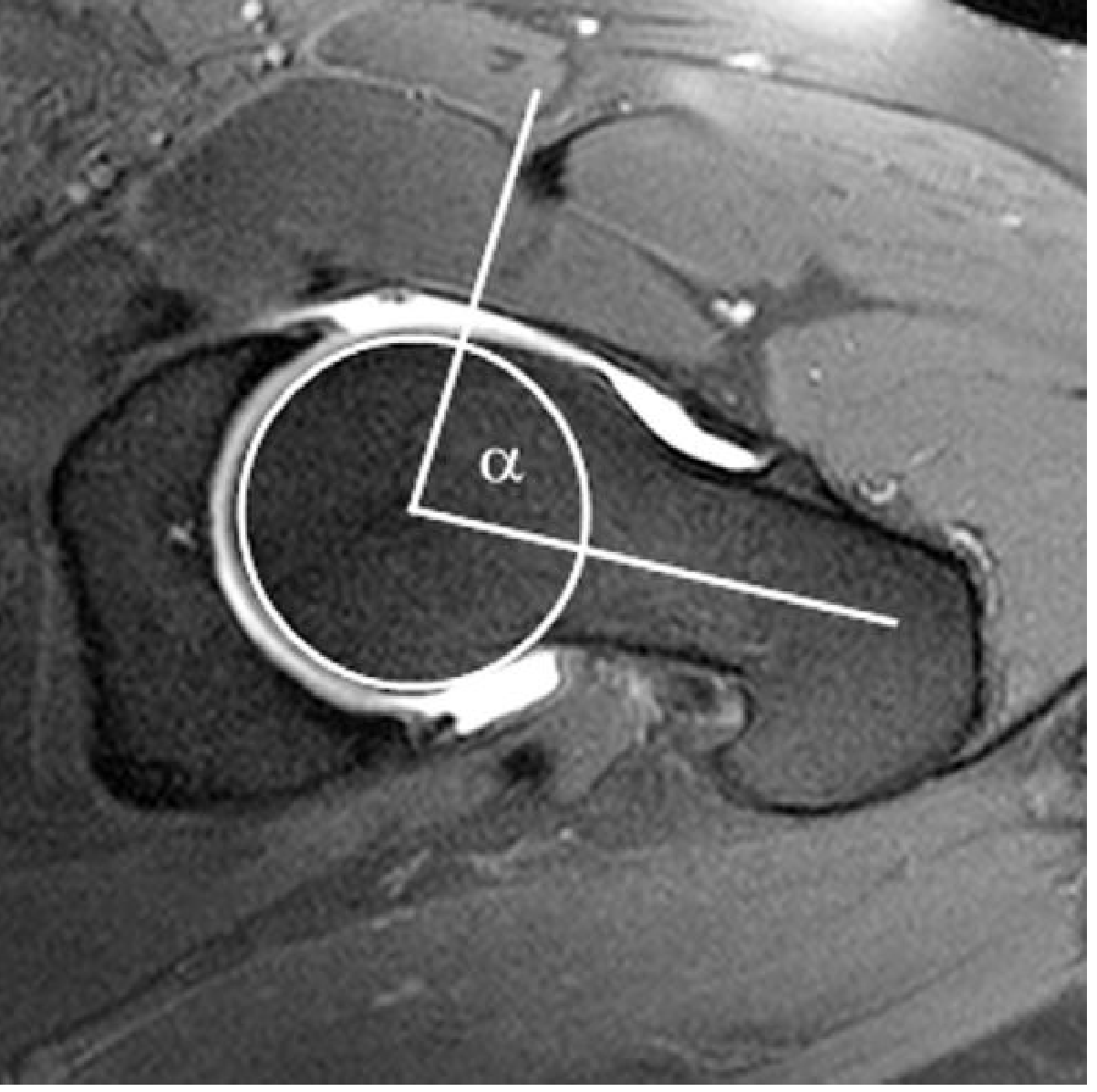
Alpha angle: Line along femoral neck axis vs line from femoral head center to the point where the head protrudes beyond the best-fit circle. >55° is abnormal (some sources use >50°).
D. Intraarticular Injection
- Diagnostic/therapeutic: Fluoroscopy-guided intraarticular LA ± steroid
- If injection relieves pain, confirms intraarticular source of pain
7. KEY MEASUREMENTS (Exam High-Yield)
| Measurement | Normal | Abnormal (FAI) |
|---|---|---|
| Alpha angle | <50-55° | >55° = cam |
| Lateral centre-edge angle (LCEA) | 25-40° | >40° = pincer overcoverage |
| Anterior centre-edge angle (ACEA) | >25° | - |
| Tönnis angle (acetabular index) | <10° | >10° = dysplasia (low coverage) |
| Head-neck offset ratio | >0.17 | <0.17 = cam |
| Joint space | >2 mm | <2 mm = high THA conversion risk |
8. CLASSIFICATION OF ARTICULAR CARTILAGE DAMAGE
Tönnis Classification of Osteoarthritis (important for prognosis):
- Grade 0: No signs of OA
- Grade 1: Slight narrowing, sclerosis
- Grade 2: Small cysts, moderate narrowing, loss of sphericity
- Grade 3: Large cysts, severe narrowing, avascular necrosis signs
Tönnis grade 2 or higher = poor outcomes after hip arthroscopy
Outerbridge / Beck Classification used intraoperatively for chondral damage.
9. DIFFERENTIAL DIAGNOSIS
- Hip dysplasia (DDH) - LCEA <20°, acetabular index >10°
- Labral tear without FAI
- Avascular necrosis (AVN) of femoral head
- Iliopsoas tendinitis / internal snapping hip
- Trochanteric bursitis
- Hip OA
- Stress fracture of femoral neck
- Lumbar spine pathology
- Sports hernia / athletic pubalgia
- Piriformis syndrome
10. TREATMENT
A. Conservative (Non-Operative) - First Line
- Activity modification: avoid deep flexion, high-impact sports
- Physiotherapy: core strengthening, hip rotator strengthening, ROM exercises
- NSAIDs / analgesics
- Intraarticular corticosteroid injection (diagnostic + therapeutic)
- Conservative management for 3-6 months before surgery
B. Operative Treatment
Indications for surgery:
- Failed conservative treatment (3-6 months)
- Symptomatic FAI with confirmed labral/chondral pathology on MRI
- Good/adequate joint space (Tönnis grade 0-1; joint space >2 mm)
- No severe osteoarthritis
Contraindications:
- Tönnis grade 2+ OA (relative contraindication)
- Joint space <2 mm (predicts high THA conversion rate)
- Advanced age with significant OA → proceed to THA
B1. Hip Arthroscopy (Most Common Surgical Approach)
- Preferred method for most FAI cases
- Performed through 2-3 portals (anterolateral, anterior, mid-anterior)
- Traction applied to distract the joint
- Procedures performed:
- Cam resection (femoral osteochondroplasty): reshaping the femoral head-neck junction
- Pincer resection (rim trimming / acetabuloplasty): removing excess acetabular rim
- Labral repair: preferred over debridement (superior outcomes); labral refixation using suture anchors
- Labral reconstruction: if labrum is irreparable (using IT band or ligamentum teres graft)
- Chondral treatment: microfracture, fibrin glue, cartilage repair as needed
- Capsular plication or repair (especially in borderline dysplasia)
- Return to sport: median 6 months
- Outcomes: Excellent in properly selected patients; 80-90% patient satisfaction
B2. Surgical Hip Dislocation (Ganz Trochanteric Flip Osteotomy)
- Allows excellent 360° exposure of the femoral head and acetabulum
- Indicated for: severe deformities not amenable to arthroscopy, complex combined pathology
- Technique (Ganz):
- Trochanteric flip osteotomy
- Z-shaped capsulotomy (anterior Z-capsulotomy)
- Safe surgical dislocation preserving posterior blood supply (medial femoral circumflex artery)
- Preserves femoral head blood supply - very important
- Allows complete labral repair and chondral flap treatment
- Complications (<5%): trochanteric nonunion, heterotopic ossification
- Anterior Z-capsulotomy preserves posterior vessels to femoral neck, minimizing AVN risk
B3. Periacetabular Osteotomy (PAO) / Bernese PAO
- For acetabular overcoverage with significant retroversion
- Posterior column is preserved - maintains pelvic stability
- Allows correction of acetabular tilt and version
- Less commonly used for FAI but helpful for retroverted acetabula
B4. Reverse PAO (Anti-protrusio / Derotation)
- Reduces anterior overcoverage in retroverted acetabulum
- Less commonly performed
B5. Femoral Osteotomy
- For femoral retrotorsion or other femoral-sided deformities
- Derotation osteotomy of the proximal femur
B6. Total Hip Arthroplasty (THA)
- Reserved for patients with significant arthritic changes (Tönnis grade 2-3)
- Joint space <2 mm = high conversion to THA risk after arthroscopy
11. PROGNOSIS / PROGNOSTIC FACTORS
Good outcomes:
- Younger age
- Tönnis grade 0-1 OA
- Joint space >2 mm
- Isolated cam impingement (better than pincer)
- Labral repair > labral debridement (superior 10-year survivorship)
- Normal acetabular coverage (LCEA 25-40°)
Poor outcomes:
- Tönnis grade ≥ 2 OA
- Joint space < 2 mm → risk of conversion to THA
- Borderline dysplasia (LCEA 18-25°) - capsular plication important
- Combined FAI morphology
- Advanced age
- Significant chondral damage at time of surgery
12. COMPLICATIONS OF HIP ARTHROSCOPY
- Traction neuropraxia (lateral femoral cutaneous nerve, pudendal nerve)
- Instrument breakage
- Avascular necrosis (rare)
- Heterotopic ossification
- Capsular instability (if over-release without repair)
- Incomplete resection → recurrence of symptoms
- Conversion to THA
13. SUBSPINE IMPINGEMENT (AIIS Impingement)
- Impingement between the anterior inferior iliac spine (AIIS) and the femoral head-neck junction
- A form of extra-articular impingement
- Common in patients with prior AIIS avulsion injuries or prominent AIIS
- Addressed arthroscopically with AIIS decompression
14. SPECIAL POINTS FOR PG EXAM
| High-Yield Fact | Detail |
|---|---|
| Alpha angle cut-off | >55° (cam); ideally measured on Dunn lateral / axial MRI |
| LCEA cut-off | >40° (pincer overcoverage); <20° = dysplasia |
| Most common type | Combined CAM + Pincer |
| Cam more common in | Young athletic males |
| Pincer more common in | Middle-aged women |
| Primary labral injury in cam | Labro-chondral junction avulsion + cartilage delamination |
| Primary labral injury in pincer | Intrasubstance labral tear (anterosuperior) |
| Contrecoup injury | Posteroinferior acetabular cartilage (in pincer) |
| Specific radiographic sign of cam | Pistol-grip deformity on AP; alpha angle on Dunn/lateral |
| Specific sign of pincer | Crossover sign (acetabular retroversion) |
| Gold standard for labral pathology | MR Arthrography (sensitivity >90%) |
| Intraoperative OA grading | Tönnis grade |
| Poor prognostic indicator | Tönnis grade ≥ 2; joint space <2 mm |
| Labral repair vs debridement | Repair = better long-term survivorship |
| Blood supply at risk in open dislocation | Medial femoral circumflex artery (protected by Z-capsulotomy) |
| Return to sport after arthroscopy | Median 6 months |
| Ganz procedure complication | Trochanteric nonunion, heterotopic ossification (<5%) |
| FAI leads to | Labral tears → early hip osteoarthritis |
| Impingement test | FADIR (Flexion, ADduction, Internal Rotation) = anterior impingement test |
15. SUMMARY OF RADIOGRAPHIC ANGLES
Alpha angle:
- Measured on: 45° Dunn lateral / cross-table lateral / axial oblique MRI
- Method: Circle of best fit around femoral head → angle between
(1) femoral neck axis and
(2) line from head center to point where head protrudes from the circle
- Normal: <50-55° | Abnormal (cam): >55°
Lateral Centre-Edge Angle (LCEA / Wiberg angle):
- Measured on: AP pelvis
- Method: Angle between vertical line from femoral head center
and line from femoral head center to lateral acetabular edge
- Normal: 25-40° | Overcoverage (pincer): >40° | Dysplasia: <20°
Head-Neck Offset Ratio:
- Normal: >0.17 | Reduced: <0.17 = cam morphology
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 | Miller's Review of Orthopaedics 9th Ed | Bailey & Love's Short Practice of Surgery 28th Ed | Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.