Shock
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
I now have comprehensive material. Let me compile the full answer.
Shock
Definition
Shock is a state of circulatory failure in which diminished cardiac output and/or reduced effective circulating blood volume impairs tissue perfusion, leading to cellular hypoxia. At the outset, cellular injury is reversible; prolonged shock leads to irreversible tissue injury and is often fatal.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 134
- Guyton and Hall Textbook of Medical Physiology
Classification
Shock falls into four major categories:
| Type | Mechanism | Key Clinical Examples |
|---|---|---|
| Cardiogenic | Pump failure - low CO due to intrinsic or extrinsic myocardial dysfunction | MI, ventricular arrhythmia, cardiac tamponade, pulmonary embolism |
| Hypovolemic | Inadequate blood/plasma volume - low CO | Hemorrhage, burns, vomiting, diarrhea |
| Distributive (Septic) | Peripheral vasodilation + cytokine cascade; maldistribution of blood flow | Gram-positive/negative bacteremia, fungal sepsis |
| Distributive (Others) | Loss of vascular tone | Neurogenic shock (spinal cord injury, anesthesia), anaphylactic shock (IgE-mediated, systemic vasodilation) |
- Robbins & Kumar Basic Pathology, Table 3.3
- Sabiston Textbook of Surgery, Fig. 33.5
Stages of Shock
Three stages are classically described (Guyton & Hall):
-
Nonprogressive (Compensated) Stage - Normal compensatory mechanisms (baroreceptors, sympathetic reflexes, RAAS) are sufficient to restore perfusion without external therapy. Arteriolar constriction, venoconstriction, and tachycardia maintain cardiac output.
-
Progressive Stage - Persistent oxygen deficit shifts aerobic to anaerobic glycolysis, producing lactic acidosis. Tissue pH falls, vasomotor response is blunted, arterioles dilate, blood pools in the microcirculation. Endothelial injury triggers DIC. Vital organs begin to fail.
-
Irreversible Stage - Widespread cell injury with lysosomal enzyme leakage. Myocardial contractility worsens (increased NO synthesis). Ischemic bowel allows translocation of intestinal flora (bacteremic superinfection). Renal failure ensues. Death follows despite maximal therapy.
Pathophysiology of Septic Shock (Most Complex)
Sepsis affects >750,000 patients/year in the US; mortality remains ~20-40%. Most frequently triggered by gram-positive bacteria, then gram-negative bacteria and fungi.
Key Mechanisms:
1. Inflammatory cascade
- Microbial PAMPs (LPS, peptidoglycans, fungal wall components) bind Toll-like receptors (TLRs), G-protein-coupled receptors, and C-type lectin receptors (dectins) on macrophages, neutrophils, and dendritic cells.
- This triggers release of TNF, IL-1, IL-6, IL-12, ROS, prostaglandins, and PAF.
- A counterinflammatory response (IL-10, soluble TNF-R, IL-1 receptor antagonist) is simultaneously activated; patients may oscillate between hyper- and hypo-inflammatory states.
2. Endothelial activation and injury
- Cytokines loosen endothelial tight junctions → vascular leakage and protein-rich edema throughout the body
- Activated endothelium upregulates nitric oxide (NO) and other vasodilators (C3a, C5a, PAF) → smooth muscle relaxation → systemic hypotension
- Microvascular heterogeneity of flow and loss of autoregulation → oxygen delivery-demand mismatch
3. Procoagulant state
- Increased tissue factor on monocytes and endothelium
- Decreased endothelial anticoagulants (TFPI, thrombomodulin, protein C)
- Increased PAI-1 suppresses fibrinolysis
- Neutrophil extracellular traps (NETs) activate both coagulation pathways
- Result: DIC in up to 50% of septic patients
4. Metabolic abnormalities
- TNF, IL-1, and stress hormones → insulin resistance and hyperglycemia
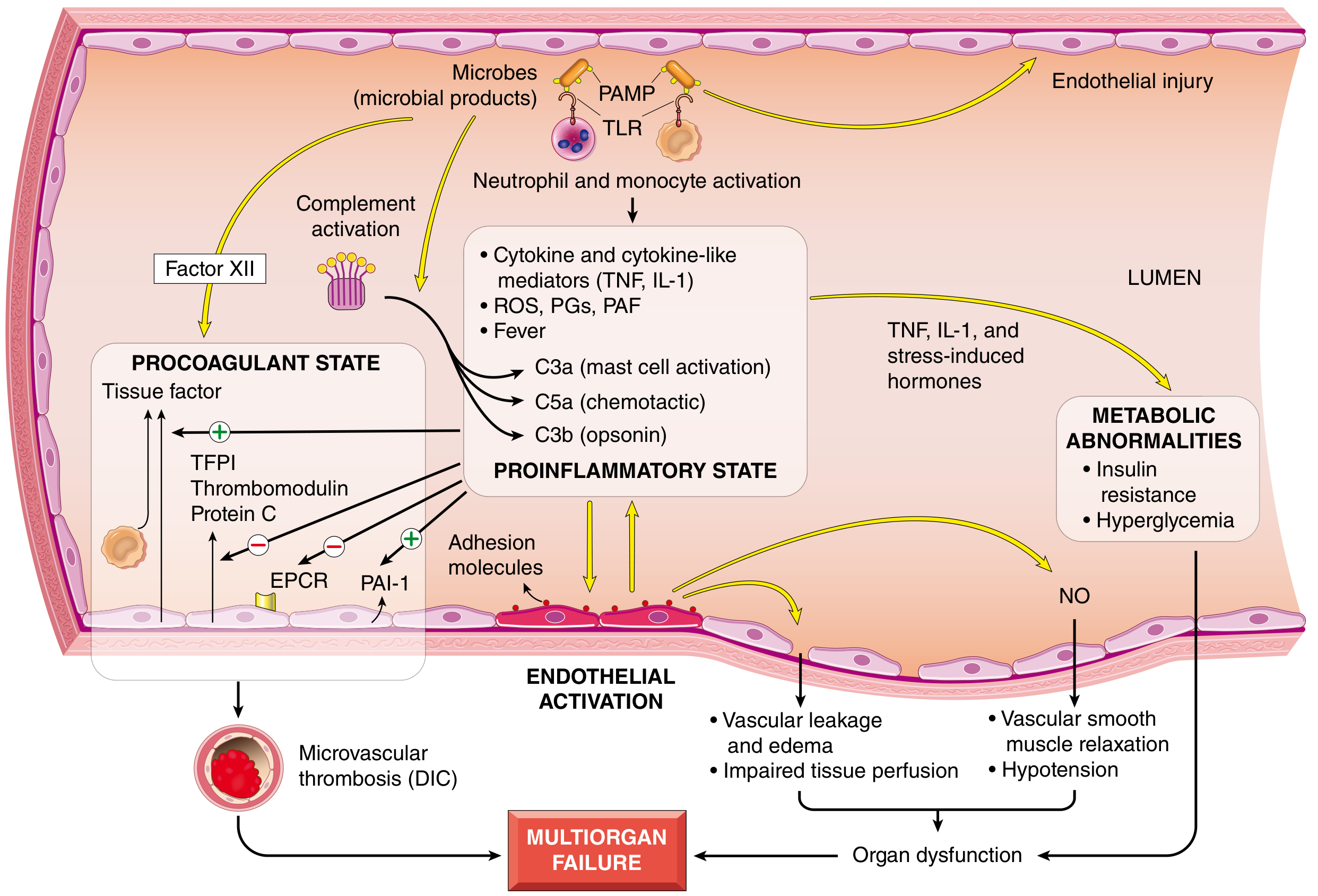
Fig: Major pathogenic pathways in septic shock. Microbial products activate innate immune cells; the resulting proinflammatory state leads to endothelial activation, procoagulant state (DIC), and metabolic derangements converging on multiorgan failure. - Robbins, Cotran & Kumar, Fig. 4.20
ATLS Classification of Hemorrhagic Shock
| Parameter | Class I | Class II | Class III | Class IV |
|---|---|---|---|---|
| Blood loss (%) | 0-15 | 15-30 | 30-40 | >40 |
| Pulse (bpm) | <100 | >100 | >120 | >140 |
| Blood pressure | Normal | Normal | Decreased | Decreased |
| Pulse pressure | Normal | Decreased | Decreased | Decreased |
| Respiratory rate | 14-20 | 20-30 | 30-40 | >35 |
| Urine output (mL/hr) | >30 | 20-30 | 5-15 | Negligible |
| CNS | Slightly anxious | Mildly anxious | Anxious/confused | Confused/lethargic |
| Fluid | Crystalloid | Crystalloid | Crystalloid + blood | Crystalloid + blood |
Note: The ATLS classification was empirically derived and not rigorously validated. Children compensate longer (large fluid reserve) and decompensate abruptly; elderly patients show signs of higher-class shock at lower blood loss due to reduced cardiac compensation. - Sabiston Textbook of Surgery, Table 33.1
Compensatory Mechanisms
Sympathetic reflexes are the first line of compensation. When blood pressure drops, baroreceptors and vascular stretch receptors trigger:
- Arteriolar constriction - increases total peripheral resistance
- Venoconstriction - maintains venous return
- Tachycardia - heart rate can rise to 160-180 bpm
These reflexes extend the survivable blood loss from ~15-20% (without reflexes) to 30-40% of total blood volume. - Guyton & Hall
Additional mechanisms include RAAS activation (angiotensin II, aldosterone), ADH release, and stress hormones (cortisol, epinephrine) promoting fluid retention.
Morphological (Organ) Effects
Organ injury is essentially that of hypoxic injury combined with microvascular thrombosis. Key organs affected:
| Organ | Effect |
|---|---|
| Brain | Encephalopathy, ischemic injury |
| Heart | Subendocardial necrosis, decreased contractility |
| Kidneys | Acute tubular necrosis (oliguria, anuria) - most clinically dominant |
| Adrenals | Cortical lipid depletion (increased steroid synthesis from stores) |
| Lungs | Resistant in pure hypovolemia; in sepsis/trauma - diffuse alveolar damage ("shock lung" / ARDS) |
| GI tract | Ischemia, mucosal loss, bacterial translocation in irreversible stage |
Fibrin thrombi form most visibly in renal glomeruli. Except for neurons and cardiomyocytes, affected tissues can fully recover if the patient survives.
Clinical Features
| Feature | Hypovolemic / Cardiogenic | Septic |
|---|---|---|
| Skin | Cool, clammy, cyanotic | Warm, flushed (early; peripheral vasodilation) |
| Pulse | Weak, rapid | Bounding (early), weak (late) |
| BP | Hypotension | Hypotension |
| Respiration | Tachypnea | Tachypnea |
Late manifestations: oliguria, metabolic acidosis (lactic), electrolyte imbalances, multiorgan failure.
Prognosis
- Hypovolemic shock in young, healthy patients: >90% survival with appropriate management
- Septic shock or cardiogenic shock: substantially worse outcomes even with optimal care
Summary - Key Concepts
- Shock = systemic tissue hypoperfusion from reduced CO and/or circulating volume
- Three major types: cardiogenic, hypovolemic, septic (distributive); also neurogenic and anaphylactic
- Septic shock - dysregulated host response involving TLR activation, cytokine storm, endothelial injury, DIC, metabolic derangements
- Three stages: compensated → progressive (lactic acidosis, DIC) → irreversible (organ failure, death)
- Management targets the underlying cause: volume resuscitation (hypovolemic), vasopressors (distributive), inotropes (cardiogenic), antibiotics + source control (septic), epinephrine (anaphylactic)
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology; Sabiston Textbook of Surgery; Guyton & Hall Textbook of Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.