Ceramic on ceramic THR
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ceramic on ceramic" AND "total hip arthroplasty"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information. Let me compile the full answer.
Ceramic-on-Ceramic (CoC) Total Hip Replacement
Overview
Ceramic-on-ceramic (CoC) bearings are a type of hard-on-hard articulation used in total hip arthroplasty (THA). The bearing pair consists of an alumina (or alumina-composite) ceramic femoral head and a ceramic acetabular insert seated within a metal shell. The primary motivation for their development was minimizing polyethylene wear debris and the associated osteolysis/aseptic loosening seen with conventional metal-on-polyethylene designs.
Material Properties
The current standard material is alumina ceramic (Al₂O₃), with modern devices using alumina matrix composite (e.g., BIOLOX delta - CeramTec), which blends alumina with zirconia particles for improved fracture toughness.
Key material characteristics:
- Very high surface hardness - more scratch-resistant than metal
- Surface finish smoother than metal implants due to high density
- Highest Young's modulus (stiffest implant material) compared to cobalt-chrome, titanium, and zirconia-reinforced alumina
- Biologically inert debris - no ionization, no cancer risk, no dysplastic/metaplastic effects on local soft tissues
Wear performance: Alumina-on-alumina wear rate has been shown to be 4000 times less than cobalt-chrome on polyethylene. Hamadouche et al. measured ceramic wear at less than 0.025 mm/year at minimum 18.5-year follow-up.
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 247
Generations of Ceramic Implants
1st and 2nd generation (early - disappointing results):
- Flawed implant design with very thick neck required for strength
- Thick neck adversely reduced the head-neck ratio
- Poor manufacturing technique, low ceramic density, coarse microstructure
- High fracture rates, inadequate fixation, occasional rapid wear with osteolysis
3rd generation alumina (improved):
- Hot isostatic pressing (HIP) manufacturing technique
- High ceramic density, finer microstructure
- Skirt elimination - better head-neck ratio
- Substantially lower fracture rate
4th generation - Alumina Matrix Composite (delta ceramic):
-
Fracture rate approximately 1 in 100,000 (0.001%) vs. 1 in 5,000 (0.02%) with pure alumina
-
Excellent wear properties and increased fracture toughness
-
Miller's Review of Orthopaedics 9th Ed, p. 447
Advantages
| Feature | Detail |
|---|---|
| Lowest wear rate | Less linear and volumetric wear than metal-on-metal (MoM) |
| Fewer particles | Fewer particles generated than MoM |
| Bioinert debris | No ionization, no carcinogenicity |
| No systemic toxicity | No adverse systemic effects reported |
| No osteolysis risk | Particles do not stimulate macrophage-mediated bone resorption the way PE particles do |
| Ideal for young/active patients | Long-term wear performance especially suited to patients expected to outlive a polyethylene bearing |
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 246-247
- Bailey & Love's Short Practice of Surgery 28th Ed, p. (Table 39.6)
Disadvantages
1. Hip Squeaking
- Reported incidence: up to 10% of CoC bearings, though generally lower in most series
- Onset typically >1 year after implantation
- Psychologically distressing; may require revision
Pathophysiology ("perfect storm"):
- Implant malpositioning
- Lever-range wear (microseparation during swing phase of gait)
- Stripe wear - arcuate area of roughness on head/cup from repetitive subclinical subluxation at extremes of motion (e.g., rising from a chair)
- Disrupted lubrication
- Implant resonance - vibrational resonance amplified by the prosthetic construct into the audible range
Treatment: Revision to PE bearing with head change (head is damaged by the squeak)
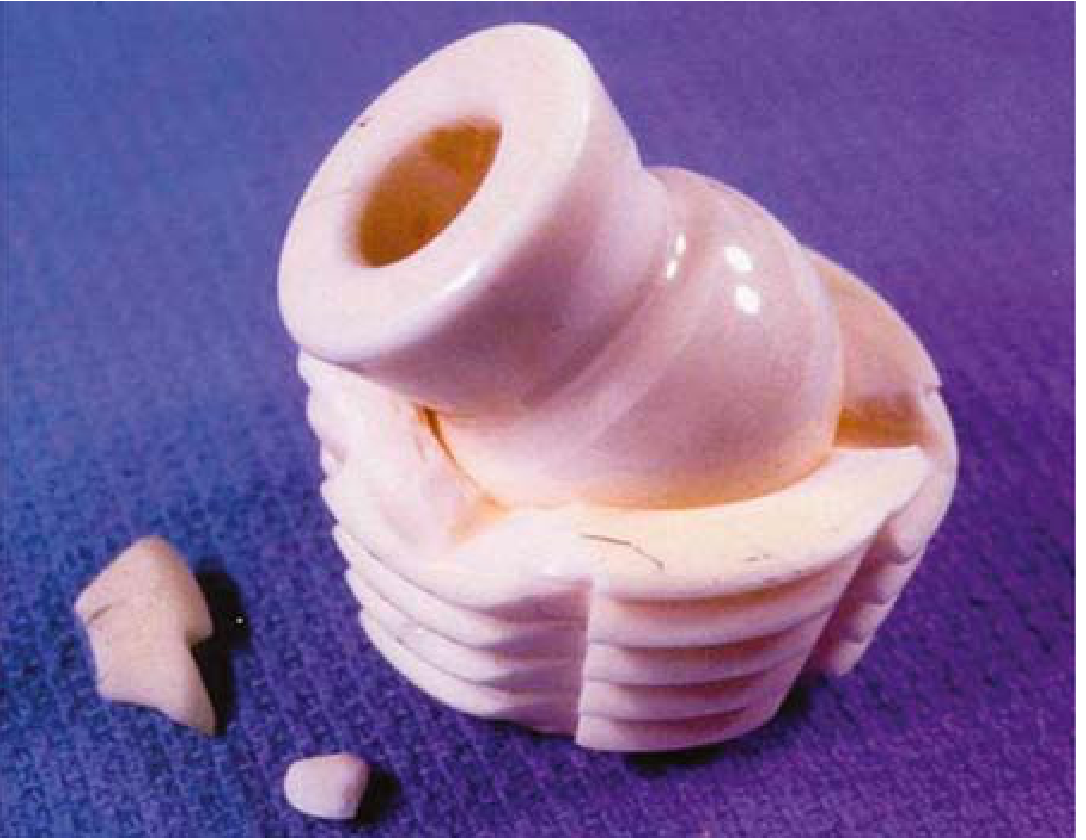
2. Fracture
- Historically a major concern due to ceramic's low toughness
- More common with smaller head sizes (28 mm) and shorter neck lengths
- Modern alumina matrix composite: fracture rate ~0.001% (very low)
- Fracture treatment: Replace with another CoC bearing - because microscopic ceramic shards remain after fracture and are severely abrasive; placing a traditional PE bearing risks rapid PE wear (highly cross-linked PE is preferred if PE bearing used after ceramic fracture)
3. Head Size Limitation
- Ceramic socket must sit within a metal acetabular shell, and must have minimum thickness to resist fracture
- This limits the ultimate head size achievable
- Stability is less than large-diameter MoM bearings
- Fluid film lubrication is less optimal with smaller head radii
4. Head Length / Offset Limitation
- No skirted heads available - limited neck length options
- Can limit hip offset, predisposing to hip impingement and instability
- Careful preoperative templating required
5. Component Constraints
- Lipped and offset liners are unavailable
- Locking mechanism not universally compatible between manufacturers
- Chipping on implantation reported - careful assembly required to ensure insert is properly oriented before impaction
6. Cost
- Significantly more expensive to manufacture than polyethylene bearings
7. Stripe Wear / Edge Loading
- CoC is more sensitive to implant malposition than other bearings
- Excessively vertical cup orientation leads to greater ceramic wear and edge loading
- More demanding surgical technique required
Surgical Considerations
Acetabular component:
- Ceramic insert mates with metal shell via taper junction
- Some manufacturers use metal backing to protect the insert rim from impingement
- Special care during insertion - the insert must be correctly oriented before impaction
Femoral component:
- Limited range of neck lengths available
- No skirted heads
- If placing a new ceramic head on a previously used femoral neck (revision): must use a ceramic head fitted with an internal titanium adapter sleeve - a roughened/corroded trunnion can cause burst fracture of a bare ceramic head
Cup orientation: Excessive acetabular abduction (vertical cup) is particularly problematic - increases stripe wear and squeaking risk.
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 247
Oxidized Zirconium (Ceramicized Metal) - Related Material
OXINIUM (Smith & Nephew) is a zirconium metal alloy with a ~5 µm zirconia ceramic surface generated by oxidation. It has ceramic-surface properties (hardness, smoothness, wettability) but no risk of chipping/fracturing because the surface is integral to the metal substrate. Currently available only as femoral head paired with polyethylene - not available as a CoC couple. Recommended for patients with confirmed metal hypersensitivity.
Indications / Patient Selection
CoC bearings are most suitable for:
- Young, active patients - where long-term wear performance justifies cost and specific complication profile
- Patients in whom osteolysis from PE wear is a dominant concern
- Patients without metal hypersensitivity who need hard-on-hard bearing for wear reduction
Recent Evidence (2024-2026)
A 2024 systematic review and meta-analysis (Wu T et al., PeerJ 2024) compared CoC vs. ceramic-on-polyethylene (CoP) in THA and found CoC had lower wear rates but a higher incidence of squeaking. A June 2026 meta-analysis (Boutros M et al., Eur J Orthop Surg Traumatol, PMID 42295433) and a June 2026 network meta-analysis (Liang Q et al., Medicine, PMID 42260839) continue to examine comparative outcomes of different bearing couples, confirming CoC's superior wear profile but highlighting squeaking and fracture as the characteristic complications to counsel patients about.
Summary: CoC bearings offer the lowest wear rate of all bearing couples and are biologically inert, making them an excellent choice for younger/active patients. The key unique complications are hip squeaking (up to 10%), fracture (historically significant, now very rare with delta ceramic at ~0.001%), and stripe wear from edge loading - all largely related to implant positioning and design.
Create a decision-making guide for CoC vs. other bearing couples
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.