Explain the abdominal segment of the esophagus its vasculature and lymphatic drainage
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough answer.
Abdominal Segment of the Esophagus
General Description
The abdominal esophagus is the shortest and most distal portion of the esophagus. It measures approximately 3–6 cm in length and begins where the esophagus exits the thorax through the esophageal hiatus of the diaphragm (formed by the right crus), at the level of vertebra T10. It ends at the cardial orifice of the stomach, slightly to the left of the midline.
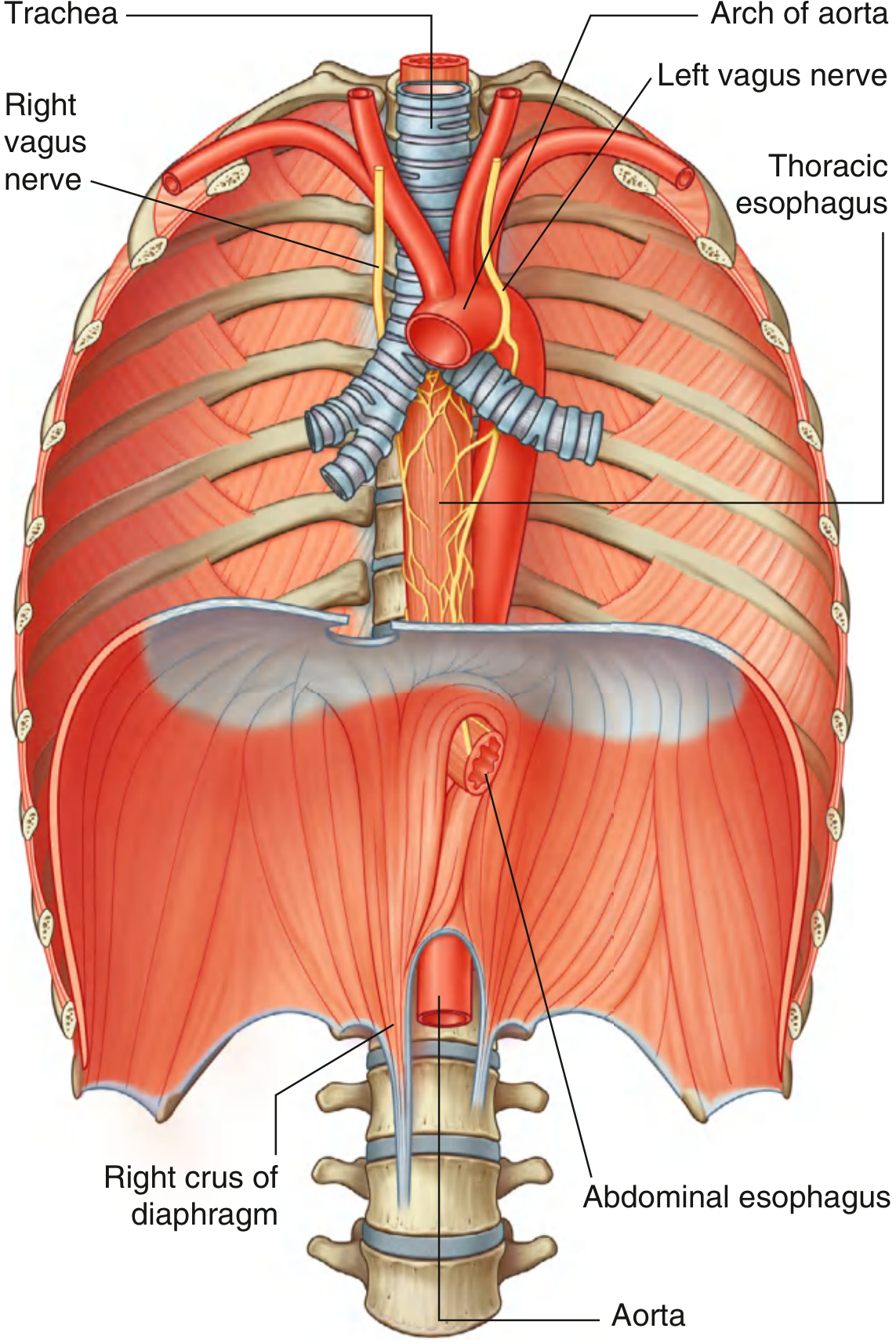
The abdominal esophagus emerging through the right crus of the diaphragm, with vagal trunks descending on its surface — Gray's Anatomy for Students
Key Structural Features
Phrenoesophageal Membrane
The abdominal esophagus is wrapped circumferentially by the phrenoesophageal membrane (ligament of Laimer), a reflection of the endoabdominal fascia:
- Its ascending (upper) leaf courses approximately 1–2 cm above the level of the hiatus.
- Its descending (lower) leaf merges with the serosa of the stomach.
- At the lower leaf, a notable paraesophageal fat pad marks the location of the gastroesophageal junction (GEJ).
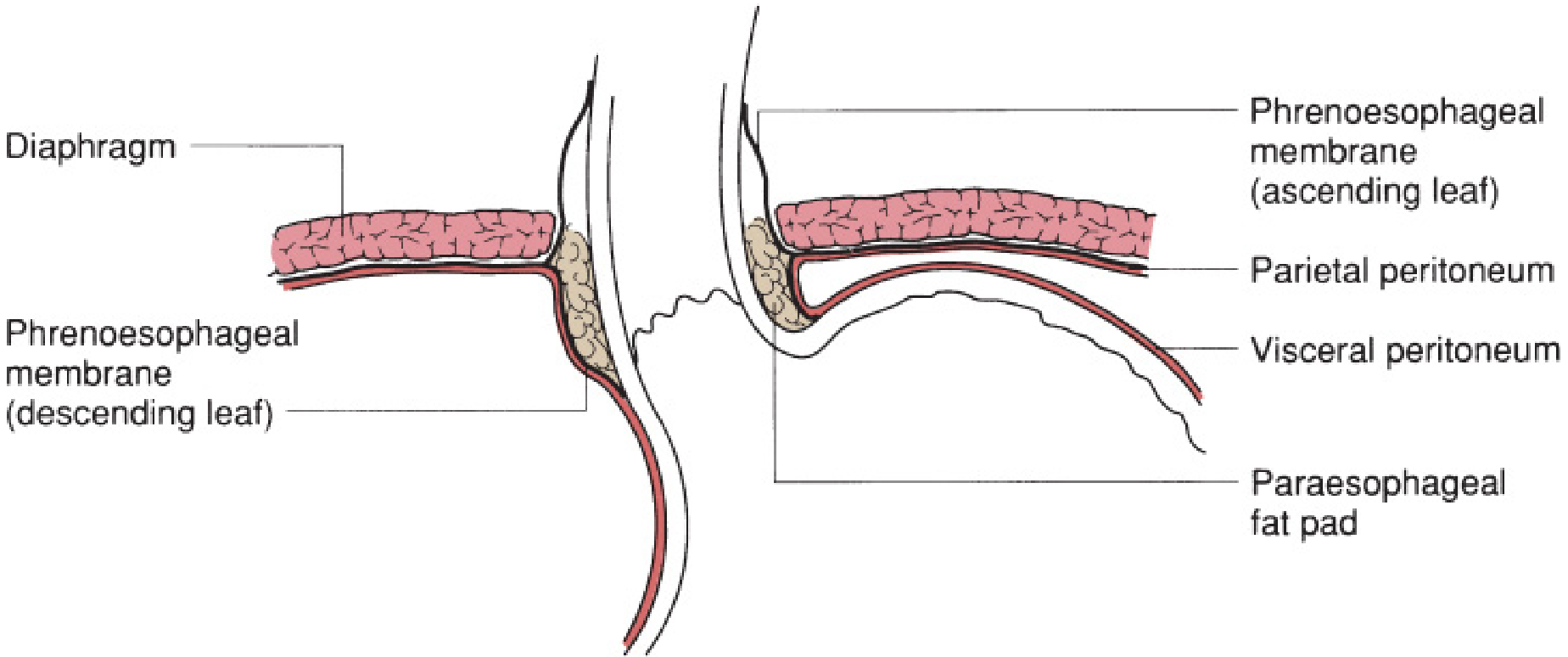
Anatomy of the esophageal hiatus and phrenoesophageal membrane — Mulholland & Greenfield's Surgery
Lower Esophageal Sphincter (LES)
The abdominal esophagus constitutes the abdominal portion of the LES, a high-pressure zone ~3–4 cm in length. The LES has no macroscopic mucosal or external surface changes but is maintained as a functional sphincter. The crura of the diaphragm form a muscular "sling" around it, originating from tendinous bands on the anterolateral surface of L1. The median arcuate ligament lies immediately anterior to the aorta and attaches the crura posteriorly.
Vagal Trunks
As the esophagus enters the abdominal cavity, it is accompanied by the anterior and posterior vagal trunks:
- Anterior vagal trunk: composed of several smaller trunks; fibers predominantly from the left vagus nerve (rotational gut development moves it anteriorly).
- Posterior vagal trunk: a single trunk; fibers predominantly from the right vagus nerve (rotation moves it posteriorly).
Arterial Supply
The arterial supply to the abdominal esophagus is segmental and comes from two main sources:
| Artery | Origin | Notes |
|---|---|---|
| Esophageal branches of the left gastric artery | Celiac trunk | Primary supply; ascends along the lesser curvature |
| Esophageal branches of the left inferior phrenic artery | Abdominal aorta | Approaches from the left side of the hiatus |
Occasional accessory branches may arise from the splenic artery or short gastric arteries (Netter's Atlas).
These vessels anastomose with one another and with the thoracic esophageal supply (bronchial arteries, direct aortic branches) via a dense submucosal arterial network, which is why esophageal infarction is rare despite segmental supply.
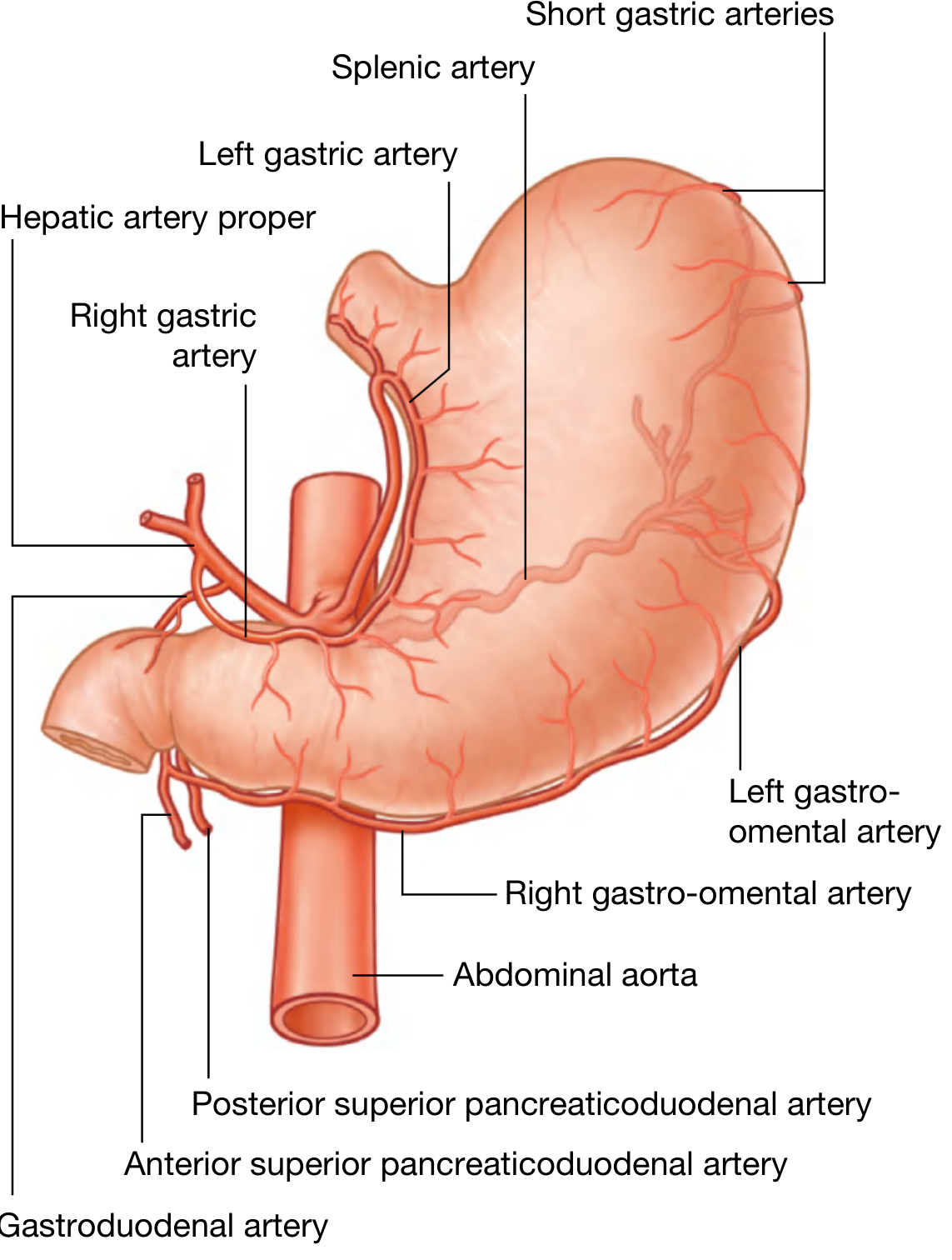
Arterial supply to the abdominal esophagus and stomach — Gray's Anatomy for Students, Fig. 4.64
Venous Drainage
Venous drainage of the abdominal esophagus flows into the portal system via:
- Left gastric (coronary) vein → portal vein
- Short gastric veins → splenic vein → portal vein
This is clinically critical: the submucosal venous plexus of the distal esophagus represents a portosystemic anastomosis. In portal hypertension, increased portal pressure is transmitted to these submucosal veins, producing esophageal varices, which are prone to life-threatening hemorrhage.
(The mid-esophagus drains to the azygos system [systemic], and the upper esophagus to the superior vena cava — making the distal esophagus the key portosystemic junction.)
Lymphatic Drainage
The lymphatics of the esophagus follow a segmental but highly interconnected pattern:
- Abdominal (distal) esophagus → celiac lymph nodes and left gastric (coronary) lymph nodes
These nodes lie along the left gastric artery and around the celiac trunk. However, an important surgical caveat: the submucosal lymphatic channels of the esophagus run longitudinally for long distances before penetrating the muscular wall to reach regional nodes. This means:
- Lymph from the distal esophagus can drain superiorly into mediastinal nodes (and vice versa).
- Most esophageal cancers present with lymph node involvement beyond their regional level at the time of diagnosis, because of this extensive longitudinal network.
Summary of Segmental Lymphatic Drainage
| Esophageal Segment | Primary Lymph Node Groups |
|---|---|
| Cervical esophagus | Deep cervical nodes, paratracheal nodes |
| Thoracic (mid) esophagus | Superior & posterior mediastinal nodes |
| Abdominal (distal) esophagus | Celiac nodes, left gastric (gastric) nodes |
Clinical Relevance
- Hiatal hernia: Laxity of the phrenoesophageal membrane allows the abdominal esophagus and gastric cardia to herniate superiorly into the thorax.
- GERD: Loss of the normal intra-abdominal pressure effect on the LES segment reduces competence of the GEJ.
- Esophageal varices: Portal hypertension shunts blood through the left gastric and short gastric veins into the submucosal plexus at the distal esophagus.
- Esophageal cancer staging: Distal esophageal/GEJ cancers spread to celiac nodes; involvement of celiac nodes (N3 disease in some staging systems) significantly worsens prognosis.
- Surgical access: Mobilization of the abdominal esophagus during fundoplication or esophagectomy requires careful identification of the vagal trunks, left gastric vessels, and phrenoesophageal membrane.
Sources:
- Gray's Anatomy for Students, Chapter 4 (Abdomen)
- Mulholland & Greenfield's Surgery, Chapter 42 (Esophageal Anatomy and Function)
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Chapter 43 (Circulation)
- Goldman-Cecil Medicine, Normal Anatomy and Physiology of the Esophagus
This is a shared conversation. Sign in to Orris to start your own chat.