GERD treatment
Reading File
Finding Sources
Searching PubMed
"gastroesophageal reflux disease" AND treatment
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive answer. Here is the full GERD treatment overview:
GERD Treatment
Overview
GERD results from failure of the anti-reflux barrier - reduced lower esophageal sphincter (LES) tone, frequent transient LES relaxations (TLESRs), hiatal hernia, impaired esophageal clearance, and increased intra-gastric pressure (e.g., obesity). Treatment is stepwise: lifestyle modification → pharmacotherapy → surgery.
1. Lifestyle Modifications (First Step for All Patients)
These are foundational and should accompany any drug therapy:
- Weight loss - obesity raises intra-gastric pressure and is one of the most impactful modifiable factors
- Elevate head of bed - reduces nocturnal reflux
- Avoid recumbency after meals - wait at least 3 hours before lying down
- Dietary triggers - limit fatty foods, chocolate, caffeine, alcohol, citrus, and carbonated beverages
- Smoking cessation - nicotine relaxes the LES
- Avoid tight-fitting clothing - reduces abdominal pressure
2. Pharmacotherapy
Step-Up Approach
| Agent Class | Role | Notes |
|---|---|---|
| Antacids | Mild, infrequent symptoms only | Fast but short-lived; insufficient for erosive disease |
| H2 Receptor Antagonists (H2RAs) | Mild-moderate GERD | Nocturnal dosing adequate for mild cases; tolerance develops with regular use |
| Proton Pump Inhibitors (PPIs) | First-line for typical GERD, erosive esophagitis | Clearly superior to H2RAs for symptom resolution and mucosal healing |
A. H2 Receptor Antagonists
For mild symptoms, nocturnal dosing of an H2RA may suffice, but twice-daily dosing is usually required. Tolerance (tachyphylaxis) develops with regular use, which limits long-term effectiveness.
| Drug | Adult Dose |
|---|---|
| Cimetidine | 400 mg 4x/day or 800 mg twice daily × 12 weeks |
| Famotidine | 10-20 mg twice daily × up to 12 weeks |
| Ranitidine | 150 mg twice daily |
| Nizatidine | 150 mg twice daily |
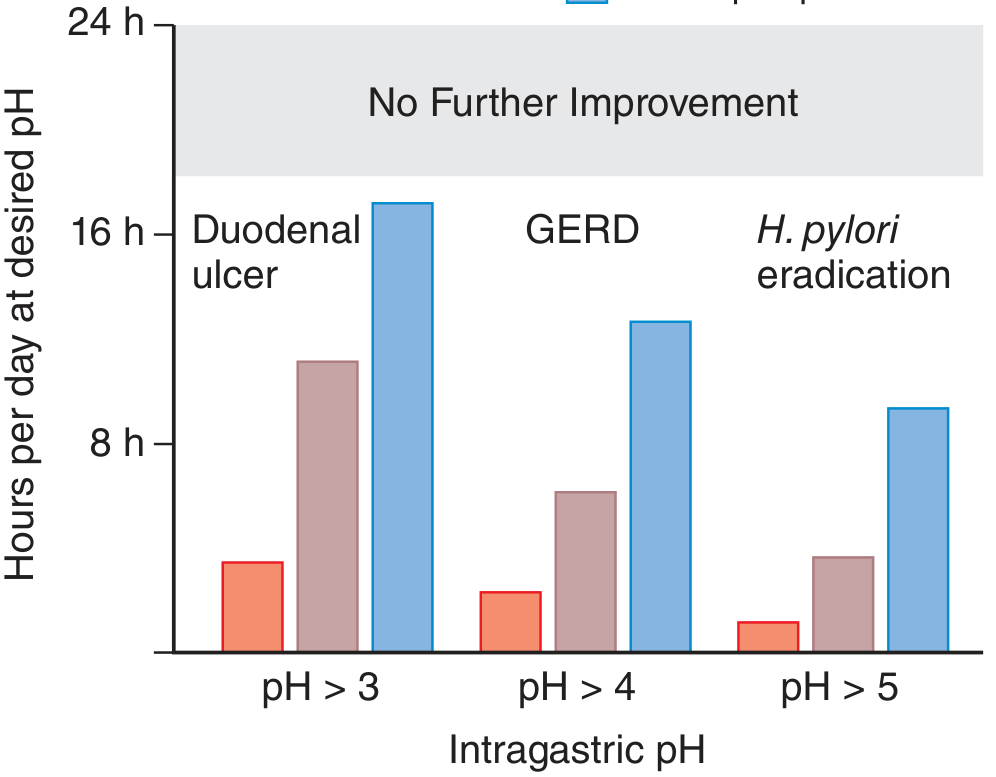
B. Proton Pump Inhibitors (PPIs) - Cornerstone of Treatment
Empiric PPI therapy for 4-8 weeks (single or double dose) is the standard initial approach for typical GERD without alarm features, per Harrison's 22E. PPIs achieve the target intragastric pH >4 (required for GERD) far more reliably and for longer durations than H2RAs, as illustrated below:
Standard PPI dosing for GERD (take 30-60 minutes before a meal for maximal efficacy):
| PPI | Dose |
|---|---|
| Esomeprazole | 20-40 mg daily × 4-8 weeks |
| Dexlansoprazole | 30 mg daily (non-erosive); 60 mg daily (erosive) × 4 weeks |
| Omeprazole | 20-40 mg daily |
| Lansoprazole | 15-30 mg daily |
| Pantoprazole | 40 mg daily |
| Rabeprazole | 20 mg daily |
Severe symptoms / nocturnal acid breakthrough: Twice-daily PPI dosing may be needed. Some add an H2RA at bedtime, though the benefit is short-lived due to tolerance.
Refractory GERD on twice-daily PPI: Up to one-third of GERD patients do not respond to PPI therapy. Options include ambulatory pH-impedance testing and, if esophageal hypersensitivity is identified, tricyclic antidepressants (e.g., amitriptyline, imipramine) to blunt visceral pain processing.
C. Adjunctive Agents
- Baclofen (GABA-B agonist): Reduces TLESRs by ~40% - useful for patients with refractory regurgitation of acid or non-acid fluid. - Harrison's 22E
- Prokinetics (e.g., metoclopramide): Generally not useful for refractory GERD alone or combined with acid suppressants; significant side-effect profile (tardive dyskinesia, especially in elderly).
- Antacids: Adequate only for infrequent, mild acute reflux episodes.
D. Complications Requiring Specific Treatment
- Strictures: Respond better to PPIs than H2RAs.
- Barrett's esophagus: More refractory - neither acid suppression nor antireflux surgery has been shown to convincingly produce regression of metaplasia. Surveillance endoscopy required; ablation (e.g., radiofrequency) for high-grade dysplasia.
- Extraesophageal manifestations (laryngitis, chronic cough, asthma, noncardiac chest pain): Twice-daily PPI is first-line; some require empiric 8-12 week trials before judging response.
3. Diagnostic Work-Up Before Escalating Treatment
- No alarm features + typical symptoms: Treat empirically with PPI × 4-8 weeks; no endoscopy needed.
- Alarm features (dysphagia, odynophagia, unexplained weight loss, recurrent vomiting, GI bleeding, jaundice, palpable mass, family history of GI malignancy): Refer promptly for upper endoscopy.
- Heartburn >5 years, especially age >50: Endoscopy to screen for Barrett's metaplasia.
- PPI-refractory symptoms: Ambulatory pH-impedance monitoring (on-PPI) to identify esophageal hypersensitivity vs. continued acid reflux vs. non-acid regurgitation.
- Pre-surgical evaluation: High-resolution esophageal manometry to assess LES and body peristalsis before fundoplication.
4. Surgical Treatment
Antireflux surgery (fundoplication) is appropriate for:
- Young patients requiring lifelong therapy
- Typical heartburn documented as acid-reflux on pH monitoring
- Good response to PPIs (predicts good surgical outcome)
- Prominent regurgitation refractory to PPIs
Laparoscopic Nissen fundoplication (LNF) is the gold standard procedure. The LOTUS trial demonstrated equivalence of laparoscopic antireflux surgery vs. esomeprazole for chronic GERD.
Predictors of poor surgical outcome:
- Atypical reflux symptoms without documented pathologic acid reflux
- Esophageal body motor disturbances on manometry
- Delayed gastric emptying
Long-term complications of fundoplication: dysphagia, gas-bloat syndrome, gastroparesis; ~60% develop recurrent GERD symptoms over time.
Special consideration - obesity: Fundoplication in obese patients carries higher risk of hiatal hernia recurrence due to elevated intra-abdominal pressure. Roux-en-Y gastric bypass is preferred in obese patients with GERD. - Sabiston Textbook of Surgery
Magnetic sphincter augmentation (LINX device): An emerging alternative to fundoplication; less gas-bloat but limited long-term data.
Summary Algorithm
Typical GERD symptoms (no alarm features)
↓
Lifestyle modifications (all patients)
↓
PPI × 4-8 weeks (empiric, no endoscopy needed)
↓
Symptoms resolved → consider step-down / on-demand therapy
↓ (if not resolved)
Optimize: take PPI 30-60 min before meal, twice-daily dosing
↓ (if still refractory)
pH-impedance monitoring → identify mechanism
↓
Consider: baclofen, TCA, or surgical referral
Sources:
- Harrison's Principles of Internal Medicine, 22E (2025) - Ch. 48
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Ch. 53
- Sabiston Textbook of Surgery - Ch. 18
- Current Surgical Therapy, 14E
This is a shared conversation. Sign in to Orris to start your own chat.