Parkinson's disease 10 marks
Reading File
Finding Sources
Searching PubMed
"Parkinson disease"[MeSH Terms] AND "review"[pt]
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile a complete 10-mark answer.
Parkinson's Disease
Definition
Parkinson's disease (PD) is a chronic, progressive neurodegenerative disorder characterized by a hypokinetic movement disorder resulting from selective loss of dopaminergic neurons in the substantia nigra pars compacta, with intraneuronal accumulation of α-synuclein (Lewy bodies).
- Robbins & Kumar Basic Pathology, p. 854
- Goldman-Cecil Medicine, Chapter 378
Epidemiology
- Symptoms typically emerge between 55–65 years of age
- Second most common neurodegenerative disease after Alzheimer's
- A 2024 systematic review (Lancet Healthy Longev, PMID 38945129) documented rising global prevalence of PD from 1980 to 2023, with increasing incidence linked to aging populations
Pathogenesis
Key molecular events:
- α-synuclein accumulation — normally involved in synaptic transmission; in PD it misfolds, aggregates, and forms Lewy bodies (cytoplasmic eosinophilic inclusions containing α-synuclein, neurofilaments, and ubiquitin)
- Defective autophagy/lysosomal clearance — mutations in Parkin, LRRK2 (most common autosomal dominant mutation), and glucocerebrosidase all impair protein/organelle clearance
- Mitochondrial dysfunction — toxins (MPTP in synthetic heroin, pesticides) selectively injure dopaminergic neurons via mitochondrial inhibition
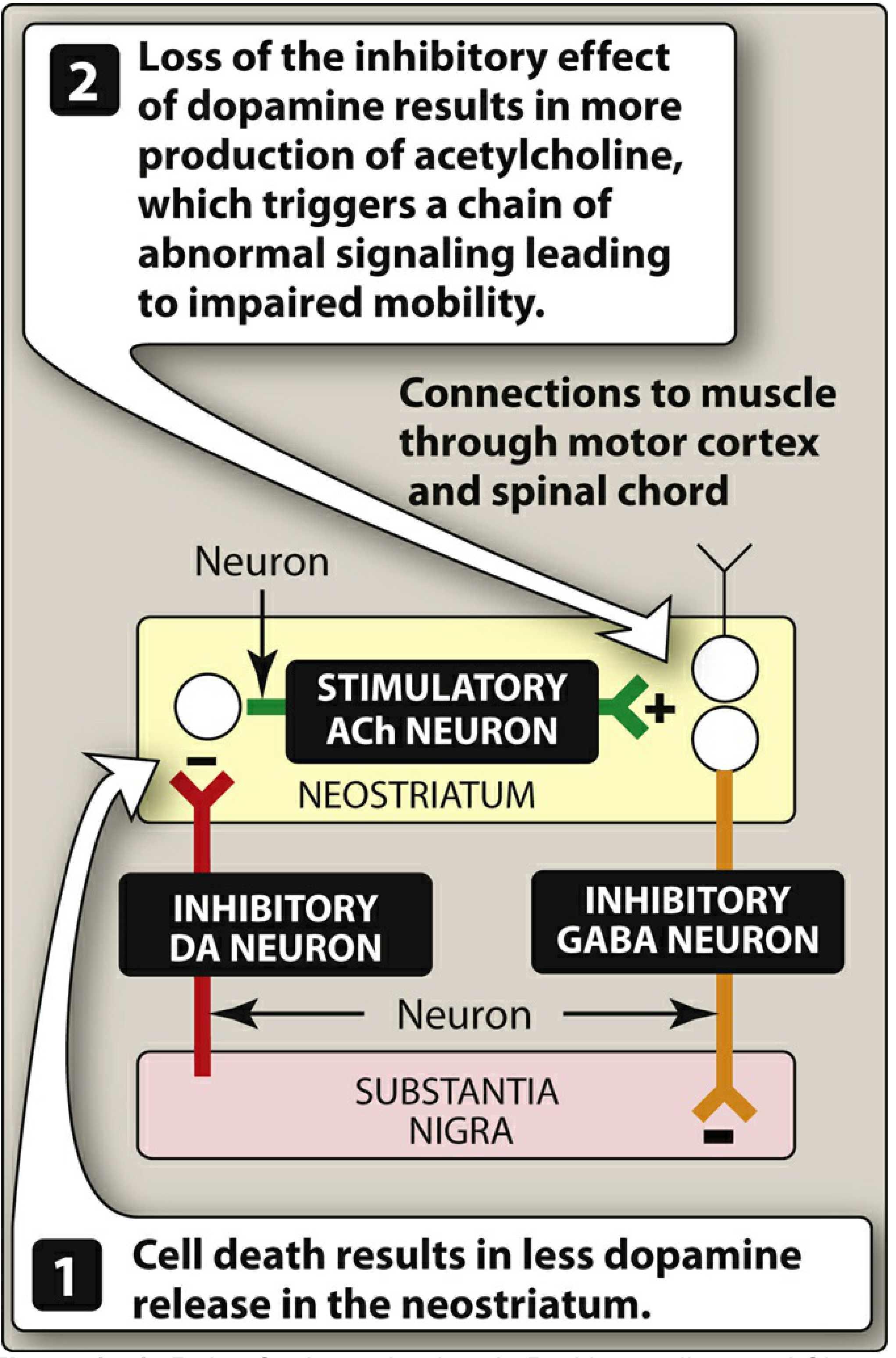
- Nigrostriatal pathway disruption — dopaminergic neurons project from substantia nigra → striatum; their loss removes inhibitory dopamine input to the neostriatum, causing relative cholinergic overactivity
Lippincott Illustrated Reviews: Pharmacology — Role of substantia nigra in Parkinson disease
Morphology
Gross: Pallor of the substantia nigra (depigmentation due to neuronal loss) and locus ceruleus.
Microscopic:
- Loss of pigmented catecholaminergic neurons with reactive gliosis
- Remaining neurons contain Lewy bodies — round, eosinophilic cytoplasmic inclusions with a dense pink center and lighter halo
- Lewy neurites — dystrophic neurites containing aggregated α-synuclein
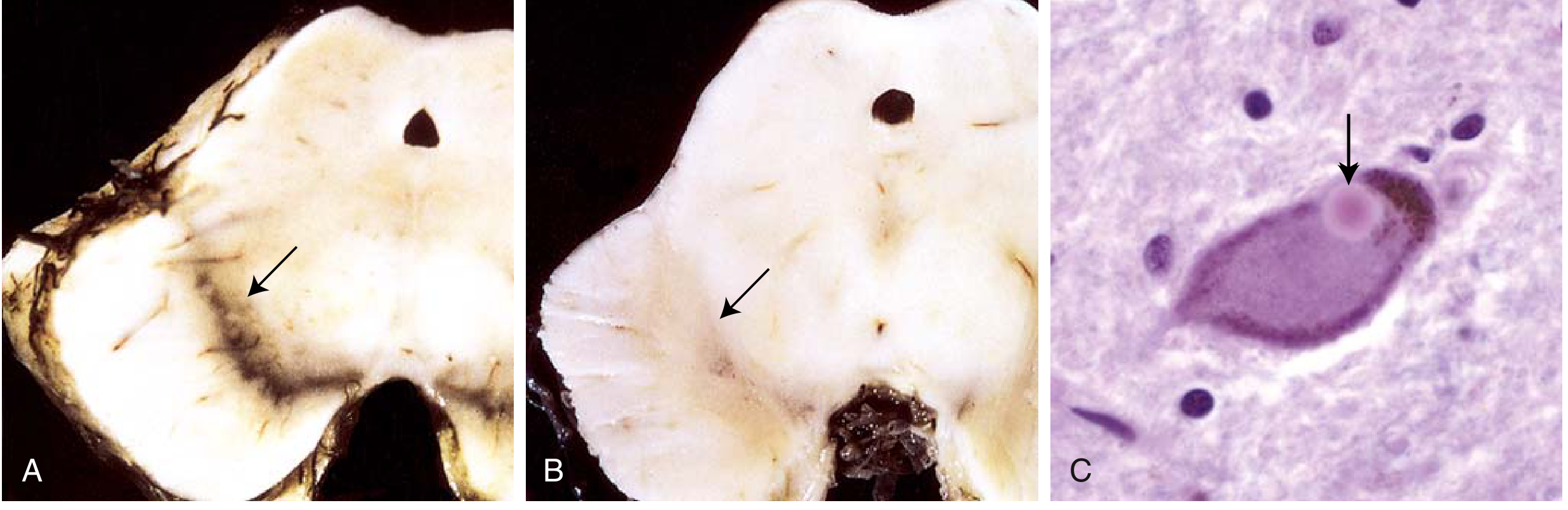
Robbins & Kumar Basic Pathology, Fig. 21.27, p. 855
Clinical Features
Cardinal Motor Features (TRAP)
| Feature | Description |
|---|---|
| Tremor | "Pill-rolling" resting tremor (4–6 Hz), decreases with intentional movement |
| Rigidity | Cogwheel or lead-pipe rigidity; increased muscle tone throughout range of motion |
| Akinesia/Bradykinesia | Slowness of movement initiation and execution; hypomimia ("masked facies"), micrographia, shuffling gait |
| Postural instability | Late feature; impaired righting reflexes; festinating gait; frequent falls |
Non-Motor Features (also diagnostically important)
- Autonomic: Orthostatic hypotension, constipation, urinary dysfunction, sialorrhea
- Neuropsychiatric: Depression, anxiety, apathy, dementia (late), visual hallucinations
- Sleep: REM sleep behavior disorder (may precede motor symptoms by years), excessive daytime sleepiness
- Olfactory: Hyposmia/anosmia — often an early pre-motor symptom
- Dysphagia: Present subjectively in ~35%, objectively in ~82%; silent aspiration occurs in 15–33%
Disease Course
Progressive over 10–15 years; death commonly from aspiration pneumonia or trauma from falls.
Diagnosis
Primarily clinical. Key diagnostic criteria:
- Bradykinesia + at least one of: resting tremor, rigidity
- Asymmetric onset
- Good response to levodopa
Investigations:
- DaT-SPECT scan — reduced dopamine transporter uptake in striatum (useful when clinical diagnosis uncertain)
- MRI brain — mainly to exclude other causes (vascular, structural)
- No blood or CSF biomarker is diagnostic in routine practice
Differential diagnosis includes: Multiple system atrophy (MSA), progressive supranuclear palsy (PSP), corticobasal degeneration, drug-induced parkinsonism (dopamine antagonists — phenothiazines, haloperidol), vascular parkinsonism, dementia with Lewy bodies.
Management
Pharmacological
Goal: Restore dopamine–acetylcholine balance in the striatum.
1. Levodopa + Carbidopa (first-line, most effective)
- Levodopa is a metabolic precursor of dopamine; crosses the blood-brain barrier
- Carbidopa inhibits peripheral DOPA decarboxylase → reduces peripheral dopamine side effects, increases CNS availability
- Standard starting dose: carbidopa/levodopa 25/100 mg three times daily
- Limitation: long-term use causes motor fluctuations ("wearing-off", "on-off" phenomenon) and dyskinesias (~50% by 5 years)
2. COMT Inhibitors (adjunct to levodopa)
- Entacapone, opicapone, tolcapone — inhibit peripheral COMT, reducing conversion of levodopa to 3-O-methyldopa
- Increase levodopa CNS availability; reduce "wearing-off"
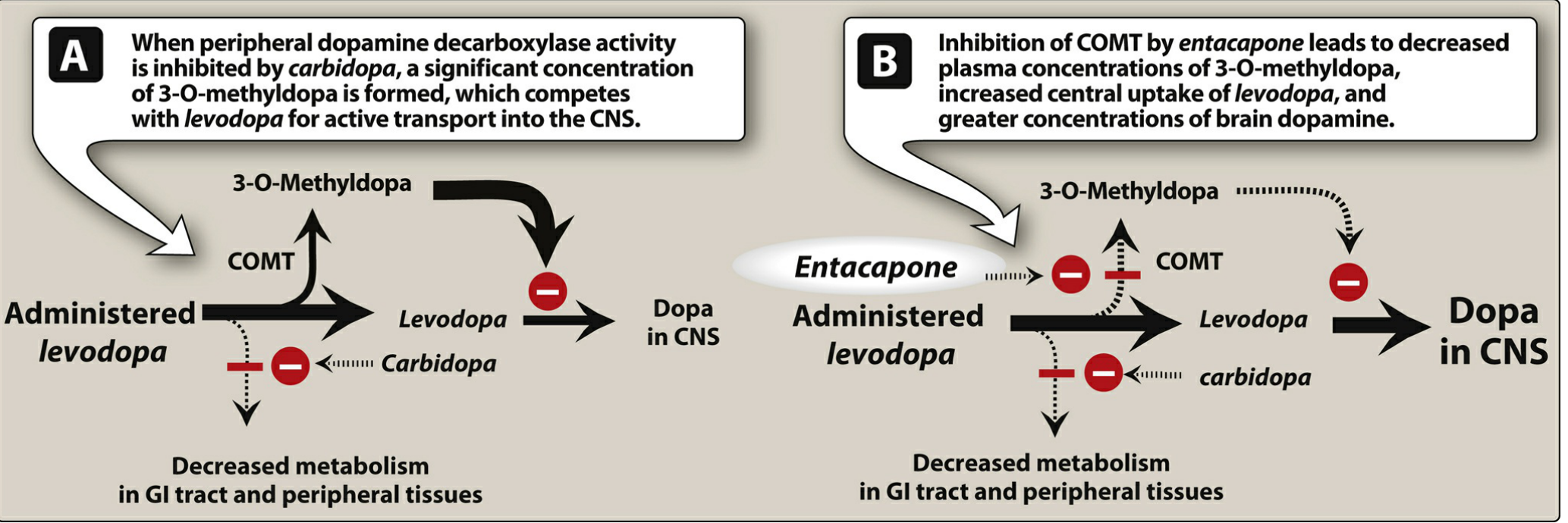
Lippincott Illustrated Reviews: Pharmacology — Effect of entacapone, Fig. 15.9
3. Dopamine Receptor Agonists
- Non-ergot: ropinirole, pramipexole, rotigotine, apomorphine (injectable)
- Longer duration of action than levodopa; used in early disease or for motor fluctuations
- Less dyskinesia risk as initial therapy vs. levodopa
- Side effects: hallucinations, impulse control disorders (especially in elderly)
4. MAO-B Inhibitors
- Selegiline, rasagiline — inhibit monoamine oxidase B, reducing dopamine catabolism
- Used as monotherapy in early disease or adjunct to levodopa
5. Anticholinergics
- Trihexyphenidyl, benztropine — reduce cholinergic overactivity
- Useful mainly for tremor, especially in younger patients
- Avoid in elderly (cognitive side effects)
6. Amantadine
- Mechanism: enhances dopamine release, NMDA antagonism
- Used for dyskinesias and mild early disease
Surgical
Deep Brain Stimulation (DBS)
- Electrodes implanted in the subthalamic nucleus or globus pallidus interna
- Modulates basal ganglia circuitry; allows significant reduction in levodopa dose
- Indicated when medical therapy fails to control motor symptoms
- Improves quality of life, reduces dyskinesias and motor fluctuations
Complications
| Late Motor | Late Non-Motor |
|---|---|
| Freezing of gait (on-period) | Dementia |
| Dysarthria | Psychosis, hallucinations |
| Dysphagia → aspiration pneumonia | Depression, apathy |
| Falls and fractures | Autonomic failure |
| Dyskinesias (peak-dose, diphasic) | REM sleep disorder |
Key Points for Exam
- Lewy body = pathological hallmark (α-synuclein inclusions)
- Substantia nigra depigmentation = gross hallmark
- TRAP = classic motor tetrad
- Levodopa remains the most effective drug; carbidopa prevents peripheral conversion
- DBS targets subthalamic nucleus or globus pallidus interna
- Non-motor features (anosmia, constipation, REM sleep disorder) may predate motor symptoms by years
Sources: Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine 26e; Lippincott Illustrated Reviews: Pharmacology; Bradley and Daroff's Neurology in Clinical Practice; Textbook of Family Medicine 9e
As per b pharmacy syllabus
Reading File
Searching the Web
B Pharmacy syllabus Parkinson's disease pharmacology topics PCI India
Finding Sources
Reading Web Page
https://www.pci.nic.in/pdf/Syllabus_B_Pharm.pdf
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a precise B. Pharmacy (PCI syllabus) answer. The PCI syllabus places Parkinson's disease under Pharmacology-I (4th Semester), Unit V — Drugs acting on CNS, with focus on: etiology, pathophysiology, and drugs used (mechanism, uses, adverse effects). Here is the answer structured exactly for that context:
Parkinson's Disease
(B. Pharm — Pharmacology, 4th Semester | PCI Syllabus)
1. Definition
Parkinsonism is a progressive neurological disorder of muscle movement characterized by:
- Tremors
- Muscular rigidity
- Bradykinesia (slowness of movement)
- Postural and gait abnormalities
It is caused by destruction of dopaminergic neurons in the substantia nigra, with a consequent reduction in dopamine activity in the striatum (basal ganglia).
2. Etiology / Pathophysiology
Normal neurochemistry of the basal ganglia:
- The substantia nigra sends inhibitory dopaminergic neurons to the neostriatum
- The neostriatum also contains excitatory cholinergic (ACh) neurons
- Normally, dopamine (DA) and acetylcholine (ACh) are balanced
In Parkinson's disease:
- Dopaminergic neurons in the substantia nigra are destroyed
- Less dopamine → less inhibition of cholinergic neurons in the neostriatum
- Relative excess of ACh → triggers abnormal motor signaling → loss of movement control
Secondary (drug-induced) parkinsonism: Phenothiazines, haloperidol (dopamine receptor blockers) can cause pseudoparkinsonism.
3. Treatment Strategy
Therapy aims to restore the DA/ACh balance in the neostriatum by either:
- Increasing dopamine (or its effects), OR
- Decreasing acetylcholine (anticholinergics)
4. Drugs Used in Parkinson's Disease
A. Levodopa + Carbidopa (First-line, most effective)
Levodopa (L-DOPA):
- Metabolic precursor of dopamine
- Dopamine itself cannot cross the blood–brain barrier (BBB), but levodopa can
- Converted to dopamine in surviving neurons of the substantia nigra → restores dopaminergic transmission
Why combine with Carbidopa?
- Carbidopa = peripheral DOPA decarboxylase inhibitor
- Prevents conversion of levodopa to dopamine in the periphery
- More levodopa reaches the CNS → better effect with lower dose
- Reduces peripheral side effects (nausea, vomiting, cardiac arrhythmias)
Adverse effects of Levodopa:
| Peripheral | Central |
|---|---|
| Nausea, vomiting | Dyskinesias (involuntary movements) |
| Postural hypotension | "On-off" fluctuations |
| Cardiac arrhythmias | Hallucinations, confusion |
| Anorexia | Mood changes |
"Wearing-off" phenomenon: after years of use, drug effect diminishes before next dose; ~50% of patients develop dyskinesias within 5 years.
B. MAO-B Inhibitors
Selegiline (Deprenyl), Rasagiline
- Inhibit monoamine oxidase type B (MAO-B) — the enzyme that breaks down dopamine in the brain
- Inhibition → increased dopamine concentration in the striatum
- Used as monotherapy in early PD or as adjunct to levodopa to reduce "wearing-off"
- Adverse effects: insomnia, nausea, dizziness (selegiline metabolized to amphetamine)
C. COMT Inhibitors
Entacapone, Opicapone, Tolcapone
- Inhibit catechol-O-methyltransferase (COMT) — a peripheral enzyme that converts levodopa to inactive 3-O-methyldopa
- When added to levodopa/carbidopa → more levodopa reaches the CNS
- Reduce "wearing-off" symptoms
- Tolcapone — risk of fulminant hepatic necrosis; only used if other options fail
- Entacapone/Opicapone — safer; have replaced tolcapone in routine practice
D. Dopamine Receptor Agonists
Bromocriptine (ergot derivative), Ropinirole, Pramipexole, Rotigotine, Apomorphine (non-ergot)
- Directly stimulate D2 dopamine receptors in the striatum (do not require enzymatic conversion)
- Longer duration of action than levodopa
- Used: early PD, or as adjuncts in motor fluctuations
- Less risk of dyskinesias than levodopa
| Drug | Route | Special Feature |
|---|---|---|
| Bromocriptine | Oral | Ergot derivative; may cause fibrosis, vasospasm |
| Pramipexole | Oral | Also for restless legs syndrome; renally excreted |
| Ropinirole | Oral | Also for restless legs syndrome |
| Rotigotine | Transdermal patch | Once daily; steady drug levels |
| Apomorphine | Injectable/sublingual | For acute "off" episodes in advanced PD |
Adverse effects: Nausea, hallucinations, orthostatic hypotension, somnolence, impulse control disorders (uncontrolled spending, hypersexuality, binge eating)
E. Amantadine
- Originally an antiviral drug (accidentally found to have antiparkinsonian action)
- Mechanism:
- Increases dopamine release
- Blocks NMDA (glutamate) receptors
- Mild anticholinergic effect
- Used in early/mild PD; also reduces levodopa-induced dyskinesias
- Less efficacious than levodopa; tolerance develops readily
- Adverse effects: restlessness, agitation, hallucinations, orthostatic hypotension, urinary retention, livedo reticularis
F. Anticholinergic (Antimuscarinic) Agents
Benztropine, Trihexyphenidyl (Benzhexol)
- Block muscarinic receptors → reduce excess cholinergic activity → restore DA/ACh balance
- Mainly useful for tremor and rigidity; less effective for bradykinesia
- Used as adjuncts; preferred in younger patients with tremor-predominant PD
- Contraindicated: glaucoma, prostatic hyperplasia, pyloric stenosis
- Adverse effects (peripheral): Dry mouth, constipation, urinary retention, blurred vision
- Adverse effects (central): Mood changes, confusion, memory impairment (avoid in elderly)
5. Summary Table of Drugs
| Drug Class | Example(s) | Mechanism | Key ADR |
|---|---|---|---|
| Levodopa + DDC inhibitor | Levodopa + Carbidopa | DA precursor + peripheral decarboxylase inhibitor | Dyskinesia, on-off, nausea |
| MAO-B inhibitors | Selegiline, Rasagiline | ↓ DA breakdown | Insomnia |
| COMT inhibitors | Entacapone, Tolcapone | ↓ Peripheral COMT → ↑ levodopa to brain | Hepatotoxicity (tolcapone) |
| DA agonists | Ropinirole, Pramipexole | Direct D2 receptor stimulation | Hallucinations, impulse disorders |
| NMDA antagonist | Amantadine | ↑ DA release + NMDA block | Agitation, confusion |
| Anticholinergics | Benztropine, Trihexyphenidyl | Muscarinic block → ↓ ACh excess | Dry mouth, confusion |
Source: Lippincott Illustrated Reviews: Pharmacology (PCI recommended textbook) — Chapter 15
This is a shared conversation. Sign in to Orris to start your own chat.