Ards
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute respiratory distress syndrome" ARDS management
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have everything needed for a thorough, well-illustrated answer. Here it is:
Acute Respiratory Distress Syndrome (ARDS)
Definition
ARDS is a syndrome of noncardiogenic pulmonary edema accompanied by severe lung inflammation, hypoxemia, and decreased lung compliance, leading to acute respiratory failure. It was first described in 1967 by Ashbaugh and colleagues in 12 patients who presented with bilateral opacities, hypoxemia, and low compliance - many following trauma or viral infection. - Murray & Nadel's Textbook of Respiratory Medicine
Berlin Criteria (2012) - Diagnostic Standard
The Berlin Definition replaced the older AECC (1994) criteria and remains the current standard. All four criteria must be met:
| Criterion | Requirement |
|---|---|
| Timing | Onset within 1 week of a known clinical insult or new/worsening respiratory symptoms |
| Chest imaging | Bilateral opacities on CXR or CT not explained by effusions, lobar collapse, or nodules |
| Origin of edema | Not fully explained by cardiac failure or fluid overload (echocardiography if no risk factor) |
| Hypoxemia (PaO2:FiO2) | Measured on PEEP ≥ 5 cmH2O |
Severity Classification by P:F Ratio
| Severity | PaO2:FiO2 (on PEEP ≥5) |
|---|---|
| Mild | 201-300 |
| Moderate | 101-200 |
| Severe | ≤100 |
Mortality ranges from 20-50% depending on severity. - Current Surgical Therapy 14e
Chest X-Ray Appearance
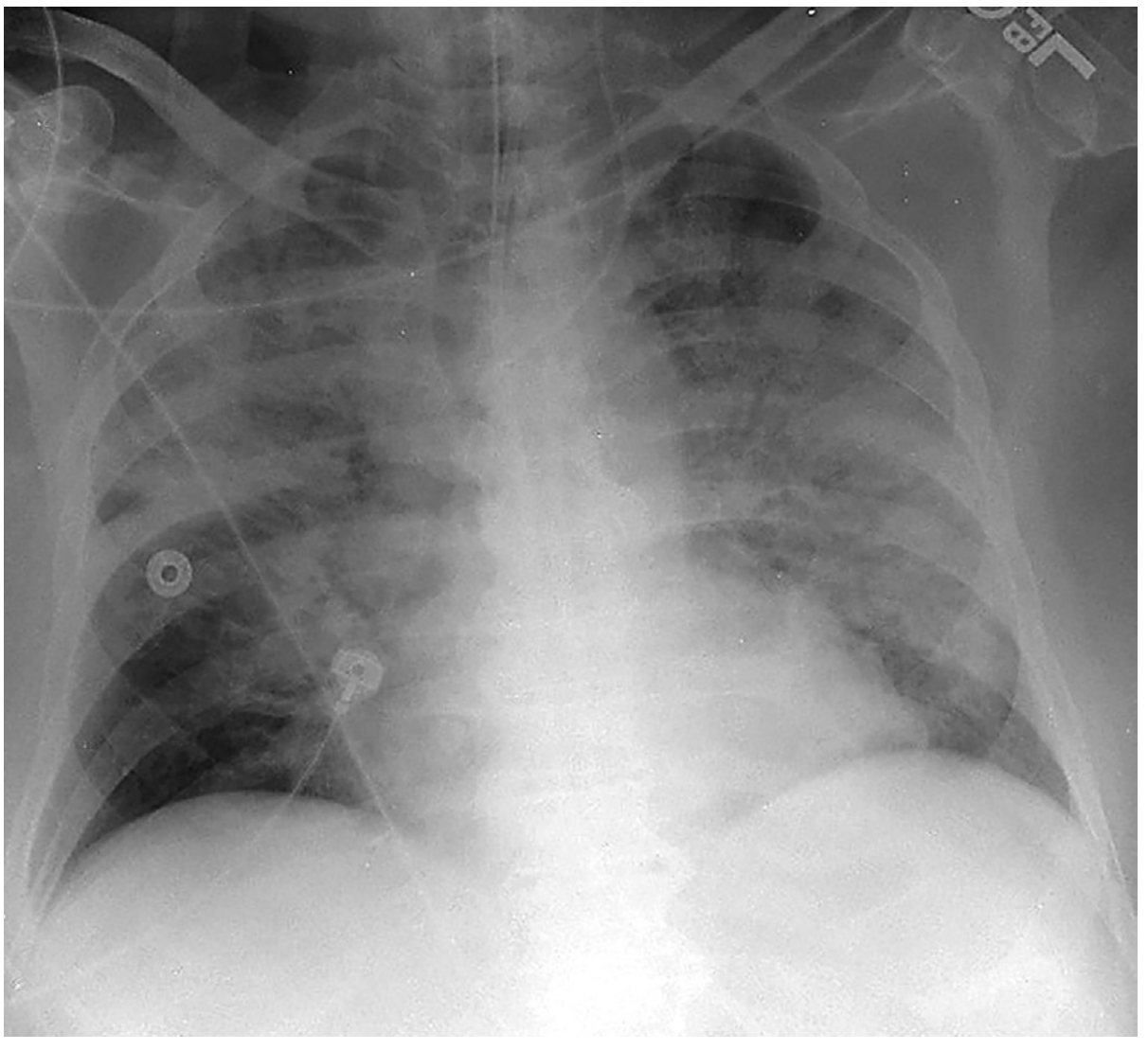
Frontal CXR in a mechanically ventilated patient showing extensive, multifocal, bilateral lung opacities involving all lobes, without features of hydrostatic edema (no interlobular septal thickening or pleural effusion). - Murray & Nadel's
Risk Factors
Risk factors are divided by mechanism of injury:
Direct (Pulmonary) Injury
- Pneumonia (bacterial, viral - including COVID-19, influenza)
- Aspiration of gastric contents
- Pulmonary contusion
- Toxic inhalation
- Near-drowning
- Reperfusion injury (e.g., post-lung transplant)
Indirect (Nonpulmonary) Injury
- Sepsis (strongest risk - up to 43% develop ARDS)
- Major trauma (40% with massive transfusions, 25% with multiple trauma)
- Multiple blood transfusions (>15 units/24h)
- Pancreatitis
- Cardiopulmonary bypass
- Drug overdose / adverse medication effects
Premorbid factors: Chronic alcoholism (RR 2.0) and cigarette smoking further increase risk and worsen prognosis. Having multiple risk factors compounds the incidence. - Murray & Nadel's
Pathophysiology
ARDS is driven by injury to the alveolar-capillary interface:
- Exudative phase (0-7 days): The insult (direct or indirect) activates the immune system, triggering massive cytokine release (TNF-α, IL-1, IL-6, IL-8). This causes increased capillary permeability - protein-rich, inflammatory edema floods the alveoli. Unlike cardiogenic edema (hydrostatic), this is a permeability edema.
- Inflammatory alveolar injury: Type I pneumocytes are destroyed. Surfactant is inactivated, causing alveolar collapse. Hyaline membranes form.
- Consequences: V/Q mismatch and intrapulmonary shunt cause refractory hypoxemia. Decreased compliance drives increased work of breathing. Pulmonary hypertension develops.
- Proliferative phase (7-21 days): Type II pneumocyte proliferation attempts repair; fibroblast infiltration begins.
- Fibrotic phase (>21 days): Some patients develop progressive fibrosis with further impairment of gas exchange. - Murray & Nadel's, Current Surgical Therapy 14e
The hallmark is patchy, heterogeneous injury - normal and abnormal alveoli are adjacent to each other. Posterior, dependent regions preferentially collapse (compression atelectasis).
Management
Treatment is supportive - no pharmacotherapy has been proven to reverse ARDS itself. Management escalates with severity:
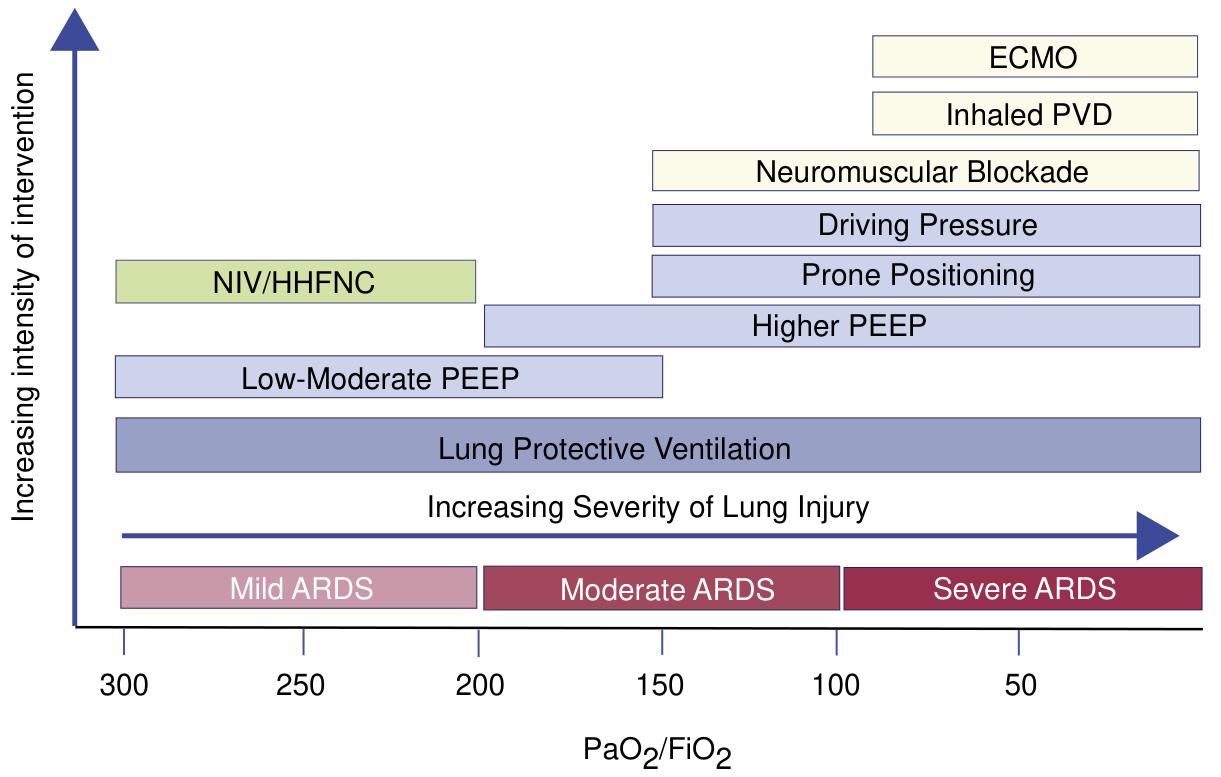
1. Lung Protective Ventilation (all severity - cornerstone)
- Tidal volume: 6 mL/kg of ideal body weight (low VT prevents volutrauma)
- Target plateau pressure ≤30 cmH2O
- Permissive hypercapnia is acceptable
- Shown to reduce mortality in the landmark ARMA trial (ARDSNet)
2. PEEP
- Low-moderate PEEP for mild ARDS
- Higher PEEP for moderate-severe ARDS to recruit collapsed alveoli and reduce FiO2 requirements
- The optimal level is individualized
3. Prone Positioning
- For moderate-severe ARDS (P:F ≤150)
- Improves V/Q matching by recruiting dependent (posterior) alveoli
- 16+ hours/day; the PROSEVA trial showed significant mortality benefit
4. Neuromuscular Blockade
- Consider in moderate-severe ARDS to eliminate patient-ventilator dyssynchrony and reduce oxygen consumption
5. Conservative Fluid Management
- Avoid fluid overload; target euvolemia
- Reduces time on ventilator
6. Driving Pressure Minimization
- Target driving pressure (plateau pressure - PEEP) <15 cmH2O
7. NIV / High-Flow Nasal Cannula (HHFNC)
- May be trialed in mild ARDS in selected, cooperative patients to avoid intubation
8. Salvage Therapies (severe, refractory ARDS)
- Inhaled pulmonary vasodilators (NO, prostacyclins): Improve oxygenation transiently, no proven mortality benefit
- ECMO (VV-ECMO): Last resort for severe refractory hypoxemia (P:F <80); referred to specialized ARDS centers
Treat the Underlying Cause
Identifying and treating the precipitant (e.g., antibiotics for sepsis/pneumonia, surgical source control) is essential. - Current Surgical Therapy 14e, Murray & Nadel's
Corticosteroids - Recent Evidence
A 2026 systematic review and meta-analysis in Annals of Internal Medicine (PMID: 41325621) found that systemic corticosteroids reduce mortality in pneumonia-associated ARDS but also increase infectious complications. A 2024 meta-analysis (PMID: 39165240) supports corticosteroid use in ARDS with careful patient selection, particularly for early moderate-to-severe ARDS. Routine use is not yet standard - patient selection matters.
Long-Term Outcomes
- Survivors often have physical impairment (muscle wasting, reduced exercise tolerance) and psychological sequelae (PTSD, depression, cognitive impairment) - collectively termed Post-Intensive Care Syndrome (PICS)
- Pulmonary function generally recovers over 6-12 months, but some patients have persistent restriction and diffusion impairment - Murray & Nadel's
Key Points Summary:
- ARDS = acute bilateral opacities + hypoxemia (P:F <300 on PEEP ≥5) + not explained by cardiac failure
- Most common triggers: sepsis, pneumonia, aspiration, trauma
- Pathology: permeability edema, diffuse alveolar damage, refractory hypoxemia
- Cornerstone treatment: low VT lung-protective ventilation (6 mL/kg IBW)
- Mortality-reducing strategies (evidence-based): lung protective ventilation, prone positioning (moderate-severe), conservative fluids
- ECMO is a salvage option for severe refractory cases
This is a shared conversation. Sign in to Orris to start your own chat.