Explain how to read or interpretation of chest x ray , mri and CT scan
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have rich textbook content and anatomical images. Let me compile a comprehensive, well-structured answer.
Interpreting Chest X-Ray, CT Scan, and MRI
PART 1: CHEST X-RAY (CXR) INTERPRETATION
Step 0 - Before You Start: Validity Check (RIP)
Before interpreting anything, confirm the technical quality of the film using the RIP acronym:
| Letter | Check | What to Look For |
|---|---|---|
| R | Rotation | Clavicular heads should be equidistant from the vertebral spinous processes (within ~2-3 mm). If one side is farther, the patient was rotated - this distorts mediastinal width. |
| I | Inspiration | Count posterior ribs as they meet the spine. A minimum of 9 posterior ribs must be visible above the diaphragm. Poor inspiration creates false "fluffy" opacities mimicking CHF. |
| P | Penetration | Intervertebral disc spaces should NOT be visible below the diaphragm (over-penetrated). Vertebral bodies should be faintly visible through the cardiac shadow (adequate). |
Standard Views
- PA (Posteroanterior): The standard view. Beam travels back-to-front. Patient stands upright. Best for cardiomegaly assessment.
- AP (Anteroposterior): Portable/bedside. Beam front-to-back. Heart appears magnified - you cannot reliably assess cardiomegaly on AP.
- Lateral view: Always request alongside PA. Without it, lesions in the retrocardiac space and the retrosternal (anterior clear) space will be missed.
Systematic Reading: Use a Top-Down Checklist
Pfenninger and Fowler's Procedures for Primary Care recommends this structured approach:
1. BONES AND SOFT TISSUES
- Scan all visible ribs, clavicles, scapulae, humeral heads, and thoracic spine for fractures, lytic lesions, or sclerotic changes.
- Check soft tissues for subcutaneous emphysema (air in the soft tissue).
2. MEDIASTINUM
- Width: should not exceed 8 cm in adults on PA view. Widening suggests aortic dissection, lymphoma, or substernal goiter.
- Trachea: should be midline; deviation indicates mass effect or collapse.
- Carina angle: Normally <70°. Widening suggests left atrial enlargement.
- Aortic knob: look for calcification, unfolding (tortuous aorta).
3. CARDIAC SILHOUETTE
- Cardiothoracic ratio: Heart width should be less than 50% of the thoracic width on PA view (up to 55% may be acceptable).
- Right heart border = right atrium.
- Left heart border (top to bottom) = aortic knob, pulmonary artery segment, left atrial appendage, left ventricle.
- The silhouette sign is key: when a border is lost (e.g., the right heart border disappears), the adjacent lung lobe is consolidated (right middle lobe pneumonia erases the right heart border; right lower lobe pathology erases the right hemidiaphragm).
4. DIAPHRAGMS
- The right hemidiaphragm is normally higher than the left (by about half an interspace) due to the liver below.
- Blunting of costophrenic angles = pleural effusion (starts at ~200-300 mL).
- Flattened diaphragms = hyperinflation (COPD, asthma).
- Elevated hemidiaphragm = phrenic nerve palsy, subphrenic abscess, or hepatomegaly.
- Air under the diaphragm (on erect film) = bowel perforation.
5. HILA
- The left hilum is normally higher than the right by about 2 cm.
- Both hila are primarily made up of pulmonary arteries.
- Hilar enlargement: bilateral = sarcoidosis, lymphoma; unilateral = malignancy, infection.
- Hilar "dance" on fluoroscopy = pulsatile (vascular) vs. non-pulsatile (lymph node).
6. LUNG PARENCHYMA
This is where most pathology shows up. Key patterns:
| Pattern | Appearance | Common Causes |
|---|---|---|
| Consolidation | Fluffy/dense opacity, air bronchograms | Pneumonia, pulmonary edema, hemorrhage |
| Interstitial | Reticular, nodular, or reticulonodular | ILD, viral pneumonia, pulmonary edema |
| Nodule | 5-30 mm discrete round opacity | Granuloma, primary lung cancer, metastasis |
| Mass | >30 mm | Malignancy until proven otherwise |
| Cavity | Lucency within opacity | TB, abscess, cavitating malignancy |
| Hyperinflation | Increased lucency, flat diaphragms | COPD, emphysema, asthma |
| Atelectasis | Plate-like or lobar collapse, shift of structures | Post-op, mucus plugging |
Cephalization of flow: Normally pulmonary vessels are larger in the lower zones (gravity). When upper zone vessels are larger than lower zone vessels, this indicates elevated pulmonary venous pressure (CHF). Vasculature normally stops 3-5 mm from the chest wall.
7. PLEURA
- Pneumothorax: Absence of pulmonary vasculature extending to the inner bony edge of the thorax - you see a sharp visceral pleural line with no vessels beyond it. Expiratory film makes it more visible.
- Pleural effusion: Homogeneous opacity with meniscus (curved upper border), blunting of costophrenic angle.
- Pleural thickening: Old infection, asbestos exposure (calcified plaques).
Anatomical Reference: PA View
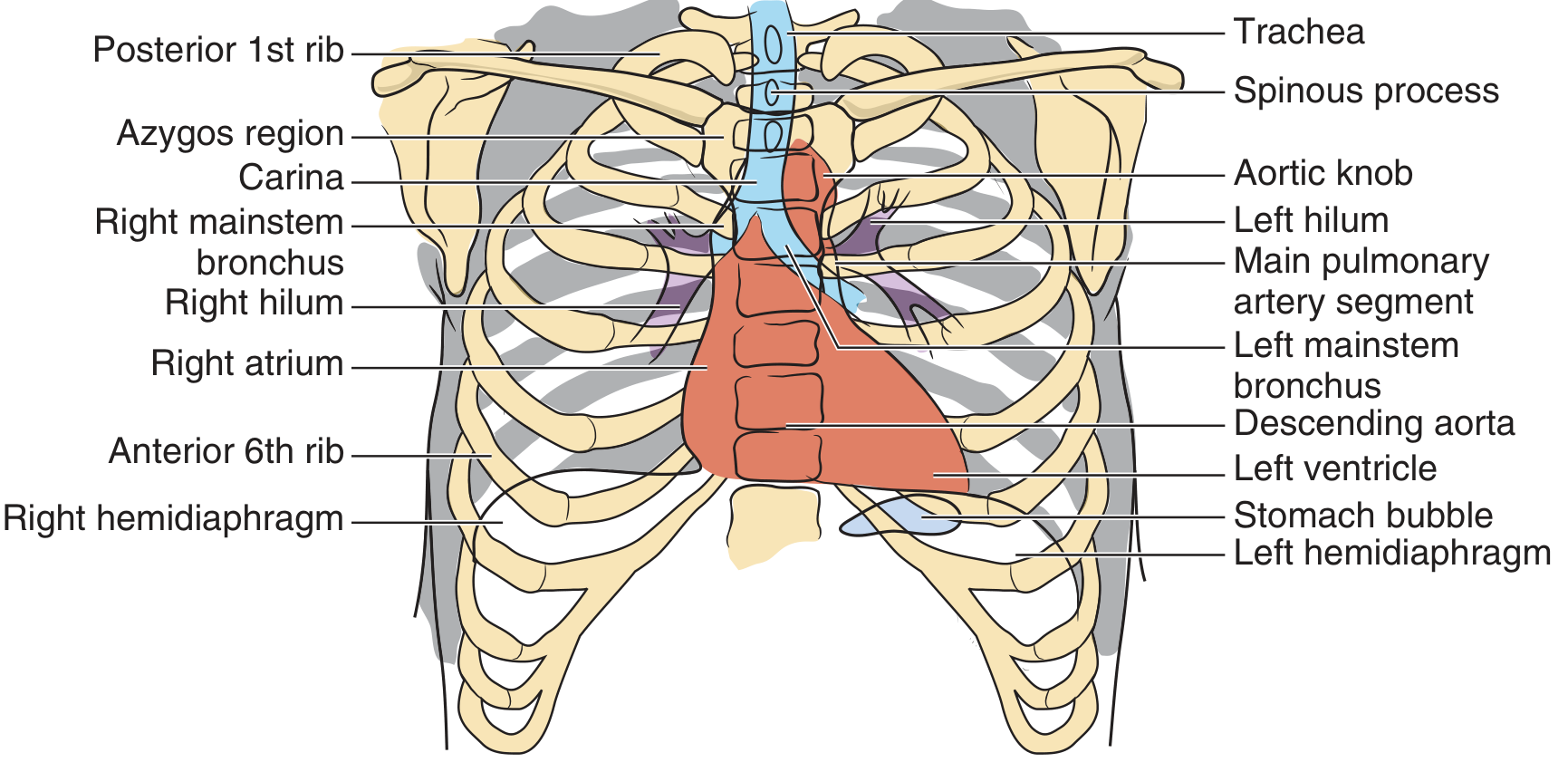
Figure: Schematic anatomy of the posteroanterior chest view - Pfenninger and Fowler's Procedures for Primary Care
Anatomical Reference: Lateral View
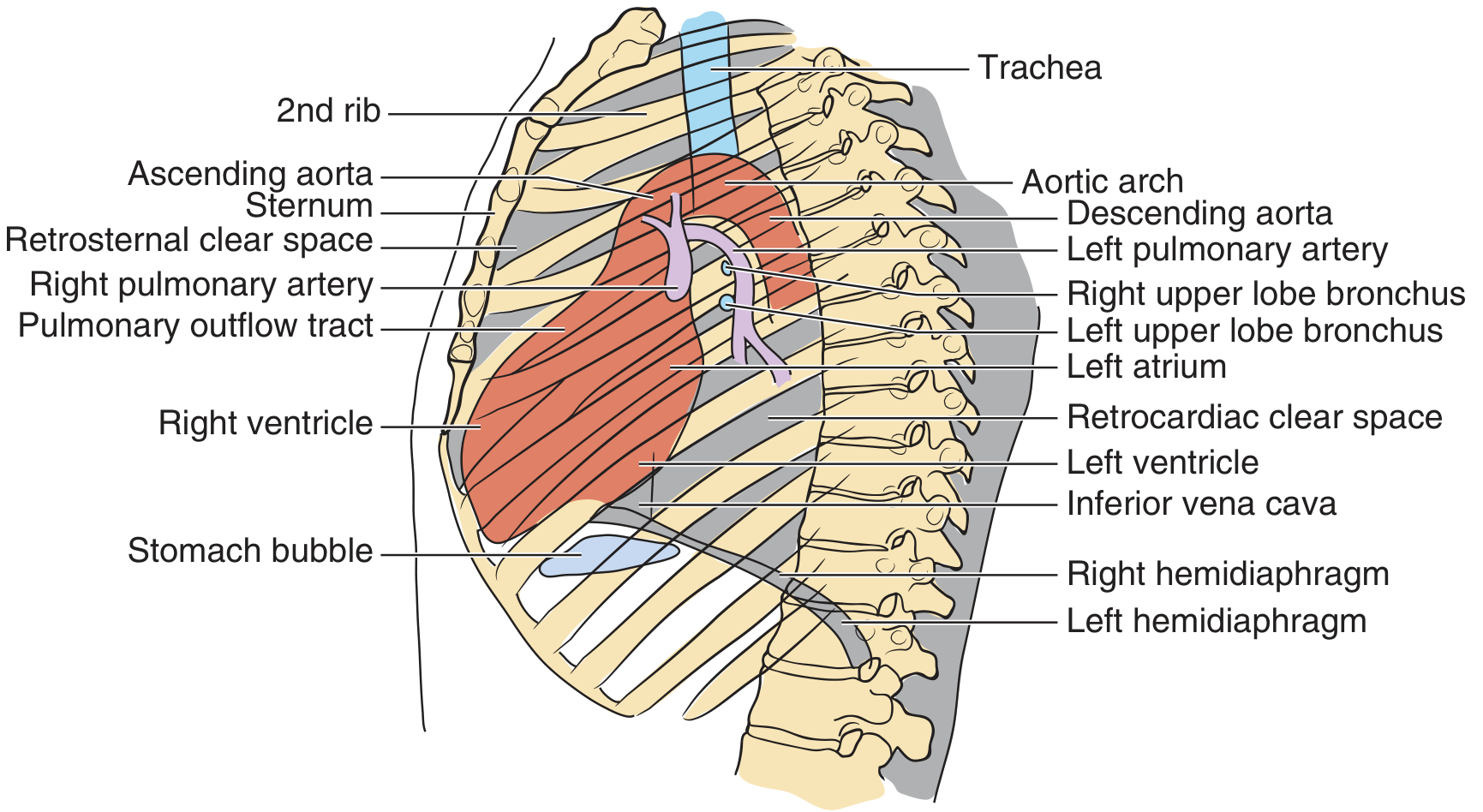
Figure: Landmarks of the lateral chest film - Pfenninger and Fowler's Procedures for Primary Care
Top 10 "Normal" Tips (from textbook)
- Integrate clinical history with the film - never read in isolation.
- Clavicular heads equidistant from spinous processes = no rotation.
- At least 9 posterior ribs visible on PA inspiration.
- Intervertebral spaces should NOT be visible below the diaphragm.
- In children under 5, the thymus is normally large and can simulate mediastinal widening.
- Mediastinum should not exceed 8 cm in adults.
- Left hilum is higher than right hilum.
- Right diaphragm is higher than left diaphragm.
- Lesions >10 mm in diameter benefit from specialist review or CT.
- Subtle hilar or parenchymal changes require clinical correlation.
PART 2: CT SCAN INTERPRETATION
CT produces cross-sectional images by measuring X-ray attenuation through tissues. The key concept is Hounsfield Units (HU) - a scale of tissue density:
| Tissue | HU Range | Appearance |
|---|---|---|
| Air | -1000 | Black |
| Fat | -100 to -50 | Very dark gray |
| Water/fluid | 0 | Gray |
| Soft tissue/muscle | +20 to +80 | Gray |
| Acute blood | +50 to +80 | Bright gray |
| Bone/calcification | +400 to +1000 | White |
CT Windows
Because the human eye cannot distinguish the full HU range simultaneously, radiologists use "windowing" to optimize contrast for specific tissue types:
| Window | Level (Center) | Width | Best For |
|---|---|---|---|
| Lung window | -600 HU | 1500-2000 HU | Lung parenchyma, airways, emphysema, nodules |
| Mediastinal/soft tissue window | +40 HU | 400 HU | Heart, vessels, lymph nodes, soft tissue masses |
| Bone window | +400 HU | 2000 HU | Rib fractures, vertebral lesions, cortical bone |
| Liver window | +60 HU | 150-175 HU | Abdominal organs |
How to Read a Chest CT Systematically
- Confirm patient details and clinical indication on the header.
- Check contrast enhancement: Was IV contrast given? Contrast highlights vessels and enhances lesions. CT pulmonary angiography (CTPA) is used for pulmonary embolism.
- Lung windows - evaluate:
- Lung parenchyma for nodules, masses, ground-glass opacities (GGO), consolidation, cavities, honeycombing, air bronchograms
- Bronchi for thickening, dilation (bronchiectasis)
- Pleural space for effusion, pneumothorax, plaques
- Mediastinal windows - evaluate:
- Heart size and pericardium
- Aorta and great vessels (dissection, aneurysm)
- Lymph nodes: short-axis diameter >10 mm = abnormal in mediastinum
- Esophagus
- Bone windows - evaluate:
- Ribs, sternum, thoracic spine for fractures, metastases, osteoporosis
- Soft tissue windows - check:
- Chest wall masses, subcutaneous emphysema
- Liver dome, upper abdominal structures visible on lower slices
Key CT Chest Patterns
| CT Finding | Description | Significance |
|---|---|---|
| Ground-glass opacity (GGO) | Hazy increased density, vessels still visible | Pneumonia (viral/bacterial), pulmonary edema, early fibrosis, COVID-19 |
| Consolidation | Dense opacity obscuring vessels | Pneumonia, malignancy, hemorrhage |
| Crazy paving | GGO + interlobular septal thickening | Alveolar proteinosis, COVID-19 |
| Honeycombing | Clustered cystic spaces 3-10 mm, thick walls | Usual interstitial pneumonia (UIP), IPF |
| Tree-in-bud | Centrilobular nodules + branching | Bronchiolitis, endobronchial spread of TB |
| Pulmonary embolism | Filling defect in pulmonary artery on CTPA | PE - compare with non-opacified vessels |
| Mediastinal widening | >8 cm, irregular contour | Aortic dissection, lymphoma |
| Pleural effusion | Dependent fluid density, bilateral in CHF | Infection, malignancy, heart failure |
PART 3: MRI INTERPRETATION
MRI uses magnetic fields and radiofrequency pulses to generate images based on hydrogen proton behavior in different tissues. It does not use ionizing radiation.
Core MRI Sequences and Signal Characteristics
Based on Cummings Otolaryngology:
T1-Weighted Images (T1WI)
- Parameters: short TR (500-700 ms), short TE (15-40 ms)
- Quick identification trick: Fat = white (bright), CSF/fluid = black (dark), muscle = intermediate gray
- Bright (hyperintense) on T1: Fat, blood products (subacute blood/methemoglobin), melanin, proteinaceous fluid, gadolinium-enhanced areas
- Dark (hypointense) on T1: Air, cortical bone, rapidly flowing blood, water/CSF, most tumors
- Best for: Anatomical detail, fat vs. non-fat distinction, post-gadolinium enhancement
T2-Weighted Images (T2WI)
- Parameters: long TR (2000-4000 ms), long TE (50-90 ms)
- Quick identification trick: CSF/fluid = white (bright), muscle = dark, fat = intermediate (bright on FSE sequences)
- Bright (hyperintense) on T2: Water/CSF, edema, most tumors, inflammation, cysts, synovial fluid
- Dark (hypointense) on T2: Cortical bone, calcification, air, hemosiderin (old blood), fibrous tissue
- Best for: Detecting pathology, edema, inflammation, cysts, tumor margins
T1 vs T2 - The Quick Reference Table
| Tissue/Structure | T1 Signal | T2 Signal |
|---|---|---|
| Fat | Bright | Bright (FSE)/Intermediate |
| CSF/fluid | Dark | Bright |
| Muscle | Intermediate | Dark |
| Cortical bone | Dark | Dark |
| Acute blood | Dark | Dark |
| Subacute blood | Bright | Bright |
| Old blood/hemosiderin | Dark | Very dark |
| Most tumors | Dark-intermediate | Bright |
| Edema | Dark-intermediate | Bright |
| Air | Dark | Dark |
Gadolinium Contrast Enhancement
- Gadolinium shortens T1 relaxation time, making enhancing tissues appear bright on T1WI.
- Used to highlight: blood-brain barrier breakdown, tumor vascularity, infection/abscess walls, vascular structures.
- Important: gadolinium should be used cautiously in severe renal impairment (risk of nephrogenic systemic fibrosis).
Other Commonly Used MRI Sequences
| Sequence | Purpose |
|---|---|
| FLAIR (Fluid-Attenuated Inversion Recovery) | CSF signal is suppressed (dark); periventricular white matter lesions (MS, edema) become very conspicuous |
| DWI (Diffusion-Weighted Imaging) | Restricted diffusion = acute stroke, abscess, hypercellular tumor (appears bright) |
| STIR (Short Tau Inversion Recovery) | Fat signal suppressed; highlights bone marrow edema, soft tissue edema |
| GRE/Gradient Echo | Sensitive to magnetic susceptibility; detects blood products, calcification, metal artifacts |
| MRA (Magnetic Resonance Angiography) | Vascular anatomy without ionizing radiation |
MRI Artifacts to Know
- Metal artifacts: Implants, dental work, bullets - cause signal void and distortion.
- Motion artifact: Breathing, swallowing, heartbeat cause ghosting/blurring.
- Chemical shift artifact: Fat-water interface - seen as dark/bright lines at organ borders.
- Susceptibility artifact: Exaggerated signal loss at air-tissue interfaces, near blood products or metal.
MRI vs CT in Chest Imaging
| Feature | MRI | CT |
|---|---|---|
| Radiation | None | Yes |
| Speed | Slower (minutes per sequence) | Fast (seconds) |
| Lung parenchyma | Poor (air causes signal loss) | Excellent |
| Cardiac/vascular | Excellent | Good with contrast |
| Soft tissue detail | Superior | Moderate |
| Bone detail | Good (marrow) | Superior (cortex) |
| Main chest indications | Cardiac MRI, mediastinal masses, brachial plexus, chest wall tumors | Pulmonary nodules, PE, lung disease, staging |
Summary: Which Imaging for What?
| Clinical Question | Best Modality |
|---|---|
| Acute chest complaint (first-line) | CXR |
| Pulmonary embolism | CTPA |
| Pulmonary nodule follow-up | CT |
| Interstitial lung disease | High-resolution CT (HRCT) |
| Mediastinal/chest wall mass | MRI or CT with contrast |
| Cardiac function/structure | Cardiac MRI |
| Pleural disease | CT |
| Aortic dissection | CT with contrast |
| Brachial plexus injury | MRI |
| Rib fractures | CT bone window |
Sources:
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed. - Chapter 231: Interpretation of the Chest X-Ray
- Cummings Otolaryngology Head and Neck Surgery - Chapter 8: MRI Pulse Sequences
- Murray & Nadel's Textbook of Respiratory Medicine - CT imaging patterns
This is a shared conversation. Sign in to Orris to start your own chat.