Alveolar ventilation full details for md exams 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive content from Guyton, Costanzo, Murray & Nadel, and other authoritative sources. Let me compile the full MD-exam answer:
Alveolar Ventilation - Complete Notes for MD Examinations (10 Marks)
1. Definition
Alveolar ventilation is the volume of fresh inspired air (non-dead-space gas) that enters the alveoli and adjacent gas exchange areas (alveolar sacs, alveolar ducts, respiratory bronchioles) per minute and is therefore available for gas exchange. It is the most physiologically important component of total ventilation.
- Guyton and Hall Textbook of Medical Physiology, p. 499
2. Key Volumes and Terminology
| Parameter | Normal Value | Description |
|---|---|---|
| Tidal Volume (VT) | 500 mL | Volume per breath |
| Anatomical Dead Space (VD) | ~150 mL | Conducting airways - no gas exchange |
| Alveolar Volume per breath (VA) | ~350 mL | VT - VD |
| Respiratory Rate | 12 breaths/min | Normal resting rate |
| Minute Ventilation (VE) | ~6000 mL/min | VT × Rate |
| Alveolar Ventilation (VA) | ~4200 mL/min | (VT - VD) × Rate |
3. Formula for Alveolar Ventilation Rate
$$\dot{V}_A = \text{Freq} \times (V_T - V_D)$$
With normal values:
$$\dot{V}_A = 12 \times (500 - 150) = 12 \times 350 = \mathbf{4200\ mL/min}$$
- Guyton and Hall, p. 499
4. Dead Space - Types and Significance
Dead space air fills the respiratory passages where no gas exchange occurs. There are two types:
A. Anatomical Dead Space
- Comprises conducting airways: nose, pharynx, larynx, trachea, bronchi, bronchioles
- Normal volume: ~150 mL (approximately 1 mL per pound of ideal body weight)
- Increases with body size, lung size, age (after 50-60 years), and in upright posture
- Women have slightly smaller anatomical dead space than men due to smaller airway size
- Guyton and Hall, p. 499
B. Physiological (Functional) Dead Space
- Anatomical dead space plus alveolar dead space
- Alveolar dead space = alveoli that are ventilated but not perfused (or under-perfused), making their ventilation "wasted"
- In healthy lungs: Physiological dead space ≈ Anatomical dead space (because all alveoli are perfused)
- In disease (e.g., pulmonary embolism, COPD, ARDS): physiological dead space can be 10x anatomical dead space (1-2 liters)
- Guyton and Hall, p. 499
Measurement of Dead Space
Fowler Method (Single-Breath N2 Washout) - measures anatomical dead space:
- Subject inhales one breath of 100% O2 (filling dead space with pure O2)
- On expiration, a nitrogen meter records N2 concentration
- Early expiration: N2 = 0% (pure O2 from dead space)
- Mid-expiration: N2 rises rapidly as alveolar air mixes
- Late expiration: N2 reaches plateau (pure alveolar air ~60%)
$$V_D = \frac{\text{Gray area} \times V_E}{\text{Pink area} + \text{Gray area}}$$
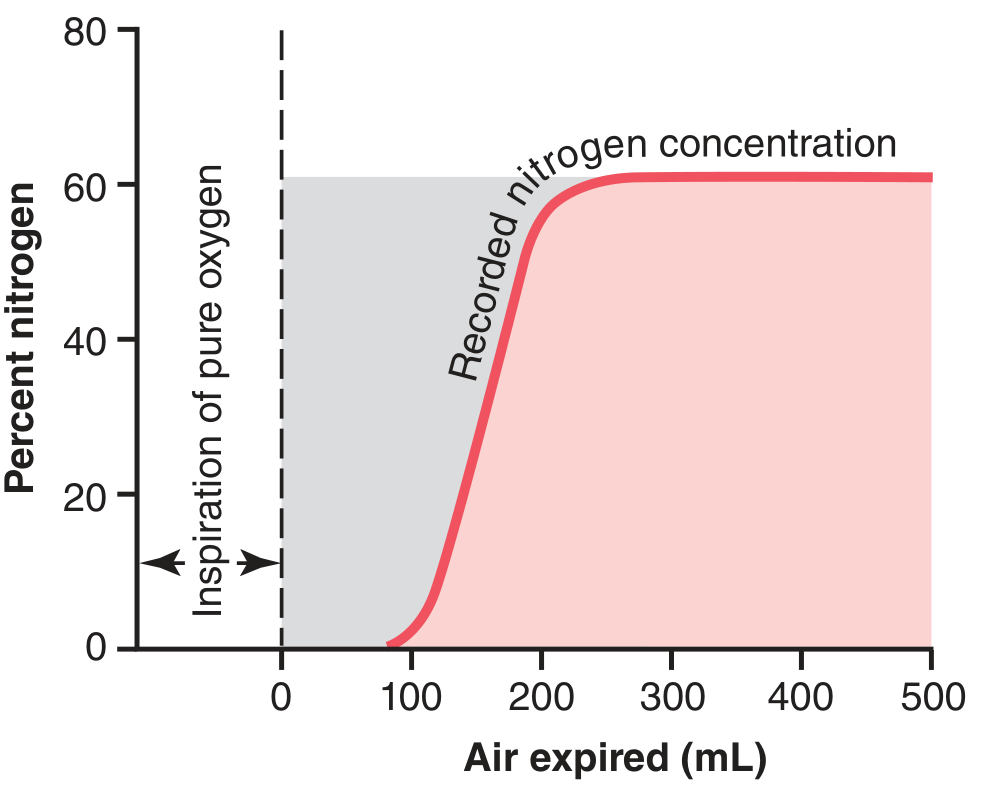
Figure: Changes in nitrogen concentration in expired air after a single inspiration of pure oxygen. The gray area (N2=0) represents dead space volume. - Guyton and Hall
5. The Alveolar Ventilation Equation
This is the fundamental equation of respiratory physiology, expressing the inverse relationship between alveolar ventilation and alveolar PCO2:
$$\boxed{P_{ACO_2} = \frac{\dot{V}_{CO_2} \times K}{\dot{V}_A}}$$
Or rearranged:
$$\dot{V}A = \frac{\dot{V}{CO_2} \times K}{P_{ACO_2}}$$
Where:
- VA = Alveolar ventilation (mL/min or L/min)
- VCO2 = Rate of CO2 production by tissues (~200 mL/min at rest)
- PACO2 = Alveolar PCO2 (normally 40 mmHg)
- K = Constant = 863 mmHg (at BTPS conditions)
Key point: Because CO2 equilibrates completely between alveolar gas and pulmonary capillary blood, PACO2 = PaCO2 (arterial). Therefore arterial PCO2, which is measurable, can substitute for alveolar PCO2:
$$\dot{V}A = \frac{\dot{V}{CO_2} \times 0.863}{P_{aCO_2}}$$
- Costanzo Physiology 7th Edition, p. 201
- Murray & Nadel's Textbook of Respiratory Medicine
6. Hyperbolic Relationship: VA vs PaCO2
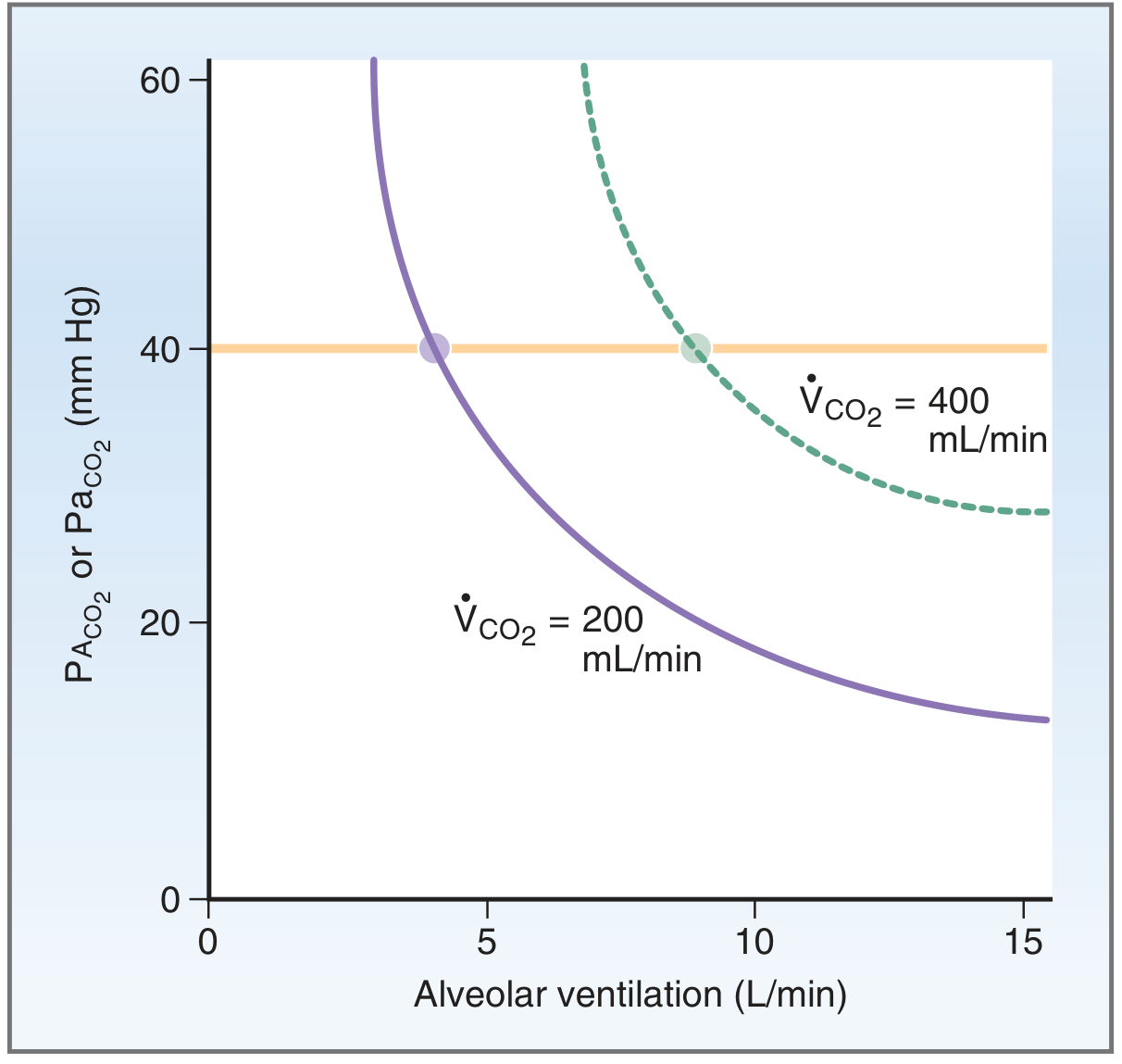
Figure: PACO2/PaCO2 vs alveolar ventilation. Hyperbolic relationship - when CO2 production doubles from 200 to 400 mL/min, alveolar ventilation must also double to maintain PACO2 at 40 mmHg. - Costanzo Physiology
Critical relationships:
- If VA doubles → PACO2 halves (hyperventilation → hypocapnia)
- If VA halves → PACO2 doubles (hypoventilation → hypercapnia)
- If VCO2 doubles and VA also doubles → PACO2 remains constant
7. Alveolar Ventilation vs. Minute Ventilation
$$\text{Minute Ventilation (VE)} = V_T \times \text{Rate} = 500 \times 12 = 6000\ \text{mL/min}$$
$$\text{Alveolar Ventilation (VA)} = (V_T - V_D) \times \text{Rate} = 350 \times 12 = 4200\ \text{mL/min}$$
$$\text{Dead Space Ventilation (VD)} = V_D \times \text{Rate} = 150 \times 12 = 1800\ \text{mL/min}$$
Alveolar ventilation is ~70% of minute ventilation; 30% is wasted as dead space ventilation.
- Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume
8. Effect of Breathing Pattern on Alveolar Ventilation
This is a high-yield exam concept. With a fixed minute ventilation, the pattern of breathing profoundly affects alveolar ventilation:
| Breathing Pattern | VT | Rate | VE | VA |
|---|---|---|---|---|
| Normal | 500 mL | 12/min | 6000 mL/min | 4200 mL/min |
| Rapid shallow | 250 mL | 24/min | 6000 mL/min | 2400 mL/min |
| Slow deep | 1000 mL | 6/min | 6000 mL/min | 5100 mL/min |
Deep slow breathing is more efficient than rapid shallow breathing because dead space ventilation remains fixed at 150 mL per breath regardless of tidal volume. Rapid shallow breathing wastes proportionally more ventilation in dead space.
9. Bohr Equation - Measuring Physiological Dead Space
$$\frac{V_{D_{phys}}}{V_T} = \frac{P_{aCO_2} - P_{\bar{E}CO_2}}{P_{aCO_2}}$$
Where:
- VDphys = physiological dead space
- VT = tidal volume
- PaCO2 = arterial PCO2 (replaces alveolar PCO2)
- PECO2 = mean expired PCO2
Normal VD/VT ratio = <0.3 (30%). In severe lung disease or pulmonary embolism, this can rise to 0.6-0.7.
This is also called the Bohr-Enghoff equation when arterial PCO2 substitutes for alveolar PCO2.
- Guyton and Hall, p. 520; Murray & Nadel's
10. Ventilation-Perfusion (V/Q) Ratio and Alveolar Ventilation
The ideal V/Q ratio = 0.8 (VA = 4.2 L/min; Q = 5 L/min)
| Condition | VA/Q | Effect |
|---|---|---|
| Normal alveolus | ~0.8 | Efficient gas exchange |
| Anatomical dead space | ∞ (ventilated, no perfusion) | Wasted ventilation |
| Physiological dead space | >0.8 | Partially wasted ventilation |
| Physiological shunt | <0.8 | Under-ventilated alveoli |
| True shunt | 0 (perfused, no ventilation) | No gas exchange |
In upright position:
-
Lung apex: V/Q = ~2.5 (over-ventilated relative to perfusion = dead space effect)
-
Lung base: V/Q = ~0.6 (under-ventilated relative to perfusion = shunt effect)
-
Guyton and Hall, p. 520
11. Clinical Significance
Hypoventilation (↓ VA)
- Causes: CNS depression (opioids, sedatives), neuromuscular disease, obesity hypoventilation, COPD
- Effect: ↑ PaCO2 (hypercapnia), ↓ PaO2 (hypoxemia), respiratory acidosis
Hyperventilation (↑ VA)
- Causes: anxiety, pain, fever, metabolic acidosis (Kussmaul breathing), pregnancy
- Effect: ↓ PaCO2 (hypocapnia), ↑ PaO2, respiratory alkalosis, perioral/fingertip tingling
Increased Dead Space (↑ VD)
- Causes: pulmonary embolism, emphysema, positive pressure ventilation, pulmonary hypertension
- Even with normal minute ventilation, effective alveolar ventilation decreases
- Compensated by ↑ minute ventilation (tachypnea and/or increased tidal volume)
12. Summary Table - Normal Values
| Parameter | Normal Value |
|---|---|
| Tidal volume (VT) | 500 mL |
| Anatomical dead space (VD) | 150 mL (~1 mL/lb ideal body weight) |
| Respiratory rate | 12 breaths/min |
| Minute ventilation (VE) | ~6000 mL/min |
| Alveolar ventilation (VA) | ~4200 mL/min |
| VD/VT ratio | <0.3 |
| Alveolar PCO2 / PaCO2 | 40 mmHg |
| Alveolar PO2 (PAO2) | ~100 mmHg |
| VCO2 (CO2 production) | ~200 mL/min |
Exam-Focused Key Points to Remember
- VA = (VT - VD) × Rate - this is the core formula
- VA is the only ventilation that matters for gas exchange; minute ventilation is not a reliable index of alveolar ventilation
- PaCO2 is the best clinical indicator of adequacy of alveolar ventilation - normal PaCO2 = 40 mmHg (35-45 mmHg)
- Inverse relationship: if VA doubles, PaCO2 halves; if VA halves, PaCO2 doubles
- Physiological dead space = anatomical + alveolar dead space; measured by Bohr equation
- Slow deep breathing is more effective than rapid shallow breathing for the same minute ventilation
- Alveolar ventilation equation: PACO2 = (VCO2 × 863) / VA
- In disease, VD/VT can rise to 0.6-0.7, meaning only 30-40% of each breath reaches functioning alveoli
Sources: Guyton and Hall Textbook of Medical Physiology (p. 499-520), Costanzo Physiology 7th Ed. (p. 200-201), Murray & Nadel's Textbook of Respiratory Medicine, Miller's Anesthesia 10e
This is a shared conversation. Sign in to Orris to start your own chat.