What is anatomy?
Anatomy is the branch of biology and medicine concerned with the structure of living organisms. In medicine, it focuses on the human body - studying the form, position, and relationships of body parts including organs, tissues, bones, muscles, nerves, and blood vessels.
There are several major subdivisions:
- Gross (macroscopic) anatomy - structures visible to the naked eye
- Microscopic anatomy (histology) - tissues and cells examined under a microscope
- Developmental anatomy (embryology) - how structures form from conception onward
- Neuroanatomy - the nervous system specifically
- Regional anatomy - studying all structures in a given body region (e.g. the thorax)
- Systemic anatomy - studying body systems (e.g. the cardiovascular system) as a whole
Anatomy is one of the oldest medical sciences, with roots going back to ancient Greece (Hippocrates, Galen) and major advances during the Renaissance (notably Andreas Vesalius, who published De humani corporis fabrica in 1543). It forms the foundation for nearly all clinical medicine - you cannot understand disease or perform surgery without knowing normal structure first.
The study of anatomy uses several approaches: cadaveric dissection, medical imaging (X-ray, CT, MRI), endoscopy, and histological staining of tissue samples.
Diaphragm
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough overview of the diaphragm anatomy, drawn from Fischer's Mastery of Surgery and Gray's Anatomy for Students:
The Diaphragm
Overview
The diaphragm is a dome-shaped musculotendinous structure that seals the inferior thoracic aperture, separating the thoracic and abdominal cavities. Muscle fibers arise radially from the margins of the inferior thoracic aperture and converge centrally into a large central tendon. Because of the oblique angle of the inferior thoracic aperture, the posterior attachment sits lower than the anterior one.
The diaphragm bulges superiorly on both sides to form two domes. The right dome is higher (reaching as far as rib V) because the liver lies beneath it. The left dome is slightly lower.
Origin (Three Parts)
| Part | Origin |
|---|---|
| Sternal | Posterior aspect of the xiphoid process and aponeurosis of transversus abdominis |
| Costal | Inner aspect of costal cartilages/ribs 7-12 |
| Lumbar | Right crus: L1-L3/4 vertebrae; Left crus: L1-L2/3 vertebrae, blending with the anterior longitudinal ligament |
The two crura are joined at the midline by the median arcuate ligament. Two additional arch-shaped ligaments complete the posterior attachment:
- Medial arcuate ligament - from the body of L2 to its transverse process (over psoas major)
- Lateral arcuate ligament - from the transverse process of L2 to the tip of rib 12 (over quadratus lumborum)
Insertion: All fibers converge into the central tendon.
Openings (Apertures)
Three major structures pass through or around the diaphragm:
| Opening | Vertebral Level | Structures Passing Through |
|---|---|---|
| Caval opening | T8 | Inferior vena cava, right phrenic nerve, lymphatic vessels |
| Esophageal hiatus | T10 | Esophagus, anterior & posterior vagal trunks, left gastric artery & vein |
| Aortic hiatus | T12 | Aorta, thoracic duct, (sometimes azygos vein) |
Memory aid: "I 8 (ate) 10 eggs At 12" - IVC at T8, Esophagus at T10, Aorta at T12.
Note: The aorta passes posterior to (not through) the diaphragm, behind the median arcuate ligament.
Also present:
- Foramen of Morgagni (sternocostal hiatus) - between sternal and costal parts; transmits lymphatic vessels from liver to anterior phrenic nodes
- Lumbocostal trigone (Bochdalek triangle) - a muscular deficiency between costal and lumbar parts; a common site of congenital diaphragmatic hernia
Blood Supply
| Surface | Arteries | Venous Drainage |
|---|---|---|
| Superior | Superior phrenic aa., pericardiophrenic & musculophrenic aa. (from internal thoracic) | Pericardiophrenic & musculophrenic vv. → IVC |
| Inferior | Inferior phrenic aa. (from abdominal aorta/celiac trunk) | Inferior phrenic vv. → IVC and left suprarenal vein |
Innervation
- Motor + central sensory: Phrenic nerves (C3, C4, C5 - "C3, 4, 5 keeps the diaphragm alive")
- The phrenic nerves course along the lateral surface of the fibrous pericardium, anterior to the lung roots, reaching the thoracic surface of the diaphragm
- Each phrenic nerve divides into: sternal branch (anteromedial), anterolateral branch, and posterior branch (splits into posterolateral and crural)
- Peripheral sensory: Lower intercostal nerves (T5-T11) and subcostal nerve supply the peripheral diaphragm
Function
- Primary muscle of respiration. On contraction, the domes flatten, increasing thoracic volume and drawing air into the lungs (inspiration). Relaxation allows the domes to rise, decreasing thoracic volume (expiration).
- Also assists with defecation, micturition, vomiting, and parturition (increasing intra-abdominal pressure).
Clinical Relevance
- Hiatal hernia - herniation through the esophageal hiatus (sliding type most common; paraesophageal type less common). See diagram above, panel B.
- Congenital diaphragmatic hernia (CDH) - most often through the Bochdalek triangle (posterolateral), causing bowel herniation into the thorax and pulmonary hypoplasia.
- Referred pain - diaphragmatic irritation (e.g., subphrenic abscess) refers pain to the shoulder tip via the phrenic nerve (C3-C5 dermatome).
- Phrenic nerve palsy - causes ipsilateral hemidiaphragm paralysis and elevation, visible on chest X-ray.
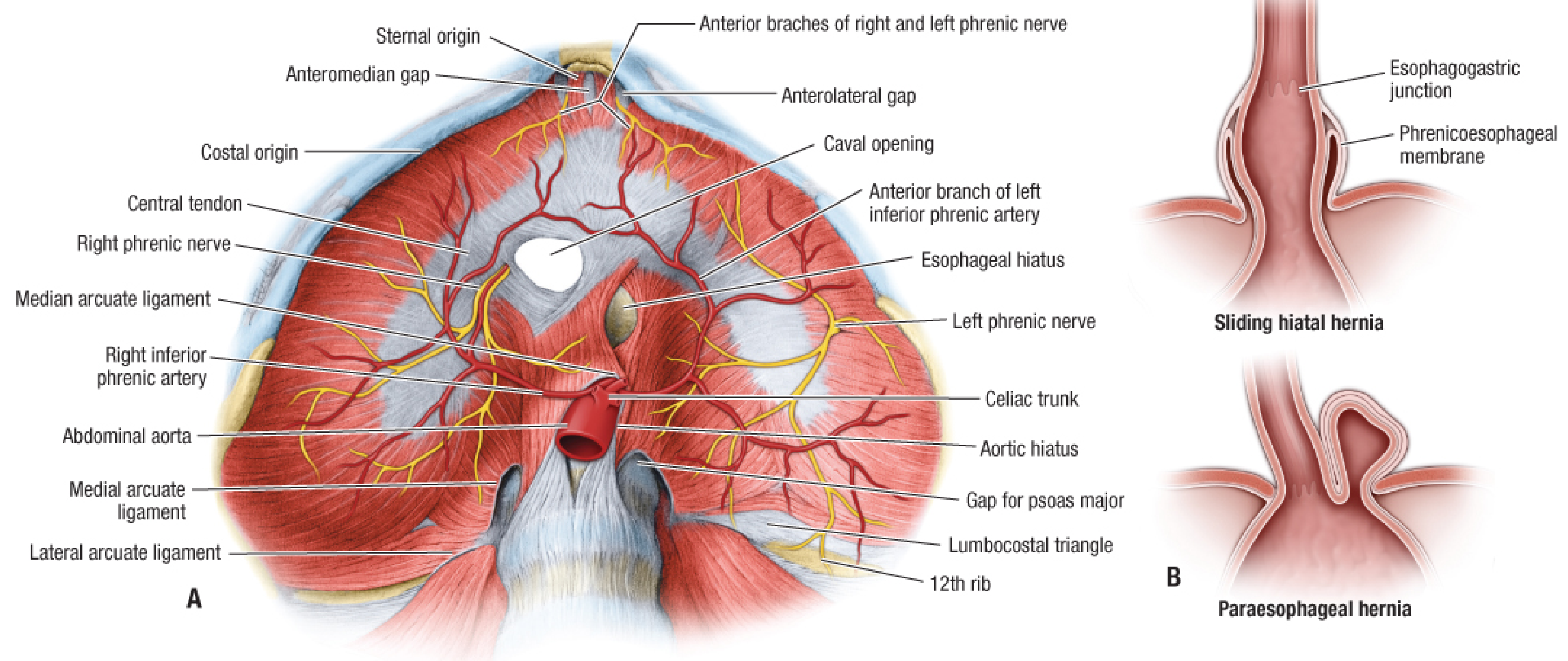
Inferior view of the diaphragm (A) and types of hiatal hernia (B) - Fischer's Mastery of Surgery
- Gray's Anatomy for Students, p. 164
- Fischer's Mastery of Surgery (8th ed.), p. 2588-2590
Mid inguinal point and mid point of inguinal ligament
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the information needed. Note there is an important discrepancy in the textbooks (one source defines mid-inguinal point differently), which is worth highlighting.
Mid-Inguinal Point vs. Midpoint of the Inguinal Ligament
These two landmarks are frequently confused in clinical practice. Here is the clear distinction:
Midpoint of the Inguinal Ligament
- Definition: Midpoint between the Anterior Superior Iliac Spine (ASIS) and the Pubic Tubercle
- The inguinal ligament itself runs from the ASIS to the pubic tubercle, so this is simply its geometric midpoint
- Structure lying here: The femoral artery - it reliably bisects the inguinal ligament at its midpoint
- Also used as the landmark for locating the femoral nerve (just lateral to femoral artery) and femoral vein (just medial)
"Femoral artery reliably bisects the inguinal ligament at its midpoint." - Fischer's Mastery of Surgery, 8th ed.
"Locate the midpoint of a straight line between the anterior superior iliac spine and pubic tubercle... insert the needle vertically [for femoral artery cannulation]." - Color Atlas of Human Anatomy
Mid-Inguinal Point
- Definition: Midpoint between the ASIS and the Pubic Symphysis (not the pubic tubercle)
- Structure lying here: The femoral pulse / deep inguinal ring (approximately ½ inch above this point)
- The deep inguinal ring, where an indirect inguinal hernia originates, lies about 1.25 cm (½ inch) above and lateral to the mid-inguinal point
"½ inch above the mid-inguinal point, which is the midpoint between anterior superior iliac spine and symphysis pubis." - S. Das Manual on Clinical Surgery, 13th ed.
Side-by-Side Comparison
| Feature | Midpoint of Inguinal Ligament | Mid-Inguinal Point |
|---|---|---|
| Between | ASIS and Pubic Tubercle | ASIS and Pubic Symphysis |
| Structure at this point | Femoral artery | Deep inguinal ring (~1.25 cm above) |
| Clinical use | Femoral pulse palpation, arterial cannulation, femoral nerve block | Locating deep inguinal ring, hernia assessment |
Why the Confusion?
The pubic tubercle and pubic symphysis are close together but distinct. The pubic tubercle is a small projection on the upper surface of the pubic bone, about 1.5 cm lateral to the pubic symphysis. This small difference shifts the midpoint enough to place it over a different structure:
- Midpoint of inguinal ligament (ASIS to pubic tubercle) = over the femoral artery
- Mid-inguinal point (ASIS to pubic symphysis) = slightly medial, over the femoral canal/deep ring region
Note: Some older texts (including some editions of Mulholland's Surgery) use the term "mid-inguinal point" loosely to mean midpoint of the inguinal ligament. Always clarify which definition is being used in context.
Mnemonic
"MidLigament = Artery; MidInguinal = deep ring"
- Ligament midpoint → Femoral Artery (L for Ligament, A for Artery)
- Mid-Inguinal point → Deep Inguinal ring (both start with I)
- S. Das Manual on Clinical Surgery, 13th ed., p. 604
- Fischer's Mastery of Surgery, 8th ed., p. 6469
- Color Atlas of Human Anatomy, p. 582
Abduction
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Now I have everything needed for a thorough answer.
Abduction
Definition
Abduction is movement of a limb or body part away from the midline of the body, occurring in the coronal (frontal) plane around an anteroposterior axis. It is the opposite of adduction (movement toward the midline).
Special cases:
- For fingers and toes, abduction means spreading them away from the middle digit (middle finger for the hand; second toe for the foot), not away from the body midline
- For the thumb, abduction is movement anteriorly (away from the palm plane), which is a special case due to the thumb's rotated orientation
Plane and Axis
| Feature | Abduction |
|---|---|
| Plane | Coronal (frontal) plane |
| Axis | Anteroposterior (sagittal) axis |
| Direction | Away from midline |
| Opposite | Adduction |
Abduction at Different Joints
| Joint | Range of Abduction | Key Muscles |
|---|---|---|
| Shoulder (glenohumeral) | 0-180° (with scapular rotation) | Deltoid (middle), Supraspinatus (initiates 0-15°) |
| Hip | 0-45° | Gluteus medius, Gluteus minimus, Tensor fasciae latae |
| Wrist | Radial deviation (~15-20°) | Flexor carpi radialis, Extensor carpi radialis |
| Fingers (MCP joints) | Spread apart from middle finger | Dorsal interossei (DAB), Abductor digiti minimi |
| Thumb (CMC joint) | Anterior abduction | Abductor pollicis brevis, Abductor pollicis longus |
| Toes | Spread apart from 2nd toe | Dorsal interossei, Abductor hallucis, Abductor digiti minimi |
Mnemonic for hand interossei: DAB = Dorsal interossei ABduct; PAD = Palmar interossei ADduct
Abduction of the Femur - Two Scenarios
An important anatomical concept is that abduction can work in two ways depending on which segment is fixed:
- Abduction of femur on a fixed pelvis - the leg swings outward (walking, standing on one leg)
- Abduction of pelvis on a fixed femur - the pelvis tilts laterally, as in single-leg stance during gait; this is what the gluteus medius and minimus do to prevent the pelvis from dropping (Trendelenburg mechanism)
Shoulder Abduction - Special Note
Full shoulder abduction to 180° is achieved in two phases:
- 0-90° - glenohumeral joint abduction (supraspinatus initiates; deltoid continues)
- 90-180° - requires upward rotation of the scapula (serratus anterior + trapezius), plus lateral rotation of the humerus to clear the greater tubercle from under the acromion
The painful arc (60-120°) during abduction suggests supraspinatus pathology or subacromial impingement.
Circumduction
When abduction is combined sequentially with flexion, adduction, and extension, the resulting circular movement is called circumduction - the limb traces a cone shape. This is possible at ball-and-socket joints (hip, shoulder) and saddle joints (thumb CMC).
Clinical Relevance
| Condition | Abduction Finding |
|---|---|
| Trendelenburg gait | Weak hip abductors (gluteus medius) - pelvis drops to opposite side during swing phase |
| Supraspinatus tear | Inability to initiate shoulder abduction (0-15°) |
| Superior gluteal nerve injury | Paralysis of gluteus medius/minimus - positive Trendelenburg sign |
| Abduction contracture of hip | Fixed abduction deformity, seen in post-polio or after hip surgery |
| Erb's palsy (C5-C6) | Loss of shoulder abduction - "waiter's tip" posture |
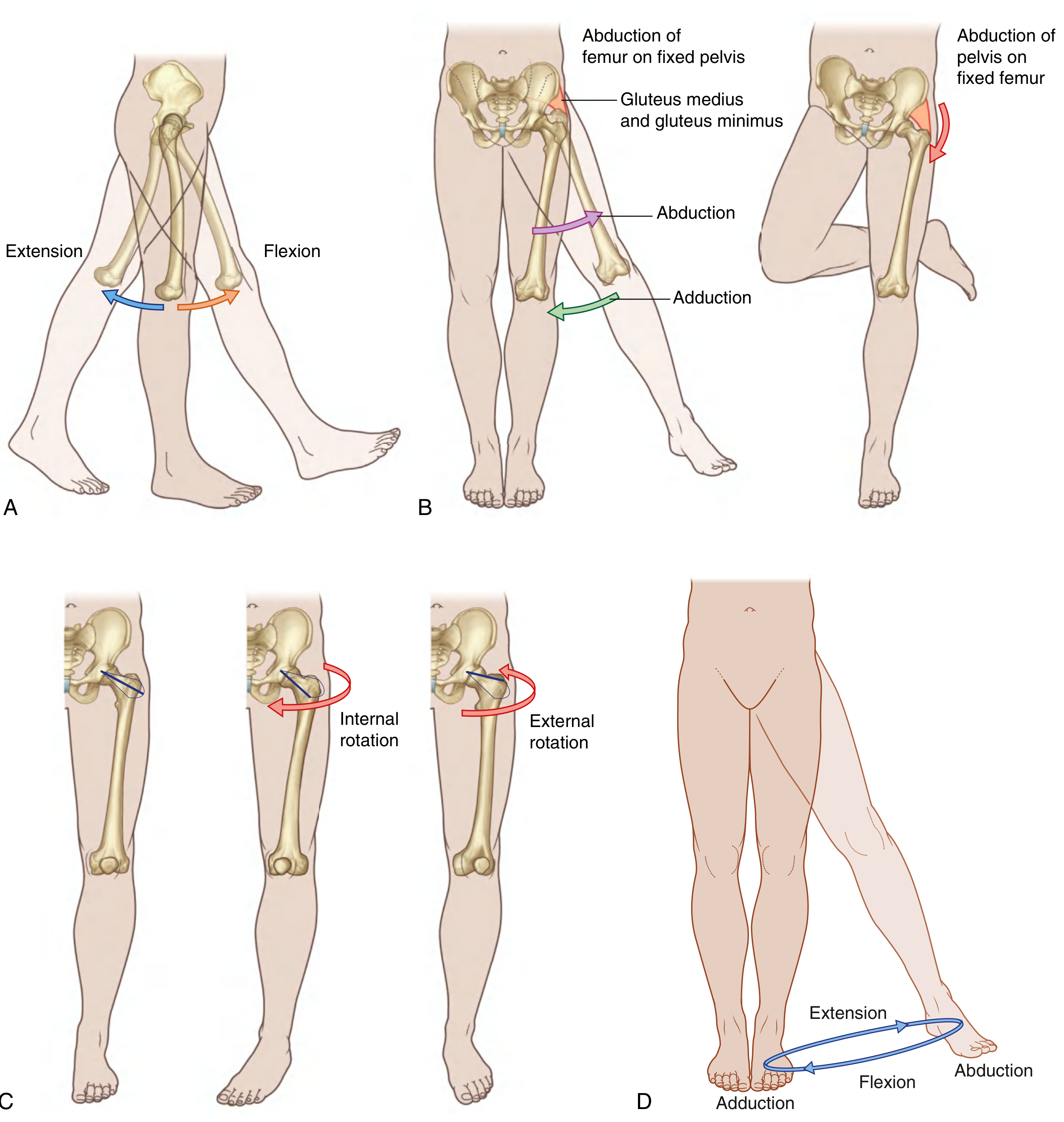
Movements of the hip joint showing abduction and adduction - Gray's Anatomy for Students
- Gray's Anatomy for Students, p. 640-641
This is a shared conversation. Sign in to Orris to start your own chat.