Placental lakes
Reading File
Finding Sources
Finding Sources
Searching PubMed
"placental lakes" ultrasound
Finding Sources
Finding Sources
Searching PubMed
"placental lakes" clinical significance
Reading File
Reading Article
PMID: 37592837
Reading File
Loading Image
Loading Image
Here is a thorough summary of placental lakes based on authoritative textbook content and the most recent review literature.
Placental Lakes
Definition
Placental lakes are enlarged intervillous vascular spaces containing maternal blood. They appear as anechoic (echo-free) areas within the placental parenchyma on ultrasound. They are distinct from placental cysts (fluid-filled blebs near the fetal surface) and from placental lacunae (seen in placenta accreta spectrum).
- Creasy & Resnik's Maternal-Fetal Medicine, p. 608
Incidence
Placental lakes are seen in ~20% of second-trimester ultrasound examinations - making them a common finding in routine obstetric scanning.
Pathophysiology
Lakes represent villous-free areas within the placental parenchyma filled with maternal blood of varying velocities. They arise from the intervillous space, where maternal blood circulates around the chorionic villi. Larger lakes tend to form in areas of lower villous density - under the fetal plate or in marginal areas - but can also occur in the center of a lobule above the entry of a spiral artery.
They typically begin appearing once maternal blood starts flowing freely within the intervillous space (late first trimester onward).
Ultrasound Appearance (Key Diagnostic Features)
- Anechoic (echo-free) spaces scattered within the placental substance
- Variable size and location on serial examinations - they can change shape, enlarge, shrink, or fully resolve
- May completely resolve before delivery
- On color Doppler: no arterial flow detected within the lake, but slow, swirling venous flow is visible on real-time scanning - this is the key distinguishing feature
Figure 27.22 - Placental echolucencies at 19 weeks:
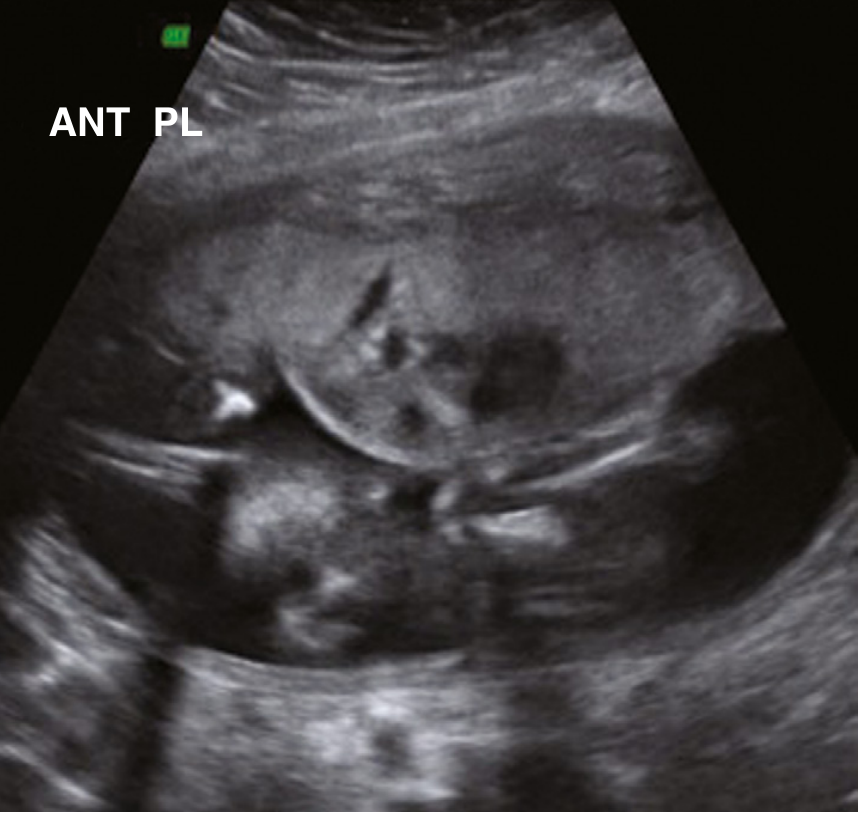
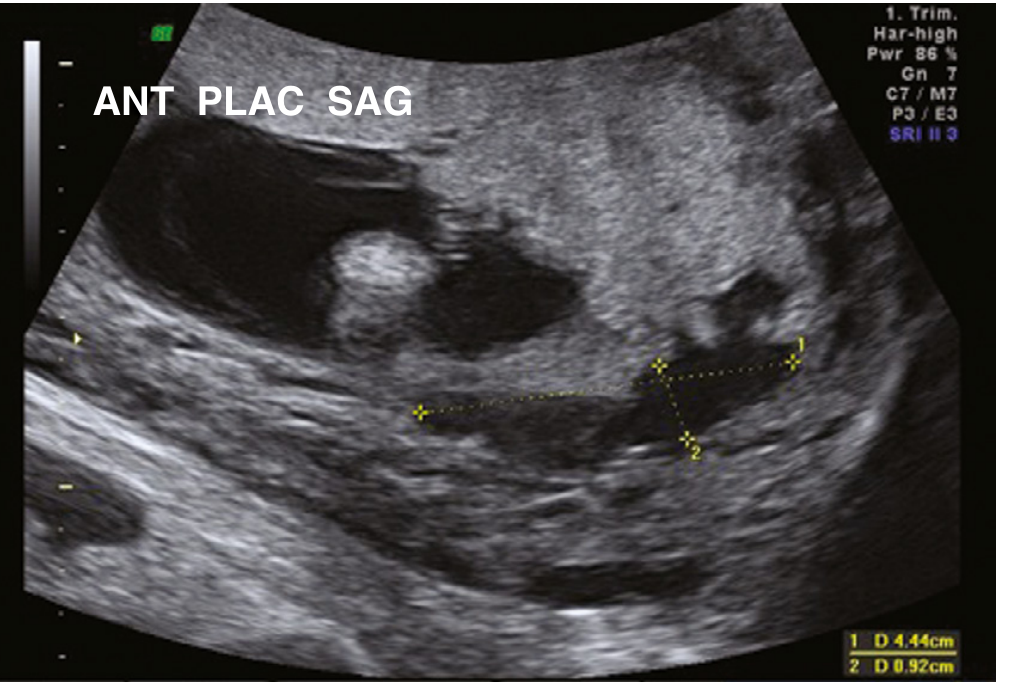
Figure 27.21 - Extensive placental echolucencies at 12 weeks (resolved by 18 weeks):
Clinical Significance
Placental lakes - by themselves - are of no clinical significance. The older teaching that numerous lakes indicated placental insufficiency or fetal growth restriction (FGR) is not supported by recent data.
The exception: if a lake transforms into an echogenic cystic lesion, this has been associated with poor fetal growth and placental malperfusion.
Lakes vs. Lacunae - An Important Distinction
A 2024 review (Jauniaux et al., Ultrasound Obstet Gynecol) clarifies this frequently confused distinction:
| Feature | Placental Lakes | Placental Lacunae |
|---|---|---|
| Timing | Appear from late 1st trimester | Develop progressively in 2nd trimester |
| Location | Any area of placenta | Within a uterine scar |
| Doppler | No arterial flow; slow venous swirl | High-velocity, high-volume arterial flow from radial/arcuate arteries |
| Clinical relevance | Generally benign | Associated with placenta accreta spectrum |
| Shape change | Variable, can resolve | Progressive growth as pregnancy advances |
Both can coexist in the same placenta. The key differentiator is Doppler - lacunae show turbulent arterial inflow, which should prompt evaluation for placenta accreta spectrum (PAS).
Differential Diagnosis
When anechoic/hypoechoic areas are found in the placenta, the differential includes:
- Placental lakes (most common, benign)
- Placental cysts
- Placental lacunae (accreta spectrum)
- Chorangioma (has internal arterial flow on Doppler)
- Uterine fibroid (adjacent to placenta)
- Subchorionic hematoma / placental abruption (can mimic lakes)
Management
- No follow-up is required for placental lakes
- Routine obstetric management applies
- No additional fetal surveillance is needed unless associated features suggest another pathology (e.g., echogenic change within the lake, growth restriction on serial scans)
Prognosis
Excellent. Isolated placental lakes carry no additional perinatal risk. They frequently resolve before delivery.
Summary: Placental lakes are a common, benign ultrasound finding representing enlarged intervillous spaces with slow venous maternal blood flow. The key management point is to distinguish them from placental lacunae (which signal possible accreta spectrum) using color Doppler - lakes have no arterial flow, lacunae do.
This is a shared conversation. Sign in to Orris to start your own chat.