Pulled elbow anatomy and x ray findings
Reading File
Finding Sources
Searching the Web
pulled elbow nursemaid elbow anatomy x-ray findings radiology
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive textbook content and high-quality anatomical images. Let me compile a thorough answer.
Pulled Elbow (Nursemaid's Elbow / Radial Head Subluxation)
Definition & Epidemiology
Pulled elbow is a radial head subluxation caused by sudden longitudinal traction on a child's extended, pronated forearm. It is the most common elbow injury in children under 5, accounting for >20% of all upper extremity injuries in this age group.
- Peak age: 2-3 years (range: 6 months to ~6 years)
- Sex: Girls slightly more affected than boys
- Side: Left arm more commonly than right
- By age 5, the annular ligament thickens and strengthens, making the injury much less common
- Rosen's Emergency Medicine, p. 639 | Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 1151
Anatomy
The elbow has three articulations relevant here:
- Radiocapitellar joint - between the radial head and the capitellum of the humerus (this is the joint involved in pulled elbow)
- Proximal radioulnar joint - the radial head sits within the radial notch of the ulna
- Humeroulnar joint
The annular ligament is a strong fibrous band that encircles the radial head like a cuff, anchoring it to the anterior and posterior margins of the radial notch of the ulna. Its proximal attachment to the radial neck periosteum is relatively loose in young children.
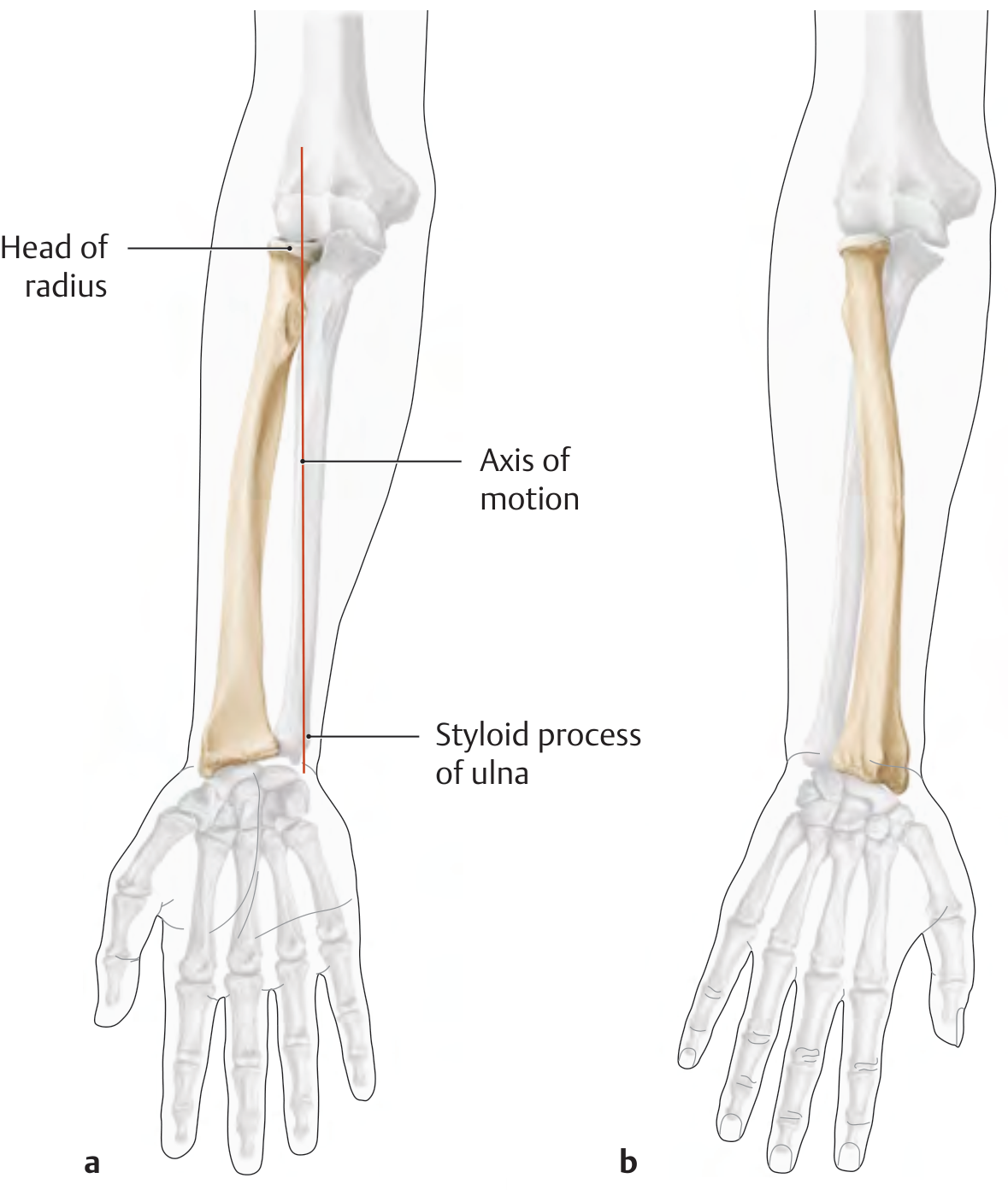
THIEME Atlas of Anatomy - showing the axis of pronation/supination through the radial head
Mechanism & Pathology
The classic mechanism is axial traction on the extended, pronated forearm - e.g., a toddler pulled up by the wrist or yanked back from running into traffic.
What happens step-by-step:
- Sudden longitudinal traction is applied with the elbow extended and wrist pronated
- The radial head moves distally, away from the capitellum
- The annular ligament tears at its periosteal attachment to the radial neck
- When traction is released, the detached flap of annular ligament slips proximally and becomes trapped between the radial head and the capitellum
- The arm snaps back but with the ligament now interposed in the radiocapitellar joint
Other mechanisms include rolling over in bed (infants <6 months) and direct trauma/twisting.
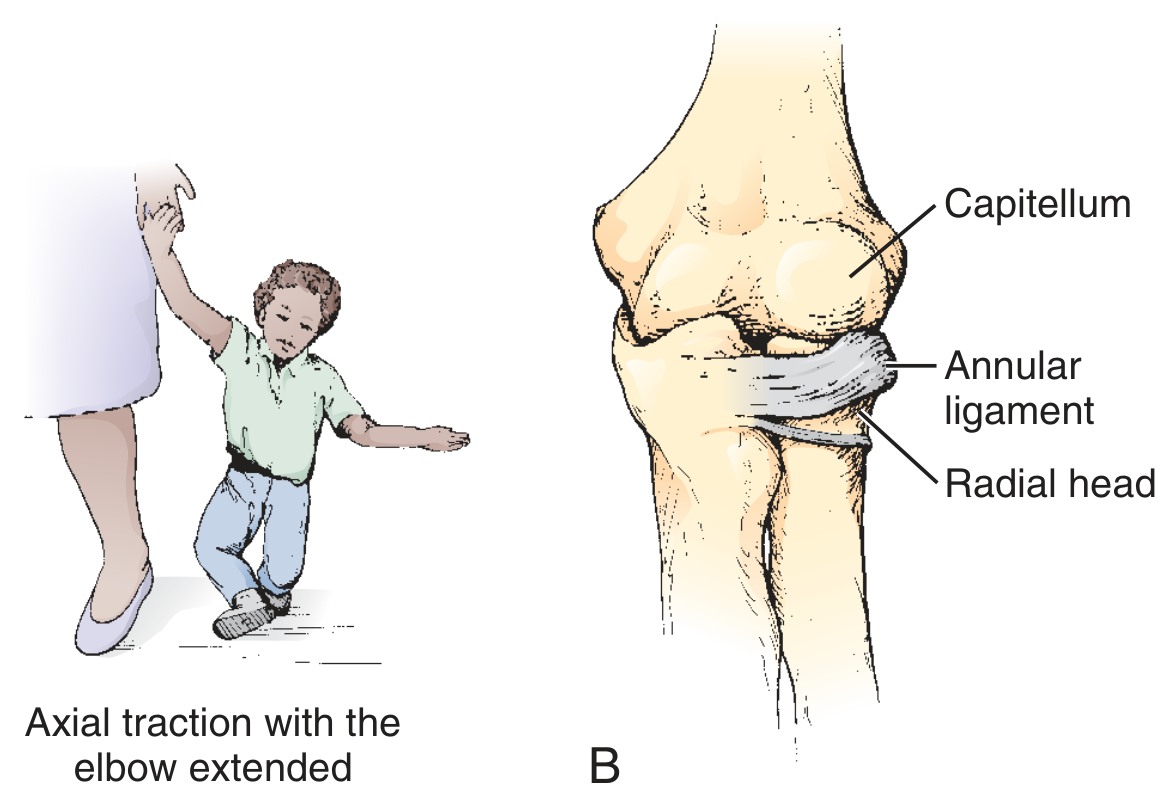
Roberts & Hedges' Clinical Procedures in Emergency Medicine - mechanism (left) and pathologic lesion with annular ligament trapped between radial head and capitellum (right)
- Roberts & Hedges', p. 1151
Clinical Features
| Feature | Detail |
|---|---|
| Arm position | Held slightly flexed, wrist pronated ("nursemaid's position") - hangs at side |
| Pain | Minimal at rest; child refuses to use arm |
| Refusal | Will not supinate or extend elbow |
| Tenderness | Localised over radial head on direct palpation |
| Swelling/bruising | Generally absent |
| Deformity | Absent |
An older child may point to the dorsal distal forearm (not the elbow), which can mislead the clinician toward suspecting a distal radial buckle fracture.
- Rosen's Emergency Medicine, p. 639
X-Ray Findings
This is a key examination point:
X-rays are typically NORMAL in pulled elbow.
The annular ligament is a soft tissue structure and is not visible on plain radiographs. The radial head subluxation is usually subtle and reduces spontaneously or during positioning.
When to X-ray:
- Swelling or deformity is present
- Uncharacteristic history / concern for non-accidental trauma
- Tenderness over the humerus, distal radius, or wrist (not just the elbow)
- Child does not regain arm use after reduction
What to look for on X-ray (if taken):
| Finding | Significance |
|---|---|
| Normal alignment | Most common finding - does not rule out pulled elbow |
| Radiocapitellar line | A line along the radial shaft axis should bisect the capitellum on all views; misalignment suggests subluxation |
| Anterior fat pad sign | May be elevated if there is joint effusion (a subtle clue) |
| No fracture | Main role of X-ray is to exclude occult fracture, not to confirm pulled elbow |
On MRI (if performed - rarely needed), findings include:
- Proximal displacement of the annular ligament
- Diffuse thickening of the annular ligament at the radiocapitellar joint
- Pericapsular edema
The X-ray is sometimes "self-correcting" - positioning the arm in supination for a true lateral view can spontaneously reduce the subluxation during the exam. - Radiology Assistant
Reduction Technique
Two established methods:
1. Hyperpronation (preferred - higher first-attempt success rate):
- Support elbow; grip distal forearm
- Firmly hyperponate the forearm with moderate pressure over radial head
- A palpable/audible "click" confirms reduction
2. Supination-Flexion (traditional):
- Supinate the forearm while applying thumb pressure over radial head
- Then flex the elbow in one continuous motion
- Click felt as radial head reduces
After successful reduction, 90% of children regain use within 30 minutes. No immobilisation is required.
Recurrence rate: ~20%; uncommon after age 5 as ligament matures.
- Rosen's Emergency Medicine, p. 639-640 | Miller's Review of Orthopaedics 9th Ed, p. 940
Summary Table
| Feature | Detail |
|---|---|
| Joint involved | Radiocapitellar |
| Pathology | Annular ligament tear + interposition between radial head and capitellum |
| Classic mechanism | Axial traction, pronated wrist, extended elbow |
| Peak age | 2-3 years |
| X-ray | Normal (main use: exclude fracture) |
| Radiocapitellar line | Should bisect capitellum on all views; disruption = subluxation |
| Reduction | Hyperpronation (first-line) or supination-flexion |
| Immobilisation | Not required |
Complications of pulled elbow
Finding Sources
Finding Sources
Searching the Web
pulled elbow nursemaid's elbow complications recurrence chronic subluxation
Reading File
Finding Sources
Reading File
Reading File
Reading File
I have comprehensive content. Let me now compile the full answer on complications.
Complications of Pulled Elbow
Overall, pulled elbow carries an excellent prognosis with very few serious complications. Most children regain full arm function within minutes to 30 minutes of reduction. However, several complications are recognised:
1. Recurrence (Most Common Complication)
- Rate: ~20% overall; up to one-third of children experience at least one recurrence
- Recurrence is especially common in the weeks immediately following the first episode
- Risk is highest in children under 5; declines sharply after age 5 as the annular ligament matures and thickens
- Recurrence usually resolves spontaneously around age 5 when the ligamentous structures about the elbow mature
- Parents should be counselled to avoid axial traction on the child's arm - no lifting by the wrist/hand, no swinging by the arms
- After multiple recurrences, parents may be taught to perform the reduction maneuver at home
- Campbell's Operative Orthopaedics 15th Ed | Miller's Review of Orthopaedics 9th Ed | StatPearls
2. Reduction Failure / Delayed Reduction
- A click is not always felt during reduction; up to 30% of patients require two or more attempts before a successful click is produced
- If no click is detected and the child does not use the arm within 30 minutes, repeat reduction attempts are recommended
- Children seen several hours after the injury may be more difficult to reduce due to soft tissue swelling and muscle spasm around the joint; oral/nasal midazolam can be a useful adjunct in this scenario
- 6 out of 10 patients released without confirmed arm use will have spontaneous restoration of function; the other 4 require further remanipulation
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 1152
3. Missed or Delayed Diagnosis
This is a clinical pitfall rather than a true complication of the injury itself, but it carries real consequences:
- An older child often points to the dorsal distal forearm as the site of pain, misleading the clinician toward a distal radial buckle fracture
- The classic traction history is present in only ~50% of cases; 22% present after a fall
- Infants under 6 months typically sustain the injury by rolling over in bed - this can incorrectly trigger a child abuse investigation
- Conditions mimicking pulled elbow that must be excluded:
- Supracondylar fracture
- Lateral condyle fracture
- Radial head/neck fracture
- Radial bowing fracture
- Septic arthritis / osteomyelitis
- Tumour
- Ultrasound can help - the "hook sign" (hyperechoic J-shaped supinator muscle above the radial head) has been reported as 100% sensitive for radial head subluxation and can confirm diagnosis without radiation
- Roberts & Hedges', p. 1151-1152 | Tintinalli's Emergency Medicine
4. Persistent / Delayed Return of Function
- Most children (90%) regain arm use within 30 minutes of successful reduction
- A minority take longer, especially:
- Children seen late after the injury
- Anxious or distressed children who will not use even a successfully reduced limb
- When no click was perceived during reduction
- If function has not returned after 24 hours, re-evaluation and radiographs are indicated
- Delayed return of function beyond 24 hours raises concern for an alternative diagnosis (fracture, infection)
- Rosen's Emergency Medicine, p. 639-640
5. Osteochondritis Dissecans of the Radial Head (Rare, Long-Term)
- Pathomechanically, repetitive or unrecognised radial head subluxation has been linked to the development of osteochondritis dissecans (OCD) of the radial head
- Proposed mechanism: repeated micro-trauma at the radiocapitellar joint disrupts the blood supply to the radial head cartilage
- This is rare and primarily a concern in cases of chronic or recurrent subluxation that goes untreated
- [Tatebe et al., J Orthop Trauma 2012, PMID referenced in PMC article on pulled elbow]
6. Unnecessary Radiation Exposure
- Because the X-ray is almost always normal, ordering radiographs routinely exposes the child to unnecessary radiation
- More importantly, positioning the arm for the lateral view (forearm in supination) can spontaneously reduce the subluxation during the X-ray - meaning the study is normal on the post-reduction film and the clinician may incorrectly conclude there was never a subluxation
- The main role of X-ray is to exclude fracture, not to diagnose pulled elbow
- Radiology Assistant | Roberts & Hedges', p. 1151
7. Non-Accidental Trauma Concern
- Pulled elbow in infants under 6 months from rolling over in bed does not automatically warrant a child abuse investigation - this is an important distinction to avoid unnecessary social/legal consequences for the family
- However, if external signs of trauma (bruising, abrasions, swelling) are present or the history is inconsistent, safeguarding evaluation is appropriate
- Roberts & Hedges', p. 1151
Summary Table
| Complication | Notes |
|---|---|
| Recurrence | ~20%; up to 1/3 of children; resolves after age 5 |
| Reduction failure | Click absent in many; ~30% need 2+ attempts |
| Missed diagnosis | Atypical pain location; 50% no traction history |
| Delayed return of function | Majority by 30 min; re-evaluate at 24 h if not |
| Osteochondritis dissecans | Rare; linked to chronic/recurrent subluxation |
| Unnecessary radiation | X-ray usually normal; may self-reduce during positioning |
| Non-accidental trauma concern | Infants <6 months can injure from rolling - not automatically abuse |
The overall outlook is excellent. Permanent damage is not expected, and the vast majority of children have complete recovery with no long-term sequelae. - Campbell's Operative Orthopaedics 15th Ed | Rosen's Emergency Medicine
Radial head subluxation in x ray in pulled elbow
Finding Sources
Searching the Web
pulled elbow nursemaid radiocapitellar line x-ray normal radial head subluxation radiograph findings
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Loading Image
I now have all the key images and textbook content. Here is a thorough, well-illustrated answer.
X-Ray Findings in Pulled Elbow (Radial Head Subluxation)
The Core Principle
X-rays are almost always NORMAL in pulled elbow.
The annular ligament is a soft tissue structure - it is invisible on plain radiographs. The subluxation is usually subtle and often reduces spontaneously during positioning for the X-ray (especially when the arm is supinated for the AP view). X-rays are not routinely required and should be reserved for specific indications.
- Tintinalli's Emergency Medicine | Campbell's Operative Orthopaedics 15th Ed | Roberts & Hedges'
When to X-Ray
X-rays are indicated when:
- Swelling, bruising, or deformity is present
- History is atypical or uncharacteristic
- Tenderness over the humerus, distal radius, wrist, or clavicle (not just the elbow)
- Child does not regain arm use within 24 hours of reduction
- Concern for non-accidental trauma
- Reduction attempts have failed
Possible X-Ray Findings (When Present)
1. Normal Radiograph (Most Common)
The most common finding in pulled elbow is a completely normal X-ray. No bony injury, no effusion, and normal alignment may all be present even with a confirmed subluxation.
2. The Radiocapitellar Line (Most Important Sign)
This is the key radiographic landmark for assessing radial head alignment on any elbow X-ray.
How to draw it:
- Draw a line along the long axis of the radial shaft/neck
- In a normal elbow, this line should bisect (pass through) the middle of the capitellum on every view - AP, lateral, and oblique
Normal radiocapitellar line on lateral view:

Tintinalli's Emergency Medicine - Figure 141-11: The radiocapitellar line (lower red line) runs along the radial shaft and intersects the capitellum. The anterior humeral line (upper red line) bisects the middle third of the capitellum.
In pulled elbow / radial head subluxation:
- The radiocapitellar line may be displaced by >3 mm from the capitellum
- The line drawn along the radial axis courses superior to (above) the capitellum instead of intersecting it
- This indicates the radial head has shifted out of normal alignment with the capitellum
Abnormal radiocapitellar line in radial head dislocation (B) vs. abnormal anterior humeral line in supracondylar fracture (A):
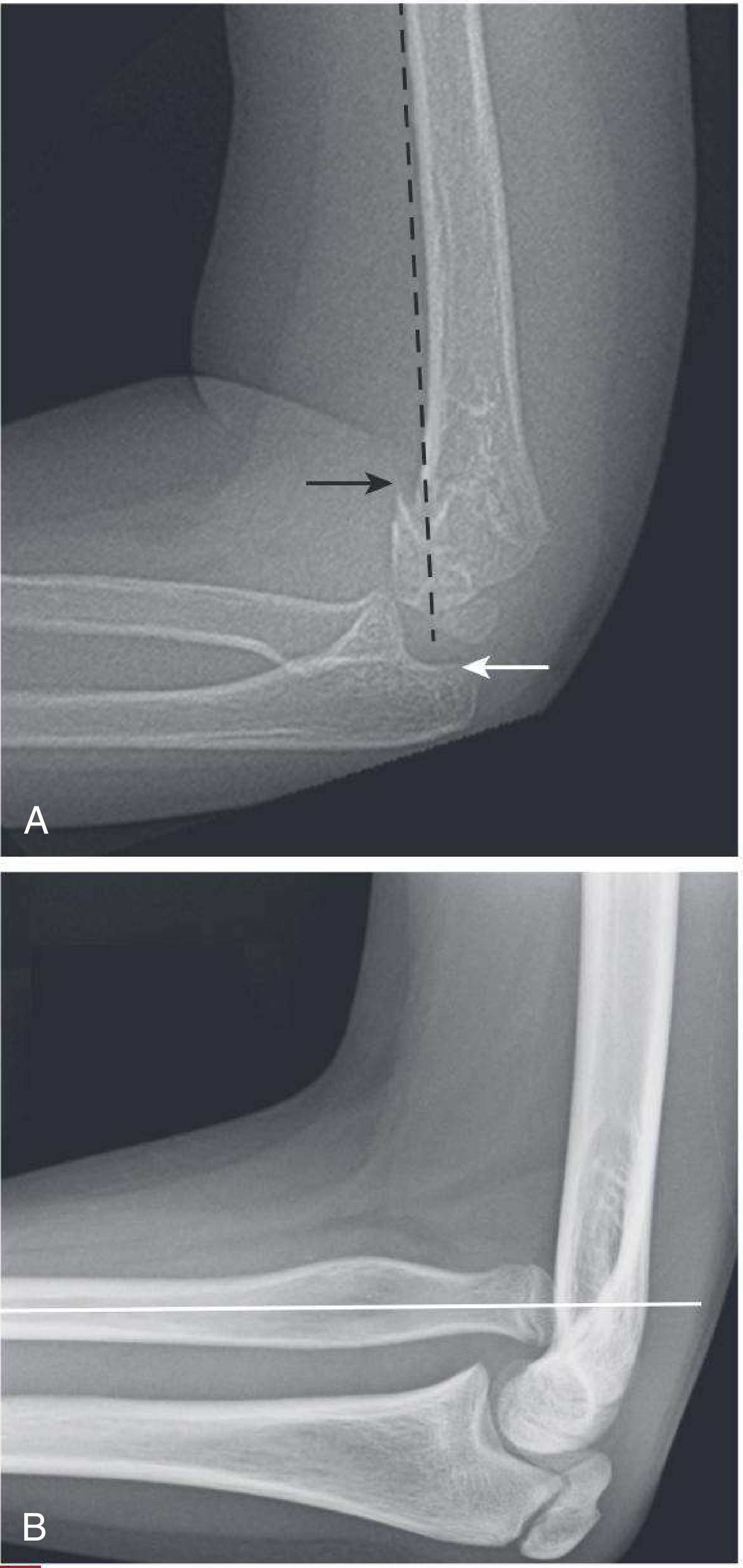
Harriet Lane Handbook 23rd Ed - Figure 26.9(B): The radiocapitellar line (white line) courses superior to the capitellum instead of intersecting it - abnormal, consistent with radial head displacement.
Important caveat: In young children, the radiocapitellar line may not reliably bisect the capitellum even in normal patients, so an abnormal RCL is suggestive of, but not pathognomonic for, injury. - Rosen's Emergency Medicine
3. Increased Radio-Coronoid Distance (Lateral View)
- On the lateral X-ray, there may be a subtle increase in the radio-coronoid distance - the space between the radial head and the coronoid process of the ulna
- This reflects the slight distal displacement of the radial head relative to its normal articulation
- This is a subtle and inconsistently present sign
- NHS Scotland Right Decisions Clinical Guideline (reviewed May 2026)
4. Fat Pad Signs (If Present - Indicates Effusion)
- A posterior fat pad on the lateral view is always pathological - it indicates a joint effusion (haemarthrosis)
- In pulled elbow, fat pad signs are usually absent (no haemarthrosis, since there is no bony injury)
- If a posterior fat pad IS present, think of an occult fracture (most commonly radial head/neck fracture in adults, supracondylar fracture in children) rather than pulled elbow

Harriet Lane Handbook 23rd Ed - Figure 26.10: Posterior fat pad (arrow) = always pathological. "Hourglass sign" (dashed line) = loss of normal hourglass shape of fat pad. In pulled elbow, this sign should be ABSENT.
- Tintinalli's Emergency Medicine | Rosen's Emergency Medicine
5. No Fracture (Role of X-Ray = Exclusion)
The primary reason to take an X-ray in suspected pulled elbow is to exclude fractures, not to confirm the subluxation:
| Fracture to exclude | Clues |
|---|---|
| Supracondylar fracture | Anterior humeral line abnormal; posterior fat pad; swelling |
| Lateral condyle fracture | Subtle metaphyseal fragment; can displace if missed |
| Radial head/neck fracture | Posterior fat pad; tenderness over radial head; fat pad sail sign |
| Monteggia fracture | Ulnar fracture + abnormal radiocapitellar line |
| Distal radial buckle fracture | Older child pointing to distal forearm |
Anatomy Diagram - Normal vs. Pulled Elbow

Radiopaedia - Normal elbow (left) with annular ligament in correct position vs. pulled elbow (right) with the annular ligament displaced/trapped in the joint.
Ultrasound Findings (Alternative to X-Ray)
When the diagnosis is unclear, ultrasound is a useful radiation-free option:
- Uses an anterior longitudinal view across the radiocapitellar joint
- The "hook sign": the hyperechoic J-shaped supinator muscle above the radial head - reported as 100% sensitive for radial head subluxation
- Can also exclude a posterior fat pad (which would suggest a supracondylar fracture)
- Useful for confirming reduction
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 1152
Summary Table
| X-Ray Finding | Pulled Elbow? |
|---|---|
| Normal radiograph | Most common - YES |
| Radiocapitellar line disrupted (>3 mm) | Sometimes - subtle sign |
| Increased radio-coronoid distance | Sometimes - subtle sign |
| Posterior fat pad (positive fat pad sign) | NO - suggests fracture instead |
| Visible fracture | NO - different diagnosis |
| No fracture seen | X-ray main role = fracture exclusion |
Bottom line: Pulled elbow is a clinical diagnosis. X-rays are normal in the vast majority of cases. The radiocapitellar line is the single most important radiographic assessment tool - it must bisect the capitellum on all views. An absent posterior fat pad and no fracture support the diagnosis of pulled elbow over alternatives.
This is a shared conversation. Sign in to Orris to start your own chat.