Maleria
Reading File
Finding Sources
Searching PubMed
malaria treatment AND management
Searching the Web
malaria overview causes symptoms treatment 2025
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks along with excellent diagrams. Let me compile the full response.
Malaria - Complete Overview
Malaria is an ancient parasitic disease caused by Plasmodium protozoa, transmitted to humans through the bite of infected female Anopheles mosquitoes. It remains one of the most significant infectious diseases globally, with over 219 million cases and ~435,000 deaths per year (primarily children in sub-Saharan Africa infected with P. falciparum).
1. Causative Organisms
Five Plasmodium species infect humans:
| Species | Character |
|---|---|
| P. falciparum | Most dangerous - causes severe/cerebral malaria, drug resistance |
| P. vivax | Forms hypnozoites in liver; can relapse months-years later |
| P. ovale | Also forms hypnozoites; milder course |
| P. malariae | Milder; fever cycle every 72 hours |
| P. knowlesi | Zoonotic (from macaques in SE Asia); can be severe, morphologically resembles P. malariae |
P. falciparum is the predominant species in Africa and the primary cause of malaria-related mortality. P. vivax dominates in Asia and the Americas. Nearly all genetic erythrocyte defects (sickle cell trait, thalassemia, G6PD deficiency) are most prevalent in malaria-endemic regions - many confer partial protection from severe disease.
2. Life Cycle
Diagram (from Lippincott Illustrated Reviews Pharmacology):
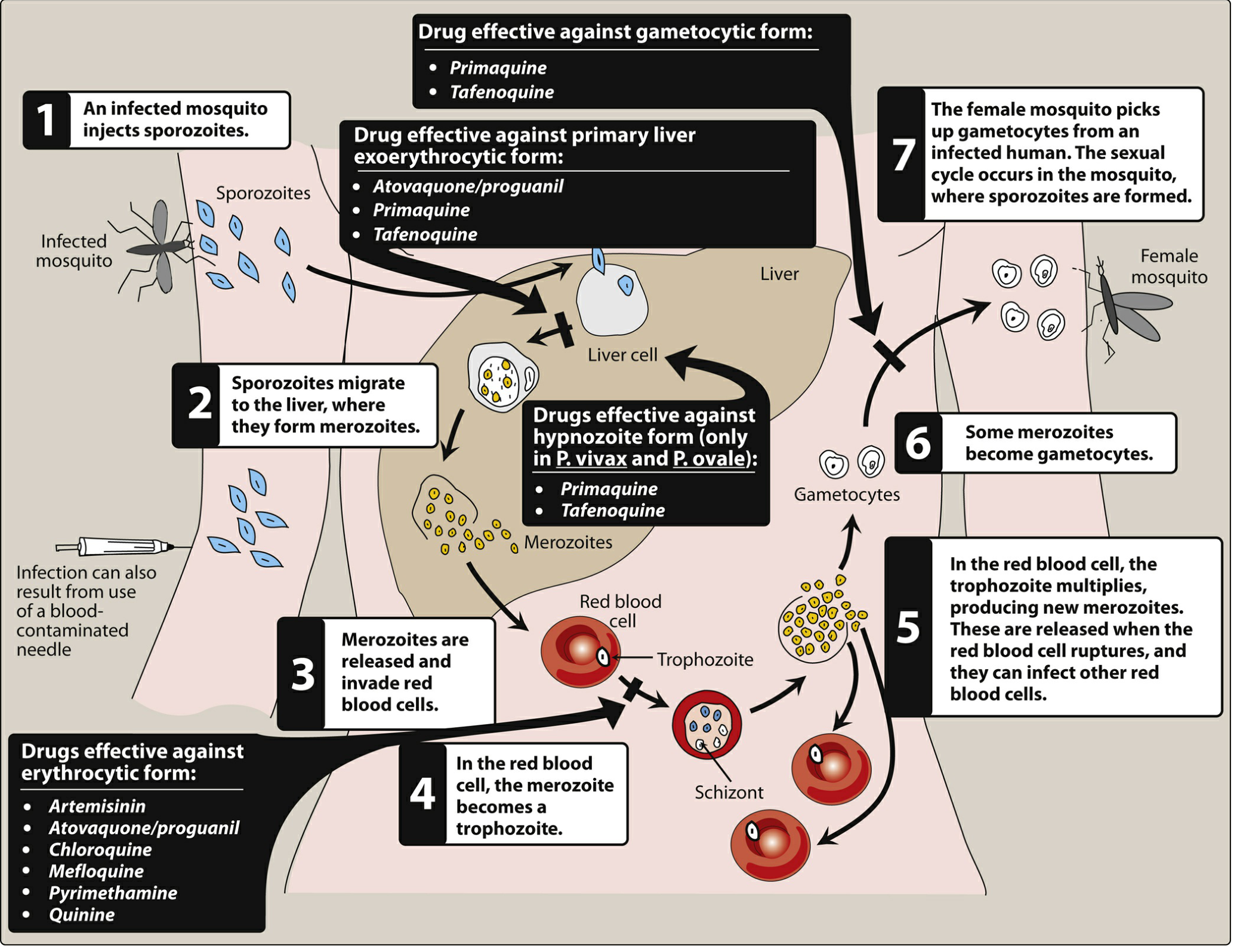
Figure: Life cycle of the malarial parasite, showing sites of action of antimalarial drugs
Diagram (from Robbins & Kumar Basic Pathology - P. falciparum detail):

Figure: Life cycle of Plasmodium falciparum - hepatic stage (left) and erythrocytic stage (right)
Steps:
- Infected female Anopheles mosquito injects sporozoites into the bloodstream
- Sporozoites travel to the liver → invade hepatocytes (clinically silent hepatic phase, 6-7 days)
- Hepatic schizonts mature and release thousands of merozoites
- Merozoites invade erythrocytes (red blood cells)
- Inside RBCs: merozoite → ring trophozoite → schizont → new merozoites (erythrocytic cycle)
- RBCs rupture, releasing merozoites → infect more RBCs (this is what causes clinical illness)
- Some merozoites become sexual gametocytes, taken up by a feeding mosquito to complete the cycle
Key point: Only the erythrocytic stage causes clinical disease. P. vivax and P. ovale also form dormant hypnozoites in the liver that can reactivate and cause relapse.
- Fever cycle: every 48 hours for P. falciparum, P. vivax, P. ovale; every 72 hours for P. malariae; every 24 hours for P. knowlesi
3. Pathogenesis
- Lysis of infected RBCs causes hemolytic anemia and releases fever-triggering inflammatory mediators (cytokines, chemokines)
- P. falciparum produces a unique virulence factor: PfEMP1 (Plasmodium falciparum erythrocyte membrane protein 1), displayed on surface "knobs" of infected RBCs
- PfEMP1 binds endothelial adhesion molecules (ICAM-1, VCAM-1, CD36) → cytoadherence and sequestration of infected RBCs in microvasculature
- Sequestration in brain vessels causes cerebral malaria - the most feared complication
- A brown pigment called hemozoin (from hemoglobin degradation by the parasite) accumulates in spleen, liver, lymph nodes, and bone marrow
- Massive mononuclear phagocyte activation leads to splenomegaly and occasional hepatomegaly
4. Clinical Features
Typical presentation:
- Prodrome: headache, fatigue, myalgia
- Classic triad: fever, chills, sweats (often paroxysmal, correlating with RBC rupture cycles)
- Hemolytic anemia, thrombocytopenia
- Fever may be continuous early on, especially with P. falciparum
Severe/complicated malaria (mainly P. falciparum):
- Cerebral malaria: altered consciousness, convulsions, coma, death
- Severe anemia
- Respiratory distress / ARDS (bilateral pulmonary opacities on chest X-ray)
- Acute kidney injury / renal failure
- Jaundice (due to hemolysis + hepatic involvement)
- Blackwater fever: massive intravascular hemolysis → hemoglobinuria (dark urine), renal failure
- Multiorgan failure - can progress within days in non-immune patients
At highest risk: children, pregnant women, non-immune travelers.
5. Diagnosis
- Gold standard: Thick and thin peripheral blood smears - identifies species and parasitemia level
- Rapid Diagnostic Tests (RDTs): detect malaria antigens (HRP-2 for P. falciparum) - fast but may have lower sensitivity, cannot always differentiate species
- PCR: most sensitive, useful for low parasitemia and species confirmation
- Travel history is essential - ask about exact dates, countries visited, prophylaxis taken, mosquito precautions
6. Antimalarial Drugs
Drugs are classified by where they act in the parasite life cycle:
| Drug | Class | Primary Use |
|---|---|---|
| Artemisinin (artesunate, artemether, dihydroartemisinin) | Sesquiterpene lactone endoperoxide | Blood schizonticide - 1st line for P. falciparum; IV artesunate for severe disease |
| Chloroquine | 4-Aminoquinoline | Treatment/prophylaxis for chloroquine-sensitive strains |
| Quinine | Quinoline methanol | IV/oral for P. falciparum (second-line) |
| Mefloquine | Quinoline methanol | Prophylaxis and treatment of P. falciparum |
| Atovaquone-proguanil (Malarone) | Quinone + folate antagonist | Treatment and chemoprophylaxis of P. falciparum |
| Primaquine | 8-Aminoquinoline | Kills liver hypnozoites (P. vivax, P. ovale); gametocidal |
| Tafenoquine | 8-Aminoquinoline | Same as primaquine (single dose convenience) |
| Sulfadoxine-pyrimethamine (Fansidar) | Folate antagonist combo | Some chloroquine-resistant P. falciparum; IPT in pregnancy |
| Doxycycline | Tetracycline | Chemoprophylaxis; combination with quinine |
| Lumefantrine (combined with artemether as Coartem) | Amyl alcohol | P. falciparum (front-line ACT) |
Important drug notes:
- Artemisinin-based combination therapies (ACTs) are now the WHO-recommended first-line treatment for uncomplicated P. falciparum malaria
- Primaquine and tafenoquine are required after treatment of P. vivax/P. ovale to eliminate hypnozoites and prevent relapse - but are contraindicated in G6PD deficiency (can cause life-threatening hemolytic anemia)
- Resistance is a major and growing problem, especially partial artemisinin resistance in SE Asia
7. Prevention
- Insecticide-treated bed nets (ITNs): most cost-effective intervention
- Indoor Residual Spraying (IRS) with insecticides
- Chemoprophylaxis for travelers: atovaquone-proguanil, doxycycline, or mefloquine (choice depends on destination and resistance pattern)
- Seasonal malaria chemoprevention (SMC) in Sahel region children
- Intermittent Preventive Treatment in Pregnancy (IPTp) with sulfadoxine-pyrimethamine
- Vaccines: RTS,S/AS01 (Mosquirix) and R21/Matrix-M have been deployed in sub-Saharan Africa for children under 5 - partial but significant protection; expected to prevent thousands of deaths from cerebral malaria
8. Malaria's Evolutionary Impact
Malaria has exerted one of the strongest selective pressures on the human genome. Conditions like sickle cell trait (HbS), alpha/beta-thalassemia, G6PD deficiency, Duffy antigen negativity (near-complete protection against P. vivax in much of sub-Saharan Africa), and ovalocytosis are all most prevalent in historically malaria-endemic regions and offer varying degrees of protection.
Sources:
- Murray & Nadel's Textbook of Respiratory Medicine, p. 1352
- Robbins & Kumar Basic Pathology, p. 392
- Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 1430-1432
- Lippincott Illustrated Reviews Pharmacology, p. 1167-1169
- ROSEN's Emergency Medicine, p. 1215+
- Nature: Malaria past, present, future review (2025)
- Malaria Journal: Epidemiology and management strategies (2025)
This is a shared conversation. Sign in to Orris to start your own chat.