BCG vaccination according to park textbook of ps,
BCG Vaccination
History
(1) Aim
(2) Vaccine
- BCG is the only widely used live bacterial vaccine.
- Consists of living attenuated bovine strain of tubercle bacilli.
- Derived from the original Calmette strain.
- Many substrains have evolved due to different production methods.
- WHO recommended strain: "Danish 1331" (used at BCG Laboratory, Guindy, Chennai since January 1967).
- Quality control: International Reference Centre at Copenhagen.
(3) Types of Vaccine
- Liquid (fresh) vaccine
- Freeze-dried vaccine - more stable, superior keeping quality; present-day vaccines are distributed in this form.
- Stable for several weeks at ambient tropical temperature.
- Up to 1 year if kept away from direct light and refrigerated at below 10°C.
- Must be protected from light during storage (wrapped in double layer of red or black cloth).
- Normal saline is the recommended diluent (distilled water may cause irritation).
- Reconstituted vaccine must be used within 3 hours; leftover vaccine must be discarded.
(4) Dosage
| Age | Dose |
|---|---|
| Standard dose | 0.1 mg in 0.1 ml |
| Newborns < 4 weeks | 0.05 ml (reduced because newborn skin is thin; full dose risks penetrating deeper tissue, causing local abscess and axillary lymphadenopathy) |
(5) Administration
- Route: Strictly intradermal using a "Tuberculin" syringe (Omega microstat syringe with 1 cm, 26-gauge intradermal needle).
- Syringe-and-needle technique is the most precise method.
- Other methods (bifurcated needle, dermo-jet) are less accurate.
- Subcutaneous injection increases risk of abscess formation.
- Site: Just above the insertion of the left deltoid muscle (left upper arm).
- Skin must not be contaminated with antiseptic/detergent; if alcohol is used, it must evaporate before injection.
- No other injection should be given into the BCG-vaccinated arm for at least 6 months.
(6) Age Policy
- India (high-TB prevalence countries): BCG given very early in infancy:
- At birth (for institutional deliveries), OR
- At 6 weeks simultaneously with DPT and polio
- BCG given early in life provides high protection, especially against:
- Severe forms of childhood tuberculosis
- Tuberculous meningitis
- Low-prevalence countries: Restriction to high-risk groups (hospital personnel, tuberculin-negative contacts of TB cases especially MDR-TB).
(7) Normal Phenomena After Vaccination
| Timeframe | Expected Finding |
|---|---|
| 2-3 weeks post-injection | Papule develops at injection site |
| ~5 weeks | Papule reaches 4-8 mm diameter |
| Subsequently | Subsides or forms a shallow ulcer (usually crust-covered) |
| 6-12 weeks | Spontaneous healing leaving a permanent, round scar of 4-8 mm |
| 8 weeks (sometimes 14 weeks) | Individual becomes Mantoux-positive |
(8) Complications
| Complication | Frequency |
|---|---|
| Prolonged ulceration / suppurative lymphadenitis | 1-10% of vaccinations |
| Osteomyelitis | Rare |
| Disseminated BCG infection | < 1 per million vaccinations (usually with severe cellular immunodeficiency) |
| Death | Very rare |
- First: Aspiration
- If unsuccessful: Incision + local applications of PAS or INH powder (daily)
- No systemic INH needed
- Patient should be reassured of harmless nature
(9) Protective Value
- Duration of protection: 15 to 20 years.
- Mechanism: Local BCG infection generates immunity associated with tuberculin hypersensitivity.
- First prospective controlled trial: 80% effectiveness over 20 years.
- Range of protection in various trials worldwide: 0 to 80% (highly variable).
- South India trial found poor protection, possibly due to prior exposure to non-tuberculous environmental mycobacteria (e.g., M. vaccae, M. non-chromogenicum) conferring partial immunity and masking BCG benefit. M. kansasii and M. scrofulaceus have an antagonistic action against BCG.
- Infants and young children vaccinated before contact with environmental mycobacteria do derive protection.
- WHO holds it unreasonable to stop current BCG vaccination programmes.
(10) Revaccination
- Duration of protection is still disputed even 90 years after vaccine development.
- BCG revaccination is NOT included in India's official EPI (Expanded Programme on Immunization) schedule.
- Booster doses are not routinely indicated.
(11) Contraindications
- Generalized eczema or infective dermatosis
- Hypogammaglobulinaemia
- Known/suspected congenital immunodeficiency
- Leukaemia, lymphoma, or generalized malignant diseases
- Patients under immunosuppressive treatment (corticosteroids, alkylating agents, antimetabolites, radiation)
- Symptomatic HIV infection
- Pregnancy
(12) Direct BCG Vaccination
- Direct BCG vaccination (without prior tuberculin test) is India's national policy.
- Allows faster, more complete coverage at lower cost.
- No adverse effects reported in tuberculin-positive reactors.
- Best practice: administer BCG during infancy before contact with environmental mycobacteria.
(13) Impact
- BCG is less effective than active case-finding and chemotherapy.
- Offers only partial protection.
- A 1982 WHO Expert Committee concluded BCG can prevent tuberculosis in uninfected individuals but has only relatively small epidemiological effect on overall risk of infection in the community.
(14) BCG Vaccination and HIV Infection
- Previous WHO recommendation: In high TB-burden countries, BCG should be given to all healthy infants at birth unless the child had symptomatic HIV infection.
- Revised recommendation (GACVS): Children known to be HIV-infected, even if asymptomatic, should NOT be immunized with BCG vaccine, because:
- HIV-infected children vaccinated at birth who later developed AIDS were at increased risk of disseminated BCG disease.
- Benefits of preventing severe TB are outweighed by risks.
- However: Most infants born to HIV-infected mothers are themselves uninfected (due to PMTCT interventions) and would benefit from BCG.
- Accurate HIV diagnosis in the first year of life is technically challenging and expensive; WHO recommends HIV testing at around 6 weeks of age, but this is often after BCG has already been given.
(15) Combined Vaccination
- BCG may be given simultaneously with:
- Oral polio vaccine
- DPT vaccine (in a different arm) - without reducing immune responses or increasing complications
- Mixed vaccines containing BCG have not yet been introduced.
Criteria for Switching from General to Selective BCG Vaccination ("Low Endemicity" Criteria)
- (a) Average annual notification rate of smear-positive pulmonary TB < 5 per 100,000
- (b) Average annual notification rate of tubercular meningitis in children under 5 years < 1 per 10 million population over previous 5 years
- (c) Average annual risk of TB infection < 0.1%
Summary
BCG vaccination is a fundamental component of a national tuberculosis programme. Despite contradictory trial evidence, BCG plays a valuable role in preventing severe forms of childhood tuberculosis - especially meningitis and miliary tuberculosis. BCG is part of WHO's Expanded Programme on Immunization (EPI). The greatest need remains in developing countries where TB is still a major health problem.
- Park's Textbook of Preventive and Social Medicine, pp. 231-232
Search for recent clinical guidelines on BCG in HIV-positive infants
BCG vaccine HIV-infected infants
BCG vaccination HIV positive infants guidelines WHO 2024 2025
BCG vaccine HIV infants safety disseminated
https://cdn.who.int/media/docs/default-source/immunization/i…
BCG vaccination HIV exposed infants ART immunocompromised
WHO BCG HIV infant 2024 2025 ART delay recommendation GACVS
BCG vaccine HIV children immunization
https://www.mdpi.com/2076-393X/14/1/40
PMID: 40334156
PMID: 38822485
PMID: 37814073
Recent Clinical Guidelines: BCG Vaccination in HIV-Positive Infants
Overview of the Core Problem
WHO / GACVS Current Recommendations (Updated December 2025)
| Infant Category | Recommendation |
|---|---|
| Confirmed HIV-infected (by early virological testing) | Delay BCG until ART started AND infant is immunologically stable (CD4% >25%) |
| HIV-infected, on ART, clinically well, immunologically stable (CD4% >25% if <5 yrs; CD4 ≥200 if >5 yrs) | Should be vaccinated with BCG |
| HIV-exposed but uninfected (HEU) - unknown status, no clinical signs, mother HIV+ | Vaccinate - benefits outweigh risks regardless of whether mother is on ART |
| Born to women of unknown HIV status | Vaccinate - benefits outweigh risks |
| Known HIV-infected (even asymptomatic) | Do NOT vaccinate with BCG |
Rationale Behind These Recommendations
- Disseminated BCG disease risk approaches 1% in HIV-positive infants - data from Argentina and South Africa. This is enormously higher than the <1 per million risk in immunocompetent infants.
- HIV severely impairs BCG-specific T-cell responses in the first year of life - meaning BCG may provide little or no protection against TB in these infants, removing the benefit side of the risk-benefit equation.
- HAART/ART may reduce dBCG disease rate and immune reconstitution inflammatory syndrome (IRIS) risk, supporting the "delay-until-stable-on-ART" strategy.
- Early virological testing (recommended by WHO at ~6 weeks of age) is often technically demanding and expensive in high-burden settings, and is frequently done after BCG has already been administered.
The Practical Dilemma in Low-Resource Settings
- BCG vaccination should continue at birth for all infants regardless of HIV exposure, given the high TB endemicity in such populations.
- Close follow-up of infants known to be born to HIV-infected mothers is mandatory to detect and treat any BCG-related complications early.
- Where adequate HIV services exist (early virological testing + rapid ART initiation), BCG should be deferred until HIV status is confirmed.
Recent PubMed Evidence
Comparison: Park's Textbook vs. Current Guidelines
| Point | Park's Textbook (older edition) | Current WHO 2025 |
|---|---|---|
| HIV-positive symptomatic infant | Do NOT vaccinate | Do NOT vaccinate |
| HIV-positive asymptomatic infant | Not clearly addressed | Do NOT vaccinate (GACVS revised) |
| HIV-exposed but uninfected | Not specifically addressed | Vaccinate (benefits > risks) |
| HIV+ on ART, clinically stable | Not addressed | CAN vaccinate if CD4% >25% |
| Delay strategy with early testing | Not addressed | Defer BCG until HIV status confirmed, then start ART first |
Summary
- Known HIV-infected infant = BCG contraindicated, even if asymptomatic
- Unknown status in a high-burden setting = vaccinate at birth, follow up closely
- HIV-exposed but confirmed uninfected = vaccinate normally
- HIV-infected but stable on ART (CD4% >25%) = BCG can be given
cardinal symptoms of tb
Cardinal Symptoms of Tuberculosis
Respiratory (Pulmonary) Symptoms
1. Cough
- The most common and earliest symptom
- Initially dry and non-productive, progressing to productive (purulent or mucoid sputum) as cavitation develops
- Chronic cough lasting >2-3 weeks is the key screening threshold
- Cough may develop late in primary TB, usually only after tubercle cavitation
2. Hemoptysis (Blood in Sputum)
- Ranges from blood-streaked sputum to frank hemoptysis
- Indicates cavitation or erosion of a blood vessel by the TB lesion
- One of the most specific "alarm" symptoms that should trigger immediate TB workup
- Described across all major textbooks as a cardinal feature
3. Chest Pain
- Usually pleuritic in nature - sharp, worsening on breathing/coughing
- Suggests pleural involvement (pleuritis or pleural effusion)
- May also arise from extensive parenchymal disease
4. Dyspnea (Breathlessness)
- Occurs with extensive lung disease, pleural effusion, or miliary TB
- Usually a later feature in the course of disease
Constitutional (Systemic) Symptoms
5. Fever
- Characteristically low-grade with an evening rise in temperature (pyrexia of insidious onset)
- Often described as a "diurnal fever" - temperature peaks in the late afternoon/evening
- The patient may be unaware of fever, only noticing the associated night sweats
6. Night Sweats
- Drenching night sweats - the patient wakes soaked
- Caused by the evening fever and its subsequent defervescence overnight
- Highly characteristic of TB and other chronic granulomatous/infectious diseases
7. Weight Loss and Anorexia
- Progressive, unexplained weight loss
- Anorexia (loss of appetite) typically precedes the weight loss
- In advanced disease, leads to frank cachexia (wasting)
- Caused by cytokine-driven catabolism (TNF-α, IL-1, IL-6) and reduced caloric intake
8. Fatigue and Malaise
- Generalized weakness, lassitude, and easy fatigability
- Often the earliest and most subtle constitutional complaint
- Patients frequently attribute it to overwork or stress, delaying presentation
Summary Table
| Symptom | Type | Key Feature |
|---|---|---|
| Chronic cough (>2 weeks) | Respiratory | Earliest, most common |
| Hemoptysis | Respiratory | Blood-stained/frank; cavitation sign |
| Chest pain (pleuritic) | Respiratory | Pleural involvement |
| Dyspnea | Respiratory | Late feature |
| Fever (low-grade, evening rise) | Constitutional | Insidious onset |
| Night sweats | Constitutional | Drenching, nocturnal |
| Weight loss / Anorexia | Constitutional | Progressive, unexplained |
| Fatigue / Malaise | Constitutional | Earliest and most subtle |
Primary vs. Reactivation TB - Symptom Differences
| Feature | Primary TB | Reactivation TB |
|---|---|---|
| Initial infection | Often asymptomatic | Symptoms present |
| Systemic symptoms | Mild - cough, fever, malaise | Fever, night sweats, weight loss (prominent) |
| Pulmonary symptoms | Cough, chest pain | Productive cough, hemoptysis, dyspnea, pleuritic pain |
| Progression | Slowly progressive | More prominent symptoms, upper lobe cavitation |
| Detection | Often by TST or CXR | Clinical symptoms + CXR |
- Tintinalli's Emergency Medicine, p. 796
Classic "Alarm" Triad for TB Screening
Hemoptysis + Night sweats + Weight loss
- Tintinalli's Emergency Medicine: "Clues that suggest tuberculosis include hemoptysis, night sweats, and weight loss."
- Textbook of Family Medicine: "Cough, hemoptysis, night sweats, fever, and weight loss suggest the need to investigate for tuberculosis."
Extrapulmonary TB - Additional Cardinal Features by Site
| Site | Cardinal Symptom |
|---|---|
| Lymph nodes (Scrofula) | Painless cervical lymphadenopathy |
| Spine (Pott's disease) | Back pain, kyphosis, paraplegia |
| Meninges (TBM) | Headache, neck stiffness, altered sensorium |
| Peritoneum | Abdominal pain, ascites, doughy abdomen |
| Pericardium | Chest pain, dyspnea, JVP elevation |
| Kidney (Renal TB) | Sterile pyuria, hematuria, flank pain |
| Miliary TB | High fever, hepatosplenomegaly, choroid tubercles |
A Note on Atypical Presentations
- Tietz Textbook of Laboratory Medicine: "Typical signs and symptoms of tuberculosis may be absent in individuals with advanced AIDS, resulting in a delay in diagnosis."
make the bcg vaccination into a flowchart for revison
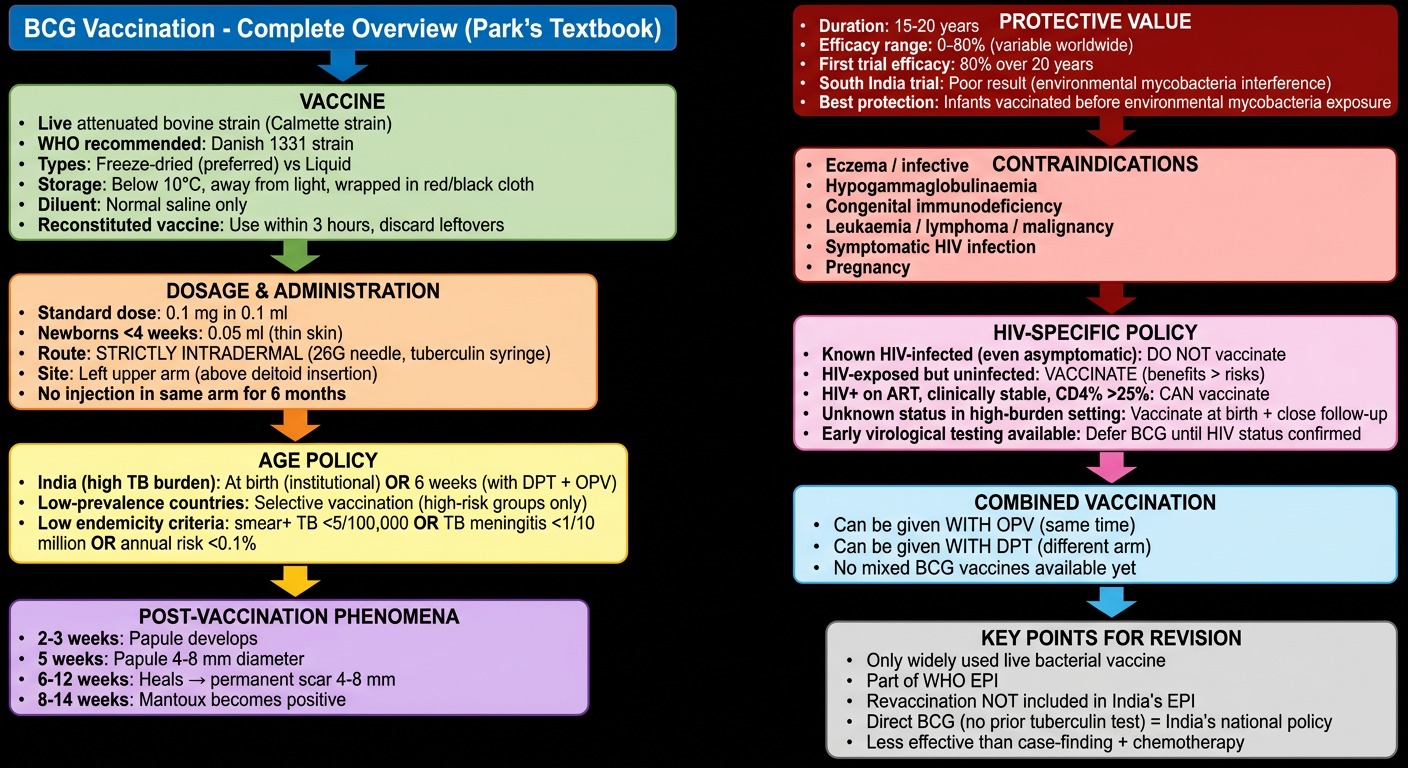
A detailed medical revision flowchart titled "BCG Vaccination - Complete Overview (Park's Textbook)" covering all the following topics in a structured top-to-bottom flow with color-coded boxes: START: BCG Vaccination (large blue header box) Branch 1 - VACCINE (green box): - Live attenuated bovine strain (Calmette strain) - WHO recommended: Danish 1331 strain - Types: Freeze-dried (preferred) vs Liquid - Storage: Below 10°C, away from light, wrapped in red/black cloth - Diluent: Normal saline only - Reconstituted vaccine: Use within 3 hours, discard leftovers Branch 2 - DOSAGE & ADMINISTRATION (orange box): - Standard dose: 0.1 mg in 0.1 ml - Newborns <4 weeks: 0.05 ml (thin skin) - Route: STRICTLY INTRADERMAL (26G needle, tuberculin syringe) - Site: Left upper arm (above deltoid insertion) - No injection in same arm for 6 months Branch 3 - AGE POLICY (yellow box): - India (high TB burden): At birth (institutional) OR 6 weeks (with DPT + OPV) - Low-prevalence countries: Selective vaccination (high-risk groups only) - Low endemicity criteria: smear+ TB <5/100,000 OR TB meningitis <1/10 million OR annual risk <0.1% Branch 4 - POST-VACCINATION PHENOMENA (purple box): - 2-3 weeks: Papule develops - 5 weeks: Papule 4-8 mm diameter - 6-12 weeks: Heals → permanent scar 4-8 mm - 8-14 weeks: Mantoux becomes positive Branch 5 - COMPLICATIONS (red box): - Ulceration/lymphadenitis: 1-10% - Disseminated BCG: <1 per million (except immunodeficient) - Management of abscess: Aspiration → if failed: incise + local PAS/INH powder (NO systemic INH) Branch 6 - PROTECTIVE VALUE (teal box): - Duration: 15-20 years - Efficacy range: 0-80% (variable worldwide) - First trial efficacy: 80% over 20 years - South India trial: Poor result (environmental mycobacteria interference) - Best protection: Infants vaccinated before environmental mycobacteria exposure Branch 7 - CONTRAINDICATIONS (dark red box): - Eczema / infective dermatosis - Hypogammaglobulinaemia - Congenital immunodeficiency - Leukaemia / lymphoma / malignancy - Immunosuppressive therapy - Symptomatic HIV infection - Pregnancy Branch 8 - HIV-SPECIFIC POLICY (pink box): - Known HIV-infected (even asymptomatic): DO NOT vaccinate - HIV-exposed but uninfected: VACCINATE (benefits > risks) - HIV+ on ART, clinically stable, CD4% >25%: CAN vaccinate - Unknown status in high-burden setting: Vaccinate at birth + close follow-up - Early virological testing available: Defer BCG until HIV status confirmed Branch 9 - COMBINED VACCINATION (light blue box): - Can be given WITH OPV (same time) - Can be given WITH DPT (different arm) - No mixed BCG vaccines available yet BOTTOM BOX - KEY POINTS FOR REVISION: - Only widely used live bacterial vaccine - Part of WHO EPI - Revaccination NOT included in India's EPI - Direct BCG (no prior tuberculin test) = India's national policy - Less effective than case-finding + chemotherapy Clean white background, clear arrows connecting sections, color-coded boxes with bold headers, small readable text, compact layout suitable for medical exam revision
| Color | Section |
|---|---|
| 🟢 Green | Vaccine (strain, types, storage) |
| 🟠 Orange | Dosage & Administration |
| 🟡 Yellow | Age policy & low-endemicity criteria |
| 🟣 Purple | Post-vaccination phenomena (timeline) |
| 🔴 Red | Complications & management |
| 🩵 Teal | Protective value & efficacy |
| 🟥 Dark red | Contraindications |
| 🩷 Pink | HIV-specific policy (updated GACVS) |
| 💙 Light blue | Combined vaccination & key revision points |
- Dose: 0.1 ml standard / 0.05 ml for newborns <4 weeks
- Scar: 4-8 mm, appears by 6-12 weeks
- Mantoux positive: by 8 weeks (max 14 weeks)
- Complications: Lymphadenitis 1-10%, disseminated <1/million
- Duration: 15-20 years protection
- Efficacy: 0-80% (variable) - first trial showed 80%