Explain posterior sub capsular cataract
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Searching Images
posterior subcapsular cataract slit lamp retroillumination
Searching PubMed
"posterior subcapsular cataract" etiology risk factors
Loading Image
I now have comprehensive information to provide a thorough answer. Here is a complete explanation of posterior subcapsular cataract (PSC):
Posterior Subcapsular Cataract (PSC)
Definition & Location
A posterior subcapsular cataract is an opacity of the crystalline lens situated just anterior to the posterior capsule, at the posterior pole of the lens. Unlike nuclear or cortical cataracts, it occupies the visual axis centrally, which gives it a disproportionately severe impact on vision relative to its physical size.
Pathology & Appearance
Histology / Cellular basis:
- The vacuoles seen in PSC are swollen migratory lens epithelial cells, known as bladder cells or Wedl cells
- These are similar to the cells seen in posterior capsular opacification (PCO) after cataract surgery
- Lens epithelial cells from the germinative zone migrate posteriorly and undergo aberrant differentiation
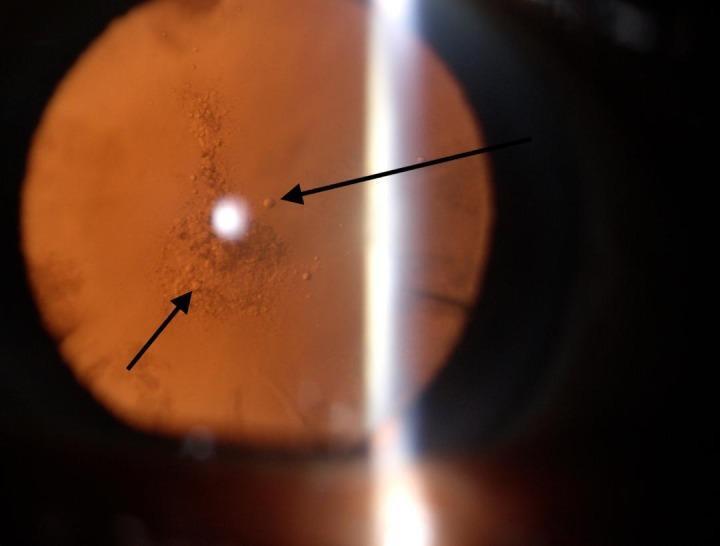
Slit-lamp appearance:
- On oblique slit-lamp biomicroscopy: granular or plaque-like opacity
- On retroillumination: appears black and vacuolated — this is the classic hallmark
Symptoms
PSC causes symptoms that are disproportionately severe for the size of the opacity due to its central posterior location:
| Symptom | Mechanism |
|---|---|
| Glare (dominant symptom) | Scattering of light at the nodal point — characteristically worse with oncoming headlights at night |
| Reduced visual acuity in bright light | Pupil constricts in bright light, concentrating all incoming light through the PSC opacity |
| Reduced near vision | Near tasks cause miosis → more light passes through the opacity |
| Contrast sensitivity loss | Scattering degrades image contrast |
| Monocular diplopia | In some cases |
Key clinical pearl: Symptoms are worse in bright light and during near work (reading, bright sunlight) — both conditions cause miosis, funneling light through the central opacity. This distinguishes PSC from nuclear cataract, which often impairs distance vision more.
Causes & Associations
Age-related (most common)
PSC is one of the three major subtypes of age-related cataract, alongside nuclear sclerotic and cortical cataract.
Drugs
- Corticosteroids (most important drug cause): systemic, topical, and inhaled steroids all carry risk. Initial opacities are posterior subcapsular, with subsequent anterior subcapsular involvement. Children may be more susceptible. Early opacities may regress if steroids are stopped, though progression can still occur after withdrawal.
- Phenothiazines (e.g., chlorpromazine): can cause both anterior and posterior subcapsular opacities
- Allopurinol (long-term, high cumulative dose)
Systemic diseases
| Disease | Type of opacity |
|---|---|
| Diabetes mellitus | PSC (also nuclear sclerosis; classic snowflake is rare) |
| Myotonic dystrophy | PSC with stellate morphology (≥90% of patients, by 5th decade) |
| Atopic dermatitis | Primarily anterior subcapsular shield; PSC also occurs |
| Neurofibromatosis type 2 | PSC (>60% of patients, early adulthood) |
Secondary (complicated) cataract
- Chronic anterior uveitis: earliest change is a polychromatic lustre at the posterior pole; inflammation and steroid treatment both contribute
- Retinitis pigmentosa: PSC is part of the classic tetrad (bone-spicule pigmentation, pale waxy disc, attenuated arterioles, PSC) | Other | Radiation (ionizing/infrared), trauma (including lightning strike), high myopia |
Comparison with Other Cataract Types
| Feature | PSC | Nuclear | Cortical |
|---|---|---|---|
| Location | Posterior, central | Nucleus | Anterior/posterior cortex |
| Glare | Severe | Mild–moderate | Moderate |
| Near vision | Severely reduced | Usually preserved early | Variable |
| Bright-light symptoms | Worse | Less affected | Moderate |
| Appearance | Granular/plaque, vacuolated on retroillumination | Yellow-brown, "second sight" myopia | Spoke-like/wedge opacities |
Management
PSC is managed like other cataracts:
- No medical treatment reverses or prevents progression
- Surgery: phacoemulsification with intraocular lens implantation — the same procedure used for all acquired cataracts and is highly successful in restoring vision
- Timing: surgery is indicated when visual impairment significantly affects daily function
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed. (pp. 323–325); The Wills Eye Manual; Goldman-Cecil Medicine.
Types of IOL
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Searching Images
types of intraocular lens IOL monofocal multifocal toric
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.