Ventilator strategy for ards treatment full details for md exams 15marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching PubMed
ARDS mechanical ventilation lung protective strategy
I now have everything I need for a thorough, exam-quality MD answer. Here is the complete, structured response:
Ventilator Strategy for ARDS - Full Details (MD Exam, 15 Marks)
1. Introduction and Rationale
Acute Respiratory Distress Syndrome (ARDS) is characterized by acute onset hypoxemia, bilateral radiographic infiltrates, and reduced respiratory compliance, occurring within 1 week of a clinical insult (Berlin Definition, 2012). Severity is classified by the PaO2/FiO2 (P/F) ratio on PEEP ≥5 cm H2O:
| Severity | PaO2/FiO2 |
|---|---|
| Mild | 201-300 mmHg |
| Moderate | 101-200 mmHg |
| Severe | ≤100 mmHg |
Mechanical ventilation is the cornerstone of ARDS management. However, the ventilator itself can worsen lung injury - a concept termed Ventilator-Induced Lung Injury (VILI). All modern ventilator strategies are designed to minimize VILI while maintaining adequate gas exchange.
2. Pathophysiologic Basis: The "Baby Lung" Concept
CT studies of ARDS lungs reveal that consolidation, atelectasis, and normal alveoli are heterogeneously distributed - unlike the diffuse-looking pattern on plain CXR. The available aerated lung is only a small fraction of total lung volume, termed the "baby lung" by Gattinoni et al. This has critical implications:
- A tidal volume of 10-15 mL/kg actual body weight distributes only to this small fraction of open alveoli
- Results in massive alveolar overdistension (volutrauma)
- Repetitive collapse and reopening of unstable alveoli during each breath cycle = atelectrauma
- Mechanical stretch triggers release of systemic proinflammatory cytokines = biotrauma
- These cytokines mediate multiorgan failure
The three mechanisms of VILI are thus:
- Volutrauma - alveolar overdistension from high tidal volume/plateau pressure
- Atelectrauma - shear stress from cyclic alveolar collapse/reopening
- Biotrauma - cytokine-mediated systemic inflammation and remote organ injury
3. Pressure-Volume (P-V) Curve in ARDS
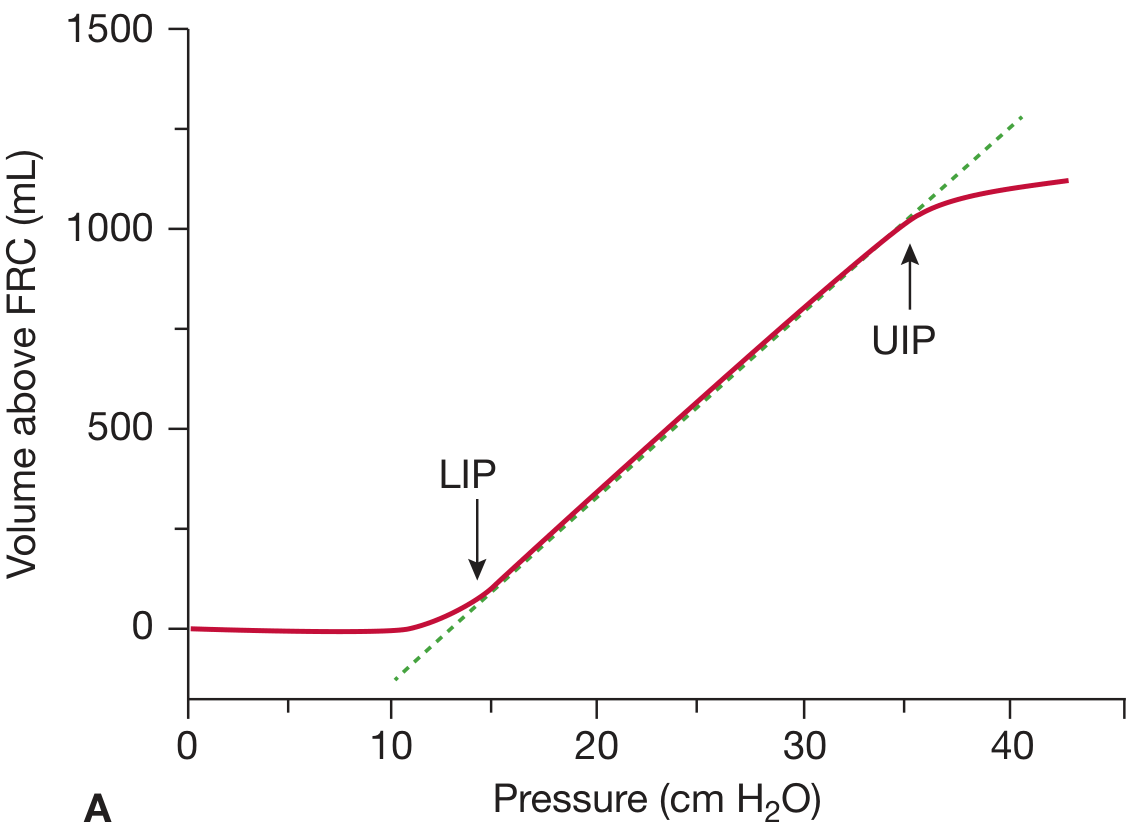
The static inspiratory P-V curve of the ARDS lung is S-shaped:
- Lower Inflection Point (LIP): ~14 cm H2O - below this, alveoli are collapsed; PEEP should be set just above LIP to prevent atelectrauma
- Upper Inflection Point (UIP): ~35 cm H2O - above this, alveoli are overdistended; plateau pressure must stay below UIP (target ≤30 cm H2O)
- The safe operating window for ventilation is between LIP and UIP
4. The ARDSNet ARMA Trial (Landmark Study)
The NIH ARDS Clinical Trials Network published this pivotal RCT in 2000 (N ENGL J MED), enrolling 861 patients:
| Parameter | Low TV Arm | Traditional TV Arm |
|---|---|---|
| Tidal volume | 6 mL/kg PBW | 12 mL/kg PBW |
| Max Pplat | ≤30 cm H2O | <50 cm H2O |
| Mean Pplat | 25 cm H2O | 33 cm H2O |
| Mortality | 31% | 40% |
Result: 9% absolute mortality reduction - one of the most impactful results in critical care medicine. This established low tidal volume ventilation as the standard of care in ARDS.
5. The ARDSNet Low Tidal Volume Protocol (ARMA Protocol)
Part I: Ventilator Setup
- Calculate Predicted Body Weight (PBW):
- Males: 50 + 2.3 x [height (inches) - 60]
- Females: 45.5 + 2.3 x [height (inches) - 60]
- Mode: Assist/Control (Volume Control)
- Initial TV: 8 mL/kg PBW, reduce by 1 mL/kg every ≤2 hours
- Target TV: 6 mL/kg PBW (may go as low as 4 mL/kg if Pplat >30)
- RR: 6-35 breaths/min to achieve pH goals
- Inspiratory flow: >80 L/min; I:E ratio goal 1:1.0-1.3
Part II: Oxygenation Goal
Target: PaO2 = 55-80 mmHg or SpO2 = 88-95%
Use the FiO2-PEEP table (low PEEP table):
| FiO2 | 0.3 | 0.4 | 0.4 | 0.5 | 0.5 | 0.6 | 0.7 | 0.7 | 0.7 | 0.8 | 0.9 | 0.9 | 1.0 | 1.0 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PEEP | 5 | 5 | 8 | 8 | 10 | 10 | 10 | 12 | 14 | 14 | 14 | 18 | 20-24 | 24 |
Part III: Plateau Pressure Goal ≤30 cm H2O
- Check Pplat (0.5-second inspiratory pause) every 4 hours
- If Pplat >30: decrease TV by 1 mL/kg (minimum 4 mL/kg)
- If Pplat <25 and TV <6: increase TV by 1 mL/kg
Part IV: pH Goal 7.30-7.45
- Acidosis (pH <7.30): Increase RR (max 35/min) → consider NaHCO3 if pH <7.15
- Alkalosis (pH >7.45): Decrease RR if possible; avoid hyperventilation
6. PEEP - The Cornerstone of Alveolar Stabilization
PEEP (Positive End-Expiratory Pressure) prevents alveolar collapse between breaths, reducing atelectrauma. However, excessive PEEP causes overdistension and reduces cardiac output.
PEEP Titration Methods:
a) ARDSNet FiO2/PEEP Tables:
- Low PEEP table (see above) - default approach
- High PEEP table - for moderate-severe ARDS (P/F <200), starts PEEP at 12 when FiO2 = 0.5
b) Best Compliance Method (Bedside "Optimal PEEP"):
- Measure static compliance at each PEEP step
- Set PEEP at level giving highest compliance without hemodynamic compromise
c) P-V Curve Method:
- Set PEEP 2 cm H2O above the LIP on the static inspiratory P-V curve
d) Esophageal Pressure-Guided PEEP:
- Measures transpulmonary pressure (Ptp = Pairway - Pesophageal)
- Targets Ptp ≥0 at end expiration
- A phase 2 trial (EPVent-2) showed no benefit over empirical high PEEP titration
Key trial - ALVEOLI (ARDSNet, 2004): Compared high PEEP vs. low PEEP - no significant mortality difference in all-comers, but subgroups with moderate-severe ARDS showed trends toward benefit with higher PEEP.
7. Permissive Hypercapnia
Low tidal volumes result in reduced minute ventilation and CO2 retention. This is deliberately tolerated as long as:
- pH remains ≥7.20-7.25
- No contraindications (raised ICP, pulmonary hypertension, right heart failure)
Permissive hypercapnia is a critical component of lung-protective ventilation and must be distinguished from inadequate ventilation. PaCO2 may rise to 60-80 mmHg or higher; this is acceptable.
8. Adjunctive Strategies
A. Prone Positioning
Mechanism: Placing the patient prone:
- Recruits dorsal (dependent) atelectatic lung
- More homogeneous distribution of ventilation dorsal to ventral
- Reduces V/Q mismatch and improves PaO2/FiO2
- Reduces VILI by distributing stress/strain more evenly
Key Trial - PROSEVA (Guerin et al., 2013):
- 466 patients with ARDS, P/F <150 mmHg, enrolled within 36 hours
- Prone ≥16 hours/day vs. supine
- 28-day mortality: 16% (prone) vs. 32.8% (supine) - highly significant
- All patients on lung-protective ventilation + NMB
Indications: P/F <150 mmHg despite optimal supine ventilation, initiated early (<36-48 hrs)
Contraindications: Unstable spine, open abdomen, facial trauma, severe hemodynamic instability
Duration: At least 16 hours/day; continue until P/F >150 on FiO2 ≤0.6, PEEP ≤10 for 4 hours
B. Neuromuscular Blockade (NMB)
Rationale:
- Abolishes patient-ventilator dyssynchrony
- Reduces oxygen consumption
- Prevents breath stacking and high driving pressures
- Facilitates prone positioning
Key Trials:
- ACURASYS (Papazian et al., 2010): Cisatracurium for 48 hours in P/F <150 - 90-day mortality 31.6% vs. 40.7% - benefit significant only after covariate adjustment
- ROSE Trial (2019): Cisatracurium + heavy sedation vs. usual care (light sedation) in 1006 patients - 90-day mortality identical (~42.5% in both arms) - NMB provides no benefit when compared to protocolized light sedation alone
Current recommendation: Not routine. Use selectively for:
- Severe ventilator dyssynchrony despite adequate sedation
- To facilitate prone positioning
- Severe refractory hypoxemia
Drug of choice: Cisatracurium (Hofmann elimination, independent of liver/renal function)
C. Corticosteroids
Theoretical benefits: Anti-inflammatory, anti-fibrotic (targets proliferative phase of ARDS)
Potential harms: Secondary infections, hyperglycemia, delirium, neuromuscular weakness
Key Trials:
- LaSRS (ARDSNet, 2006): Methylprednisolone in persistent ARDS (7-21 days) - no mortality difference; patients enrolled after 14 days had WORSE mortality
- Dexamethasone RCT (2020): Dexamethasone in moderate-severe ARDS (P/F <200) - improved ventilator-free days; not definitively mortality-reducing
- COVID-RECOVERY trial: Dexamethasone 6 mg/day improved mortality in mechanically ventilated COVID-ARDS patients
Current recommendation:
- Avoid in late-phase ARDS (>14 days) - increased harm
- May be considered in early moderate-severe ARDS
- Use for underlying indications (CAP, septic shock, COVID)
D. Conservative Fluid Management
Rationale: Increased pulmonary vascular permeability in ARDS means even modest rises in left atrial filling pressure worsen pulmonary edema. Low filling pressures minimize edema, improve compliance, and shorten ventilator days.
FACTT Trial (ARDSNet): Conservative fluid management improved ventilator-free days and ICU-free days vs. liberal strategy, with no difference in 60-day mortality and no increase in renal failure.
Target: CVP 4-8 mmHg (or lowest tolerated without compromising perfusion). Use diuretics aggressively once hemodynamically stable.
E. Recruitment Maneuvers (RM)
Technique: Transient application of high CPAP (35-40 cm H2O for 30 seconds) to open collapsed alveoli, followed by elevated PEEP to maintain recruitment.
Evidence:
- No RCT demonstrates mortality benefit
- ART Trial (2017): RM + aggressive PEEP titration resulted in higher 28-day mortality (55.3%) vs. control (49.3%) and more barotrauma
Current recommendation: NOT routinely recommended. May be considered as salvage in severe refractory hypoxemia only.
F. Inhaled Vasodilators (Inhaled Nitric Oxide / Prostacyclin)
Mechanism: Selective pulmonary vasodilation of ventilated alveoli → diverts blood from shunt units → improves V/Q matching and PaO2.
Evidence: Consistently improves oxygenation (PaO2/FiO2). No RCT shows mortality benefit.
Use: Rescue therapy only, for severe refractory hypoxemia as a bridge (e.g., to prone positioning, NMB, or ECMO).
9. Modes of Ventilation in ARDS
| Mode | Role |
|---|---|
| Volume-Controlled AC (A/C) | Standard first-line mode; ensures consistent TV delivery |
| Pressure-Controlled Ventilation (PCV) | Useful when plateau pressures are difficult to control; TV varies with compliance |
| Airway Pressure Release Ventilation (APRV) | Maintains high mean airway pressure; allows spontaneous breathing; not proven superior to standard |
| High-Frequency Oscillatory Ventilation (HFOV) | Uses tiny tidal volumes at very high frequencies (3-15 Hz); OSCAR and OSCILLATE trials showed no benefit, possible harm; NOT recommended routinely |
| Pressure Support Ventilation (PSV) | Used during weaning; monitor for excessive patient effort and high spontaneous TV |
10. ECMO (Extracorporeal Membrane Oxygenation)
Indication: Severe refractory ARDS (P/F <80 despite optimal management), as rescue therapy
Types: Veno-venous ECMO (VV-ECMO) for respiratory failure
Key Trial - CESAR (2009): Referral to ECMO center improved survival (63% vs. 47%)
EOLIA Trial (2018): Early VV-ECMO in very severe ARDS (P/F <50) - 60-day mortality 35% (ECMO) vs. 46% (control); p=0.07 (not statistically significant, but post-hoc crossover analysis supports use as rescue)
Current status: Reserved for specialized centers as rescue therapy when conventional ventilation and prone positioning fail.
11. Driving Pressure - Emerging Concept
Driving Pressure (ΔP) = Pplat - PEEP = Tidal volume / Respiratory system compliance
- Represents the actual stress delivered to the lung with each breath
- A retrospective analysis by Amato et al. (NEJM 2015) showed ΔP >15 cm H2O was most strongly associated with increased mortality
- Target: ΔP <15 cm H2O
- Driving pressure-guided ventilation is increasingly used to individualize therapy
A 2024 meta-analysis [PMID: 38937217] confirmed that driving pressure-guided ventilation is associated with reduced postoperative pulmonary complications.
12. Summary Table: ARDSNet Ventilator Bundle
| Parameter | Target |
|---|---|
| Mode | Volume-Controlled A/C |
| Tidal volume | 6 mL/kg PBW (4-8 range) |
| Plateau pressure | ≤30 cm H2O |
| Driving pressure | <15 cm H2O |
| PEEP | Per FiO2/PEEP table; minimum 5, up to 24 cm H2O |
| FiO2 | Minimum to maintain SpO2 88-95% |
| PaO2 target | 55-80 mmHg |
| pH target | 7.30-7.45 |
| RR | Up to 35 breaths/min |
| Permissive hypercapnia | Tolerate PaCO2 up to 60-80 mmHg (if pH ≥7.20) |
| Prone positioning | If P/F <150, ≥16 hrs/day, early |
| NMB | Selective (dyssynchrony, prone facilitation) |
| Fluids | Conservative (CVP 4-8 mmHg) |
| HFOV/RM | Not recommended routinely |
| ECMO | Rescue for P/F <80 |
13. Complications of Mechanical Ventilation in ARDS
- Ventilator-Induced Lung Injury (VILI) - prevented by above strategies
- Ventilator-Associated Pneumonia (VAP) - head-of-bed elevation 30°, oral care bundles
- Barotrauma - pneumothorax, pneumomediastinum (limit Pplat)
- Hemodynamic compromise - high PEEP reduces venous return and cardiac output
- Oxygen toxicity - minimize FiO2; avoid prolonged FiO2 >0.6
- ICU-acquired weakness - minimize NMB, early mobilization
14. Weaning from Mechanical Ventilation
Attempt daily Spontaneous Breathing Trial (SBT) when:
- Underlying cause of ARDS is improving
- FiO2 ≤0.4 and PEEP ≤8 cm H2O
- Hemodynamically stable (no/minimal vasopressors)
- Patient awake and cooperative (RASS 0 to -1)
Use PS 5-8 cm H2O + PEEP 5 for 30-120 min SBT. Extubate if tolerating.
Key Points for Exam
- 6 mL/kg PBW tidal volume is the single most important intervention - reduces mortality by ~9% (ARMA trial)
- PBW, not actual body weight, is used for TV calculation
- Plateau pressure (not peak pressure) ≤30 cm H2O
- Permissive hypercapnia is intentional and acceptable
- Prone positioning (PROSEVA) halves mortality in P/F <150 - must be ≥16 hrs/day
- HFOV and routine recruitment maneuvers are harmful - contraindicated
- Driving pressure <15 cm H2O is an emerging independent predictor of outcome
- ECMO is rescue therapy only (P/F <80, severe refractory ARDS)
- Conservative fluid management shortens ventilator days (FACTT trial)
- NMB is NOT routine (ROSE trial shows no benefit over light sedation)
Sources: Fishman's Pulmonary Diseases and Disorders, 6e; Harrison's Principles of Internal Medicine 22e (2025); Murray & Nadel's Textbook of Respiratory Medicine; Miller's Anesthesia 10e; Goldman-Cecil Medicine; Current Surgical Therapy 14e
just give answer from studies not whole study now combine and make an answer
Here is the combined, study-evidence-based answer on ventilator strategy for ARDS:
Ventilator Strategy for ARDS - Evidence-Based Answer
1. Low Tidal Volume Ventilation (The Foundation)
ARDSNet ARMA Trial (2000) - 861 patients, the landmark RCT:
- 6 mL/kg PBW vs. 12 mL/kg PBW
- Plateau pressure (Pplat) kept ≤30 cm H2O
- Result: Mortality reduced from 40% → 31% (9% absolute reduction)
- Also reduced ventilator-free days
- Conclusion: 6 mL/kg PBW is the standard of care
Permissive hypercapnia is accepted (PaCO2 up to 60-80 mmHg; tolerate pH ≥7.20). PaO2 target: 55-80 mmHg or SpO2 88-95% - deliberate acceptance of moderate hypoxemia to avoid high FiO2 toxicity.
2. PEEP Titration
ARDSNet ALVEOLI Trial (2004) - High PEEP vs. Low PEEP table:
- No significant mortality difference in all-comers
- High PEEP trend toward benefit in moderate-severe ARDS (P/F <200)
EPVent-2 Trial - Esophageal pressure-guided PEEP vs. empirical high PEEP:
- No benefit of esophageal-guided strategy over empirical titration
- Conclusion: ARDSNet FiO2/PEEP table remains the practical standard
3. Prone Positioning
PROSEVA Trial (Guerin, 2013) - 466 patients, P/F <150 mmHg, enrolled within 36 hours:
- Prone ≥16 hours/day vs. supine
- 28-day mortality: 16% (prone) vs. 32.8% (supine) - statistically significant halving of mortality
- All patients were on lung-protective ventilation + neuromuscular blockade
- Conclusion: Prone positioning for ≥16 hrs/day is mandatory in P/F <150
Prior meta-analysis confirmed benefit specifically in severe ARDS (P/F <100); no benefit in mild ARDS.
4. Neuromuscular Blockade (NMB)
ACURASYS Trial (Papazian, 2010) - Cisatracurium 48 hrs in P/F <150:
- 90-day mortality: 31.6% (cisatracurium) vs. 40.7% (placebo)
- Statistically significant only after covariate adjustment
- Suggested benefit - widely adopted
ROSE Trial (2019) - 1006 patients; cisatracurium + heavy sedation vs. light sedation alone:
- 90-day mortality: 42.5% vs. 42.8% - no difference
- Conclusion: Routine NMB has no benefit over protocolized light sedation
- Selective use only: ventilator dyssynchrony, facilitating prone positioning
5. Recruitment Maneuvers
ART Trial (2017) - RM + aggressive PEEP titration vs. conventional low PEEP:
- 28-day mortality: 55.3% (RM group) vs. 49.3% (control) - HIGHER in RM group
- Increased barotrauma and hypotension
- Conclusion: Routine recruitment maneuvers are HARMFUL - not recommended
6. High-Frequency Oscillatory Ventilation (HFOV)
OSCAR Trial (UK, 2013) and OSCILLATE Trial (Canada, 2013):
- HFOV vs. conventional lung-protective ventilation
- OSCILLATE stopped early: in-hospital mortality 47% (HFOV) vs. 35% (control)
- Conclusion: HFOV is NOT recommended in adult ARDS - may cause harm
7. Fluid Management
FACTT Trial (ARDSNet) - Conservative vs. liberal fluid strategy:
- Conservative strategy: more ventilator-free days (+2.5 days) and ICU-free days (+2.2 days)
- No difference in 60-day mortality; no increase in renal failure
- Conclusion: Conservative fluid management (CVP 4-8 mmHg) shortens mechanical ventilation duration
8. Corticosteroids
LaSRS (ARDSNet, 2006) - Methylprednisolone in persistent ARDS (7-21 days):
- No mortality benefit; patients enrolled after 14 days had significantly HIGHER mortality
- Conclusion: Steroids contraindicated in late ARDS (>14 days)
Dexamethasone RCT (Villar, 2020) - Dexamethasone in P/F <200:
- Improved ventilator-free days; 60-day mortality 21% vs. 36%
- Conclusion: Early dexamethasone may benefit moderate-severe ARDS
RECOVERY Trial (COVID, 2020) - Dexamethasone 6 mg/day in ventilated patients:
- Mortality reduced by ~35% in mechanically ventilated patients
- Conclusion: Dexamethasone is standard in COVID-ARDS and likely benefits ARDS from other causes
9. Driving Pressure
Amato et al. (NEJM, 2015) - Retrospective analysis of 3562 patients across 9 RCTs:
- Driving pressure (ΔP = Pplat - PEEP) >15 cm H2O was the variable most strongly associated with mortality
- More predictive than TV or Pplat alone
- Conclusion: Target ΔP <15 cm H2O; individualize ventilation to minimize driving pressure
10. ECMO
CESAR Trial (2009, UK) - Referral to ECMO center vs. conventional management:
- Survival without disability: 63% vs. 47%
EOLIA Trial (2018) - Early VV-ECMO in P/F <50 vs. conventional:
- 60-day mortality: 35% vs. 46%; p = 0.07 (not significant)
- 28% of control group crossed over to ECMO as rescue - confounded results
- Post-hoc Bayesian analysis: 96% probability of benefit
- Conclusion: ECMO is rescue therapy for P/F <80 despite all optimal strategies; refer to specialized centers early
Combined Evidence-Based Protocol Summary
| Strategy | Trial | Recommendation |
|---|---|---|
| TV 6 mL/kg PBW | ARMA (2000) | First-line - reduces mortality 9% |
| Pplat ≤30 cm H2O | ARMA (2000) | Mandatory with low TV |
| Driving pressure <15 | Amato (2015) | Target in all patients |
| PEEP per FiO2 table | ALVEOLI (2004) | Standard PEEP titration |
| Prone ≥16 hrs if P/F <150 | PROSEVA (2013) | Mandatory in moderate-severe ARDS |
| Conservative fluids | FACTT | Shorten ventilator days |
| NMB - selective only | ROSE (2019) | Not routine |
| Steroids (early, moderate-severe) | Villar (2020) | Consider dexamethasone |
| Recruitment maneuvers | ART (2017) | Do NOT use routinely |
| HFOV | OSCAR/OSCILLATE (2013) | Do NOT use |
| ECMO (rescue) | CESAR/EOLIA | P/F <80, specialized centers |
The single most important message from all the evidence: Low tidal volume (6 mL/kg PBW) ventilation combined with early prone positioning for moderate-severe ARDS (P/F <150) represents the only two interventions with robust, replicated mortality benefit in ARDS.
This is a shared conversation. Sign in to Orris to start your own chat.