What should we do for crashing BP and ECG shows VT
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is the full management approach for VT with crashing BP, synthesized from Braunwald's Heart Disease, Goldman-Cecil Medicine, and Tintinalli's Emergency Medicine:
VT with Hemodynamic Instability (Crashing BP)
Step 1: Immediate - Electrical Cardioversion (Do NOT wait for drugs)
This is a TIME-CRITICAL emergency. Electricity first.
| VT Type | Shock Type | Energy |
|---|---|---|
| VT with pulse + crashing BP | Synchronized cardioversion | Start 100-200 J biphasic |
| Pulseless VT / VT degenerating to VF | Unsynchronized defibrillation | 200 J biphasic immediately |
| Polymorphic VT (irregular) | Unsynchronized shock | 200 J biphasic |
- If the patient is conscious, sedate first (e.g., midazolam + ketamine) before synchronized cardioversion, if time allows.
- Do NOT delay the shock waiting for sedation if the patient is losing consciousness.
"QRS synchronous electrical cardioversion should be performed in case of impaired consciousness, hypotension, or pulmonary edema, after sedation if possible if the patient is conscious." - Braunwald's Heart Disease
Step 2: Simultaneous Resuscitation
While preparing for shock (or if shock temporarily restores rhythm):
- IV access x 2, continuous ECG monitoring
- High-flow oxygen, secure airway if obtunded
- Call for crash cart/defibrillator immediately
- Start CPR if pulseless at any point
Step 3: Post-Cardioversion / If Temporarily Stable - Antiarrhythmic Drugs
Once sinus rhythm is restored, give antiarrhythmics to prevent recurrence:
Drug Options (in order of evidence):
-
Amiodarone - 150 mg IV over 10 minutes (loading), then 1 mg/min x 6 hours, then 0.5 mg/min
- Better at preventing recurrence (more effective at slower rates)
- Can cause hypotension - watch BP
-
Procainamide - 10 mg/kg IV (up to 1000 mg) over 20 minutes
- Superior to amiodarone for acutely terminating wide-complex tachycardia in randomized trials
- Avoid in renal failure (metabolite causes QT prolongation and Torsades)
- Also a vasodilator - can worsen hypotension in up to 30% of patients
-
Lidocaine - 50 mg IV bolus (1-1.5 mg/kg)
- More effective at faster heart rates
- Good in acute ischemia/MI-related VT
- Less effective for preventing recurrence
Step 4: Find and Fix the Cause
| Precipitant | Action |
|---|---|
| Hypokalemia | Aggressive K+ replacement (target K+ >4.0) |
| Hypomagnesemia | IV MgSO4 2g over 10 min |
| Hypoxia | Correct with supplemental O2 or intubation |
| Acidosis | Sodium bicarbonate if severe metabolic acidosis |
| Acute MI | Urgent ECG, troponin, cath lab activation |
| Heart failure | Diuretics, inotropes as needed |
| Drug toxicity (QT prolongation) | Stop offending drug |
"The most important factors in preventing early recurrence are the prompt identification and reversal of any precipitating causes." - Goldman-Cecil Medicine
Step 5: If VT Keeps Coming Back (Electrical Storm)
Defined as ≥3 episodes of VT/VF in 24 hours requiring shocks:
- Esmolol 500 mcg/kg IV bolus, then 50-200 mcg/kg/min infusion (preferred - short half-life beta-blocker)
- Continue amiodarone infusion
- Consider intra-aortic balloon pump for hemodynamic support
- Treat ischemia - reperfusion if coronary occlusion
- Catheter ablation if refractory to all the above
Critical Warnings
- Do NOT give IV verapamil or diltiazem for VT (unless you are 100% certain it is idiopathic fascicular VT in a structurally normal heart) - can cause irreversible hemodynamic collapse
- Adenosine can be used diagnostically for stable wide-complex tachycardia of uncertain origin, but only in a hemodynamically stable patient
- Magnesium is specifically for Torsades de Pointes (polymorphic VT with long QT) - give 2g IV over 1-2 minutes
Bottom line: VT + crashing BP = synchronized cardioversion immediately (or unsynchronized if pulseless). Drugs come after. Fix the underlying cause to prevent recurrence.
- Braunwald's Heart Disease, p. 556
- Goldman-Cecil Medicine, p. 590
- Tintinalli's Emergency Medicine, p. 145
How to diagnose polymorphic VT in ECG
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a complete guide to diagnosing Polymorphic VT on ECG, sourced from Harrison's, Tintinalli's, and Rosen's Emergency Medicine:
ECG Diagnosis of Polymorphic VT (PMVT)
Core ECG Features
| Feature | Polymorphic VT | Monomorphic VT (for comparison) |
|---|---|---|
| QRS morphology | Continuously changing beat to beat | Consistent, same shape every beat |
| Electrical axis | Shifting / undulating | Fixed |
| Rhythm | Rapid and irregular | Rapid and regular |
| QRS width | Wide (>100-120 ms) | Wide (>100-120 ms) |
| Rate | 140-300 bpm | Usually 140-180 bpm |
| P waves | None (or rare dissociated P waves) | None (or rare dissociated P waves) |
| R-R interval | Variable/inconsistent | Regular |
"Polymorphic VT has a continually changing QRS morphology indicating a changing ventricular activation sequence." - Harrison's Principles of Internal Medicine 22E
Real ECG Examples
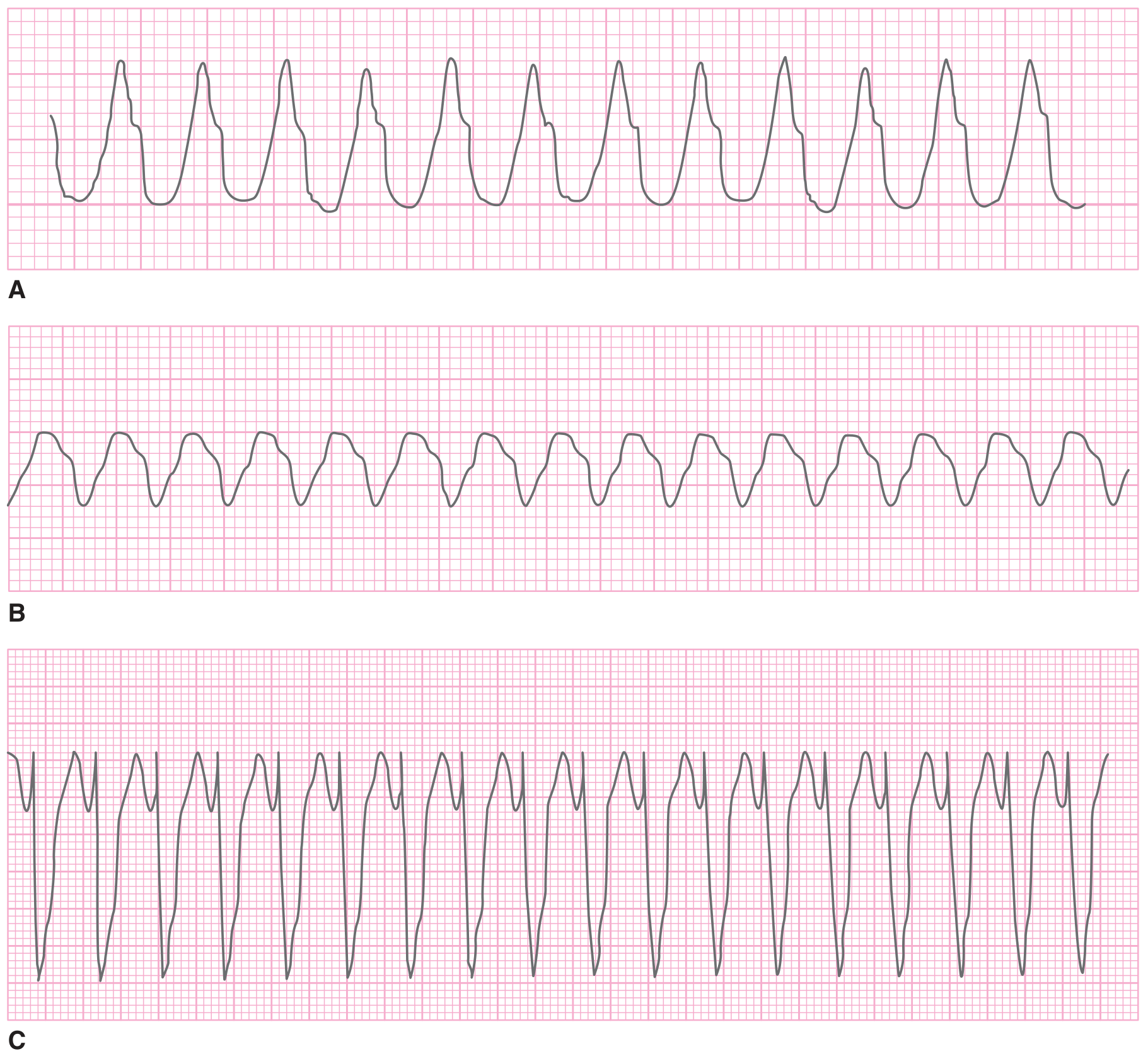
Monomorphic VT (A, B, C) - notice consistent QRS shape every beat:
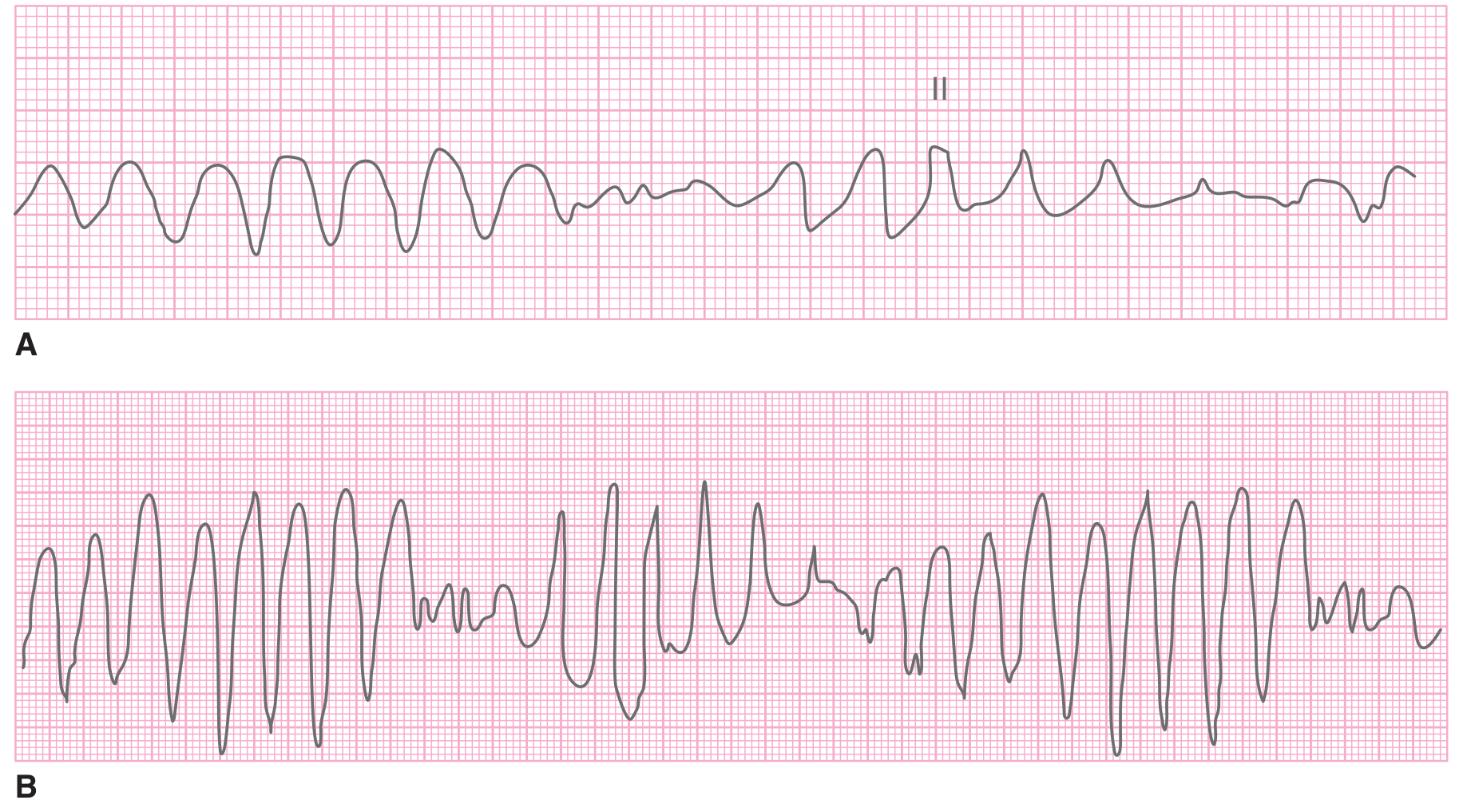
Polymorphic VT (A) vs Torsades de Pointes (B):
The Two Subtypes of Polymorphic VT
1. Polymorphic VT WITHOUT QT Prolongation
- QRS changes randomly and chaotically in shape, amplitude, and axis
- Baseline (sinus rhythm) ECG shows normal QT interval
- Occurs in: acute MI/ischemia, structural heart disease, catecholaminergic PMVT
- Key trigger: Ischemia, adrenergic surge
2. Torsades de Pointes (TdP) - PMVT WITH QT Prolongation
This is the "classic" named subtype and has specific diagnostic criteria:
Diagnostic Criteria (Rosen's Emergency Medicine):
- Ventricular rate >200 beats/min
- Undulating QRS axis - the polarity of the complexes appears to shift around the baseline (the "twisting of the points")
- Paroxysms typically <90 seconds in duration (often self-terminating)
- On the preceding sinus beats: prolonged QT interval (>450 ms in males, >470 ms in females)
The "Twisting" Pattern:
- QRS complexes appear to rotate around the isoelectric baseline
- Amplitude gradually increases then decreases in a cyclical, sinusoidal fashion
- Best seen in a single continuous rhythm strip
How to Identify TdP on ECG - Step by Step
- Look at the rhythm strip - see wide, fast, chaotic complexes
- Is the QRS morphology changing beat to beat? → Yes = PMVT
- Is there a spindle/waxing-waning pattern? - complexes appear to "twist" around the baseline → suggests TdP
- Go back to the sinus beats BEFORE the episode - is the QT prolonged?
- Look for the "short-long-short" initiating sequence - TdP is often triggered by a PVC following a long R-R pause (pause-dependent mechanism)
Causes to Look for After Diagnosis
| Type | Causes |
|---|---|
| PMVT (normal QT) | Acute MI, ischemia, Brugada syndrome, catecholaminergic PMVT (CPVT) |
| TdP (prolonged QT) | Drugs (antiarrhythmics Class IA/III, antipsychotics, antibiotics like azithromycin/fluoroquinolones, methadone), electrolytes (↓K+, ↓Mg2+, ↓Ca2+), congenital Long QT syndrome, bradycardia/complete heart block |
Key Clinical Point: TdP vs VF
- TdP - recognizable organized "twisting" pattern, usually self-terminates, then recurs
- VF - completely chaotic, no discernible QRS, no organized pattern at all
- TdP can degenerate into VF if sustained
Treatment Reminder (Based on Diagnosis)
-
PMVT with normal QT (ischemic) - cardioversion + treat ischemia; beta-blockers
-
TdP - IV MgSO₄ 2g immediately (even if Mg is normal); correct K+; stop QT-prolonging drugs; overdrive pacing if bradycardia-dependent; avoid Class IA/IC antiarrhythmics (they worsen QT prolongation)
-
Tintinalli's Emergency Medicine, p. 156-157
-
Harrison's Principles of Internal Medicine 22E, p. ~1248
-
Rosen's Emergency Medicine, p. 1063
Torsedes de pointes
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
Loading Image
Here is a complete, textbook-level reference on Torsades de Pointes:
Torsades de Pointes (TdP)
What It Is
The name is French for "twisting of the points" - it describes a specific subtype of polymorphic VT where the QRS complexes appear to spiral/twist around the isoelectric baseline. It always occurs in the context of a prolonged QT interval.
Classic ECG Appearance

ECG Features - Diagnostic Criteria:
| Feature | Description |
|---|---|
| Rate | >200 beats/min |
| QRS morphology | Wide, undulating axis - polarity shifts around the baseline in a spindle/waxing-waning pattern |
| Rhythm | Irregular |
| Duration | Paroxysms typically <90 seconds (often self-terminating, but recurs) |
| Preceding sinus beats | Prolonged QT interval (QTc >450 ms men / >470 ms women) |
| Initiation | Classic "short-long-short" R-R sequence - triggered by a PVC after a long pause |
Mechanism
TdP is triggered by Early Afterdepolarizations (EADs):
- Prolonged QT = prolonged action potential phase 2/3
- During this prolonged repolarization window, abnormal Ca²⁺ and late Na⁺ influx generate EADs
- EADs reach threshold and trigger an ectopic beat (usually the initiating PVC)
- This sets up a reentrant circuit with constantly shifting activation wavefronts → the "twisting" appearance
Two Types: Acquired vs Congenital
Type 1: Acquired (Pause-Dependent) - MOST COMMON
Triggered by slow heart rate / pauses. QT prolongs with bradycardia, creating the window for EADs.
Causes:
| Category | Examples |
|---|---|
| Drugs (most common) | Class IA antiarrhythmics: quinidine, procainamide, disopyramide |
| Class III: sotalol, amiodarone (rare), dofetilide, ibutilide | |
| Antipsychotics: haloperidol, droperidol, thioridazine, quetiapine | |
| Tricyclic antidepressants | |
| Macrolide antibiotics: azithromycin, clarithromycin, erythromycin | |
| Fluoroquinolones: moxifloxacin | |
| Antifungals: fluconazole, ketoconazole | |
| Antihistamines, antiemetics (domperidone, ondansetron), antiseizure drugs | |
| Methadone | |
| Electrolytes | Hypokalemia, hypomagnesemia, hypocalcemia |
| Systemic | Bradycardia/AV block, hypothyroidism, starvation/low protein diet, cerebrovascular accident |
| Myocardial ischemia |
Type 2: Congenital (Adrenergic-Dependent) - triggered by exercise/emotion
| Syndrome | Inheritance | Gene Defect |
|---|---|---|
| Romano-Ward syndrome | Autosomal dominant | KCNQ1, KCNH2, SCN5A (LQT1, LQT2, LQT3) |
| Jervell and Lange-Nielsen syndrome | Autosomal recessive | KCNQ1 (with congenital deafness) |
- Women are at greater risk than men for TdP due to naturally longer QTc
Clinical Features
- Episodes of palpitations, dizziness, presyncope, syncope
- Often self-terminates (<90 seconds) then recurs repeatedly
- Can degenerate into VF and sudden cardiac death
- Patients may present with recurrent "blackouts" that are misdiagnosed as seizures
Treatment
Acute Management
| Step | Action |
|---|---|
| 1. IV Magnesium Sulfate | 1-2 g IV over 5-15 minutes (first-line even if serum Mg is normal) - stabilizes the membrane |
| 2. Correct electrolytes | Target K⁺ >4.5 mEq/L, Mg²⁺ >2 mEq/L |
| 3. Stop the offending drug | Identify and remove any QT-prolonging medications immediately |
| 4. Increase heart rate | Rate of 100-120 bpm shortens QT interval and prevents recurrence |
| - | Isoproterenol infusion (beta-agonist): increases heart rate, shortens QTc - used for acquired/pause-dependent TdP |
| - | Temporary overdrive pacing (transcutaneous or transvenous at 100-120 bpm): most reliable way to increase rate and suppress TdP |
| 5. Cardioversion | For sustained TdP / hemodynamically unstable - unsynchronized shock (synchronization may not be possible) |
Drugs to AVOID in TdP
- Class IA antiarrhythmics (quinidine, procainamide, disopyramide) - prolong QT further
- Class IC (flecainide, propafenone)
- Amiodarone (lengthens QT, use with caution)
Long-Term Management
| Situation | Treatment |
|---|---|
| Acquired TdP | Remove precipitant; replete K⁺ & Mg²⁺ |
| Congenital LQTS | Beta-blockers (nadolol, atenolol, metoprolol) - first-line for LQT1 and LQT2 |
| Breakthrough on beta-blocker (~25%) | ICD |
| High-risk refractory cases | Left cardiac sympathetic denervation (LCSD) |
| Aborted cardiac arrest | ICD regardless |
"An ICD is recommended for patients who present with aborted cardiac arrest. About 25% of patients continue to experience ventricular arrhythmias on full doses of beta-blocker therapy and require an ICD." - Goldman-Cecil Medicine
Key Points to Remember
- QT prolongation is the substrate - always check QTc on the prior ECG
- Mg first, always - even if serum Mg is normal
- Isoproterenol for acquired/pause-dependent TdP; beta-blockers for congenital LQTS (opposite treatments!)
- Never give Class IA/IC drugs - they make it worse
- Short-long-short initiating pattern is pathognomonic
- Women > men for risk; concurrent QT-prolonging drugs multiply risk dramatically
- Rosen's Emergency Medicine, p. 1063
- Goldman-Cecil Medicine, p. 590-591
- Lippincott Pharmacology
- Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.