Ischemic heart disease detail 10 mark answer medicine mbbs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive 10-mark MBBS answer. Let me compose the full answer:
Ischemic Heart Disease (IHD) - 10 Mark Answer
Definition
Ischemic heart disease (IHD) is a broad clinical syndrome caused by an imbalance between myocardial oxygen supply and demand, most commonly due to atherosclerotic obstruction of the coronary arteries. It is the leading cause of mortality worldwide, accounting for approximately 7.5 million deaths per year.
IHD is synonymous with coronary artery disease (CAD) in over 90% of cases.
Etiology / Risk Factors
Primary cause: Coronary atherosclerosis (>90% of cases)
Modifiable risk factors:
- Hypertension
- Dyslipidemia (raised LDL, low HDL)
- Diabetes mellitus
- Cigarette smoking
- Obesity and sedentary lifestyle
Non-modifiable risk factors:
- Age (males >45 yrs, females >55 yrs)
- Male sex
- Family history of premature CAD
Other causes of ischemia (non-atherosclerotic):
- Increased demand: tachycardia, hypertension, hypertrophy
- Decreased supply: hypotension, anemia, carbon monoxide poisoning, coronary vasospasm (Prinzmetal angina), vasculitis, embolism
Pathogenesis
IHD results from two key mechanisms:
1. Fixed (Chronic) Atherosclerotic Stenosis
- Stenosis of <70% lumen is typically asymptomatic
- >70% occlusion = "critical stenosis" - causes exertional angina (stable angina)
- >90% occlusion - may cause symptoms even at rest
- Clinically significant plaques occur in the first few cm of LAD, LCX, and along the RCA
- Slow progressive occlusion allows collateral circulation to develop, potentially preventing infarction
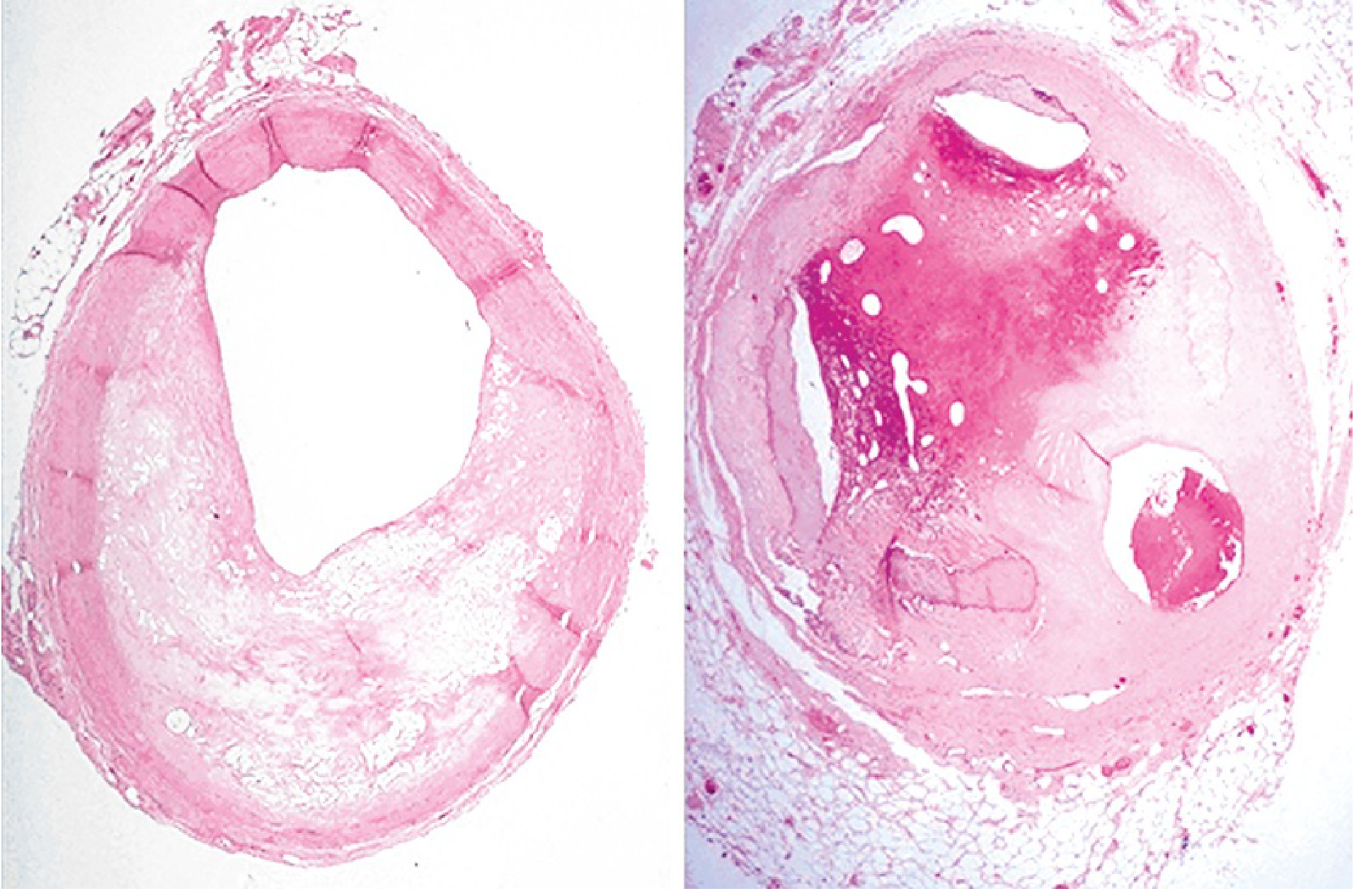
2. Acute Plaque Change (ACS trigger)
- Sudden plaque rupture, fissure, or erosion exposes thrombogenic subendothelial contents
- Triggers rapid platelet aggregation and thrombus formation
- Hemorrhage into plaque core can acutely expand the lesion
- Coronary vasospasm worsens luminal narrowing and can precipitate plaque disruption
- Vasospasm is triggered by: circulating adrenergic agonists, platelet products, imbalance of NO/endothelin, perivascular inflammatory mediators
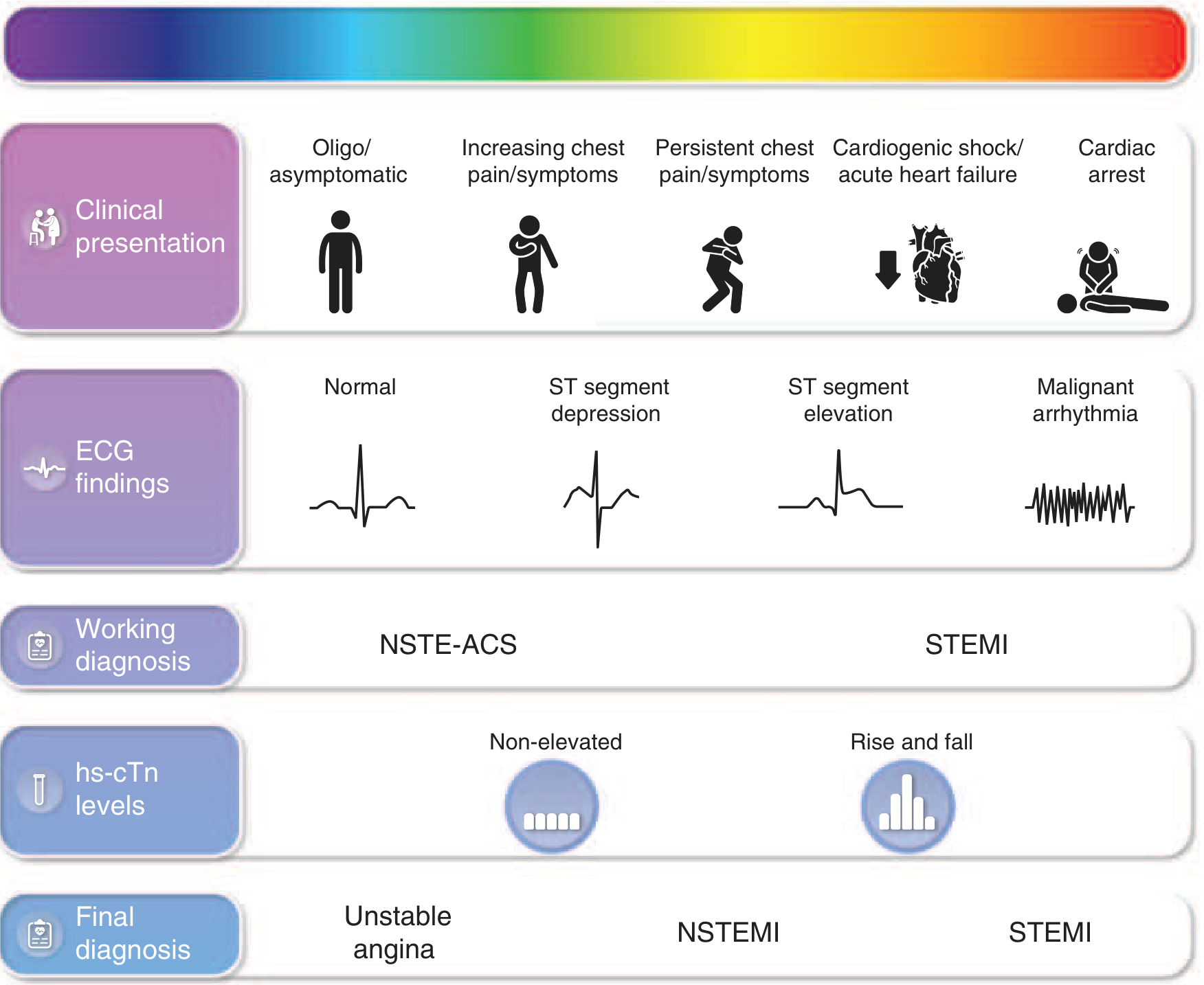
Clinical Syndromes of IHD
| Syndrome | Mechanism | Key Feature |
|---|---|---|
| Stable angina | >70% fixed stenosis | Predictable exertional chest pain, relieved by rest/nitrates |
| Unstable angina | Plaque erosion/rupture + non-occlusive thrombus | Increasing pain at lower thresholds or at rest |
| NSTEMI | Partial/transient occlusion - subendocardial infarct | Troponin rise, no ST elevation |
| STEMI | Complete occlusion - transmural infarct | ST elevation, Q waves develop |
| Sudden cardiac death | Lethal ventricular fibrillation from ischemic irritability | Often first manifestation; 80-90% of pre-hospital deaths |
| Chronic IHD / Ischemic cardiomyopathy | Accumulated ischemic injury | Progressive CHF after multiple infarcts |
The term Acute Coronary Syndrome (ACS) covers unstable angina, NSTEMI, and STEMI collectively.
Pathology of Myocardial Infarction
Cellular Sequence of Events:
- Seconds: Aerobic metabolism ceases; ATP falls; lactic acid accumulates
- Minutes: Loss of contractility (reversible)
- 20-40 minutes: Irreversible myocyte death (coagulative necrosis)
- Earliest sign: Disruption of sarcolemmal membrane - intracellular proteins (troponins, CK-MB) leak into bloodstream
Zone of Injury:
- Irreversible injury first appears in the subendocardial zone (most susceptible - last to receive blood, highest intramural pressure)
- With prolonged ischemia, necrosis advances as a "wavefront" toward epicardium (driven by edema, ROS, inflammatory mediators)
Histological Changes Over Time:
| Timing | Gross Finding | Microscopic Finding |
|---|---|---|
| 0-4 hrs | None (may be normal) | None visible (early: wavy fibers) |
| 4-12 hrs | Dark mottling | Coagulation necrosis begins; edema |
| 12-24 hrs | Dark mottling | Pyknosis of nuclei; contraction bands |
| 1-3 days | Yellow-tan pallor with hyperemic border | Neutrophil infiltration; coagulative necrosis |
| 3-7 days | Yellow-tan softening | Macrophage infiltration; phagocytosis begins |
| 1-3 weeks | Red-grey borders; yellow center | Granulation tissue ingrowth; fibroblasts |
| >2 months | White fibrous scar | Dense collagen scar (complete) |
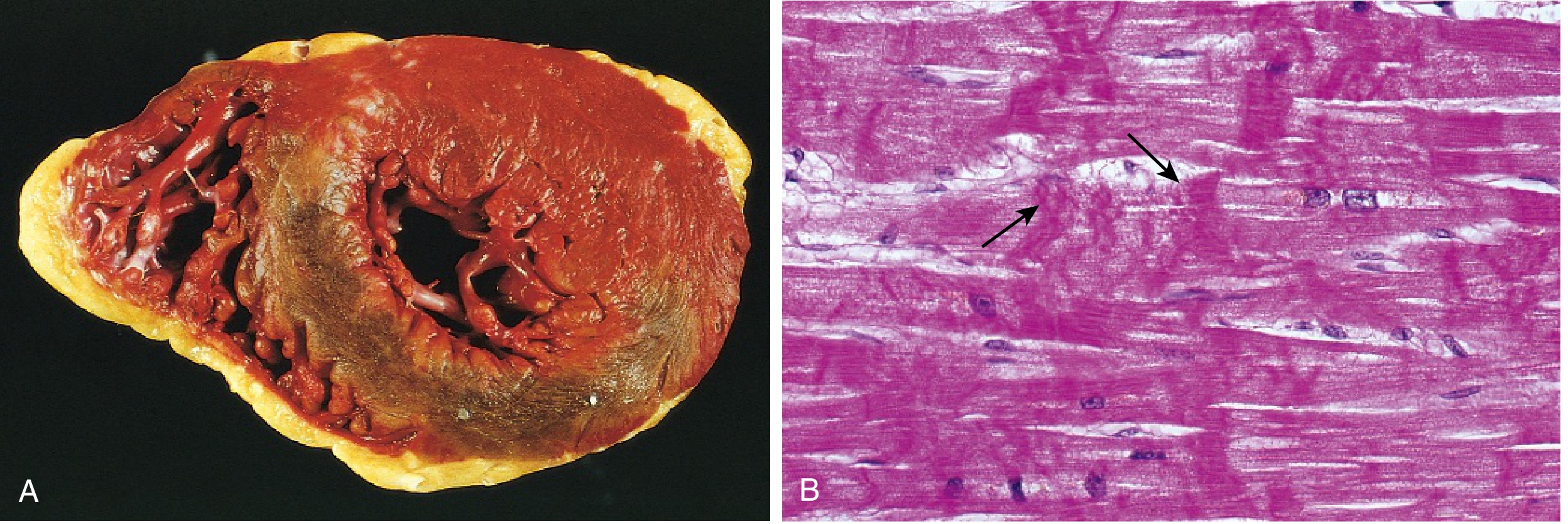
Reperfused Infarction:
- Hemorrhagic (due to vascular damage in reperfused zone)
- Shows contraction band necrosis microscopically - intense eosinophilic bands from calcium-induced hypercontracted sarcomeres fixed in tetanic state
Clinical Features of Acute MI
- Chest pain: Severe, crushing, substernal; radiates to neck, jaw, epigastrium, or left arm; lasts minutes to hours; NOT relieved by nitrates or rest
- Silent MI (~25%): Common in diabetics (autonomic neuropathy) and the elderly
- Other features: Diaphoresis, nausea/vomiting (especially posterior wall MI), dyspnea, tachycardia, weak pulse
- Cardiogenic shock: Develops if >40% of LV is infarcted
Investigations
ECG:
- STEMI: ST elevation in territory of affected artery; followed by Q wave development
- NSTEMI: ST depression or T wave inversion; no Q waves
- Unstable angina: May be normal or have transient changes; troponin negative
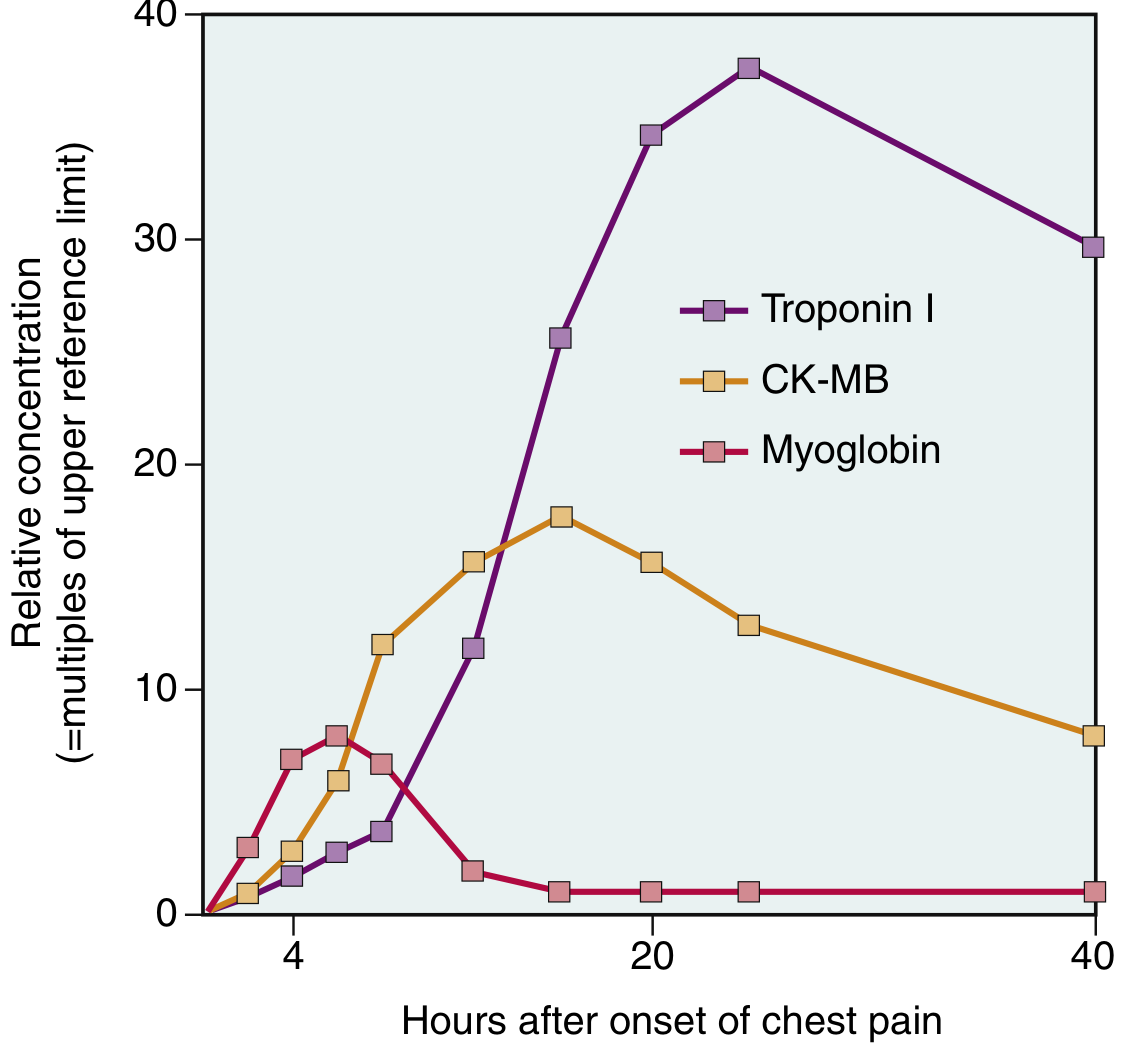
Cardiac Biomarkers (order of appearance):
| Marker | Rise | Peak | Return to Normal | Notes |
|---|---|---|---|---|
| Troponin I/T | 3-6 hrs | 24-48 hrs | 7-10 days | Highest specificity and sensitivity |
| CK-MB | 3-6 hrs | 24 hrs | 2-3 days | Good for reinfarction detection |
| Myoglobin | 1-3 hrs | 4-6 hrs | 24 hrs | First to rise; not cardiac-specific |
| LDH | 24-48 hrs | 3-6 days | 8-14 days | Elevated late |
Troponins T and I have the highest specificity and sensitivity for myocardial damage.
Other Investigations:
- Echocardiography: wall motion abnormalities
- Coronary angiography: defines anatomy, guides PCI
- Chest X-ray: pulmonary edema, cardiac enlargement
Complications of MI (Mnemonic: DREAD)
Early (within days):
- Arrhythmias (most common cause of early death; VF is most lethal)
- Cardiogenic shock (>40% LV involvement)
- Acute mitral regurgitation (papillary muscle rupture, 3-5 days)
- Ventricular free wall rupture (3-7 days - cardiac tamponade)
- Ventricular septal defect (septal rupture)
- Mural thrombus (with risk of systemic embolism)
Late:
- Pericarditis (Dressler syndrome - weeks later, autoimmune)
- Ventricular aneurysm (thin scarred wall, persistent ST elevation)
- Chronic heart failure / ischemic cardiomyopathy
Management
Immediate (within minutes of presentation):
- MONA: Morphine, Oxygen, Nitrates, Aspirin
- Antiplatelet: Aspirin 300 mg loading + P2Y12 inhibitor (clopidogrel/ticagrelor)
- Anticoagulation: Heparin or LMWH
Reperfusion (for STEMI - time is muscle):
- Primary PCI (percutaneous coronary intervention): Treatment of choice within 90 min of first medical contact; balloon angioplasty + stent
- Thrombolysis (fibrinolytics): If PCI not available within 120 min; use streptokinase or tPA (tissue plasminogen activator); contraindicated in recent surgery, bleeding risk, severe hypertension
Medical Therapy (ABCDE):
- A - Aspirin + ACE inhibitor (reduces remodeling, mortality)
- B - Beta-blockers (reduce heart rate, infarct size, arrhythmia risk)
- C - Cholesterol-lowering (high-intensity statins)
- D - Diabetes/Diet management
- E - Exercise (cardiac rehabilitation)
Surgical:
- CABG (coronary artery bypass graft surgery): For multivessel disease, left main stenosis, or failed PCI
Prognosis
- ~800,000 Americans have MI annually; ~50% die
- Mortality has fallen 50% since 1963 due to risk factor control, aspirin, CCUs, PCI, thrombolysis
- Worse prognosis: large infarct, reduced EF, VT/VF, cardiogenic shock, diabetes, advanced age
- Early reperfusion is the single most important factor determining outcome
Summary Table
| Feature | Stable Angina | Unstable Angina | NSTEMI | STEMI |
|---|---|---|---|---|
| Troponin | Normal | Normal | Elevated | Elevated |
| ECG | Normal/ST changes | Transient ST/T changes | ST depression | ST elevation |
| Plaque | Fixed stenosis >70% | Rupture + non-occlusive thrombus | Partial occlusion | Complete occlusion |
| Infarct depth | None | None | Subendocardial | Transmural |
| Management | Medical | Medical + urgent angiography | PCI within 24-72h | Primary PCI or thrombolysis |
Sources: Robbins & Kumar Basic Pathology, 10th ed. | Braunwald's Heart Disease, 12th ed.
Give me more details
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have all the deep content needed. Here is the full expanded answer:
Ischemic Heart Disease (IHD) - Detailed MBBS Answer
1. DEFINITION AND OVERVIEW
Ischemic Heart Disease (IHD) is a spectrum of clinical syndromes resulting from an imbalance between myocardial oxygen/nutrient supply and demand, most commonly due to atherosclerotic obstruction of the coronary arteries. It remains the leading cause of mortality worldwide, responsible for approximately 7.5 million deaths per year.
IHD is essentially synonymous with Coronary Artery Disease (CAD) in >90% of cases. The remaining cases result from vasospasm, vasculitis, embolism, hypotension, anemia, or carbon monoxide poisoning causing demand-supply mismatch.
2. ETIOLOGY AND RISK FACTORS
Primary Cause: Coronary Atherosclerosis
Risk Factors:
| Modifiable | Non-Modifiable |
|---|---|
| Hypertension | Age (M >45 yrs, F >55 yrs) |
| Dyslipidemia (high LDL, low HDL) | Male sex |
| Diabetes mellitus | Family history of premature CAD |
| Cigarette smoking | Genetic predisposition |
| Obesity (BMI >30) | - |
| Sedentary lifestyle | - |
| Metabolic syndrome | - |
| Chronic kidney disease | - |
Note: The epidemic of obesity sweeping both high-income and low/middle-income countries is driving a resurgence of IHD globally.
3. PATHOGENESIS
3a. Fixed (Chronic) Atherosclerotic Stenosis
- <70% stenosis: Typically asymptomatic at rest and with exertion
- >70% ("critical stenosis"): Reduces coronary flow reserve; causes predictable stable angina on exertion
- >90% stenosis: Can cause ischemia at rest - a form of unstable angina
- Plaques typically affect the first few cm of the LAD and LCX from their takeoff, and along the entire RCA
- Secondary branches (diagonal branches of LAD, obtuse marginals of LCX, posterior descending of RCA) may also be involved
- Gradual occlusion over years allows collateral circulation to develop, potentially protecting from infarction even with complete vessel closure
- Rapid acute occlusion gives no time for collaterals - infarction results
3b. Acute Plaque Change - Trigger of ACS
The initiating event in most ACS is:
- Plaque rupture, fissure, erosion, or ulceration exposing thrombogenic plaque core or subendothelial basement membrane
- Rapid platelet aggregation and thrombus formation at the site of disruption
- Hemorrhage into the plaque core acutely expands its volume, worsening stenosis
- Vasospasm further reduces luminal caliber; also mechanically promotes plaque disruption
Triggers of vasospasm:
- Circulating adrenergic agonists (stress, cocaine use)
- Platelet-derived mediators (thromboxane A2, serotonin)
- Imbalance between NO (vasodilator) and endothelin (vasoconstrictor) due to endothelial dysfunction
- Perivascular inflammatory cell mediators
Most critically, a completely obstructive thrombus over a disrupted plaque causes transmural infarction (STEMI), while partial obstruction typically causes subendocardial infarction (NSTEMI).
4. CLINICAL SYNDROMES OF IHD
4a. Stable (Chronic) Angina
- Due to fixed >70% stenosis; consistently triggered by exertion, cold, or emotion
- Pain: substernal tightness/pressure, radiates to left arm/jaw; relieved by rest or nitroglycerin within 5 min
- ECG during attack: transient ST depression; returns to normal between attacks
- Troponin: normal (no myocyte death)
4b. Unstable Angina (UA)
- Defined by any of: (1) chest pain at rest lasting >10 min, (2) new-onset severe angina, or (3) crescendo pattern - increasing frequency, severity, or duration
- Caused by plaque rupture/erosion + non-occlusive thrombus + vasospasm
- Troponin: normal (distinguishes UA from NSTEMI)
- ECG: transient ST depression or T-wave changes; or normal
4c. NSTEMI (Non-ST Elevation MI)
- Same mechanism as UA but thrombus is sufficiently obstructive to cause subendocardial infarction
- Troponin: elevated (dynamic rise and fall characteristic)
- ECG: ST depression, deep T-wave inversion (≥0.3 mV); no ST elevation; no Q waves
- hsTroponin elevation >99th percentile + clinical history = NSTEMI diagnosis
4d. STEMI (ST Elevation MI)
- Complete, persistent occlusion of a coronary artery
- Causes transmural (full-thickness) infarction
- ECG: ST elevation in affected territory → Q waves develop over 12-24 hours
- Troponin: markedly elevated
- Medical emergency - time from symptom onset to reperfusion is the key determinant of outcome
4e. Vasospastic (Prinzmetal) Angina
- Caused by focal spasm of an epicardial coronary artery - may occur on a background of mild atherosclerosis or in a normal artery
- Pain occurs at rest, typically early morning; not exertional
- ECG during attack: ST elevation (distinguishes from stable angina); resolves with nitroglycerin
- Diagnosis confirmed by: coronary angiography showing transient spasm; provoked by intracoronary acetylcholine or hyperventilation
- Associated with: migraine, Raynaud's phenomenon, cigarette smoking
- Treatment: Calcium channel blockers (first-line); long-acting nitrates; aspirin may worsen spasm (prostacyclin-related mechanism)
- Prognosis: 5-year survival ~90-95%, but ~20% develop MI
4f. Sudden Cardiac Death (SCD)
- Most commonly occurs due to ventricular fibrillation from ischemia-induced myocardial electrical irritability
- Accounts for 80-90% of pre-hospital MI-related deaths (within 1 hour of onset)
- Underlying substrate: usually severe coronary artery disease; may occur without preceding infarction
- In younger patients: inherited channelopathies (long QT, Brugada) or structural anomalies
4g. Chronic IHD / Ischemic Cardiomyopathy
- Progressive cardiac decompensation from accumulated ischemic injury
- From previous infarction(s) or chronic "stunned/hibernating" myocardium
- Manifests as progressive CHF with reduced ejection fraction
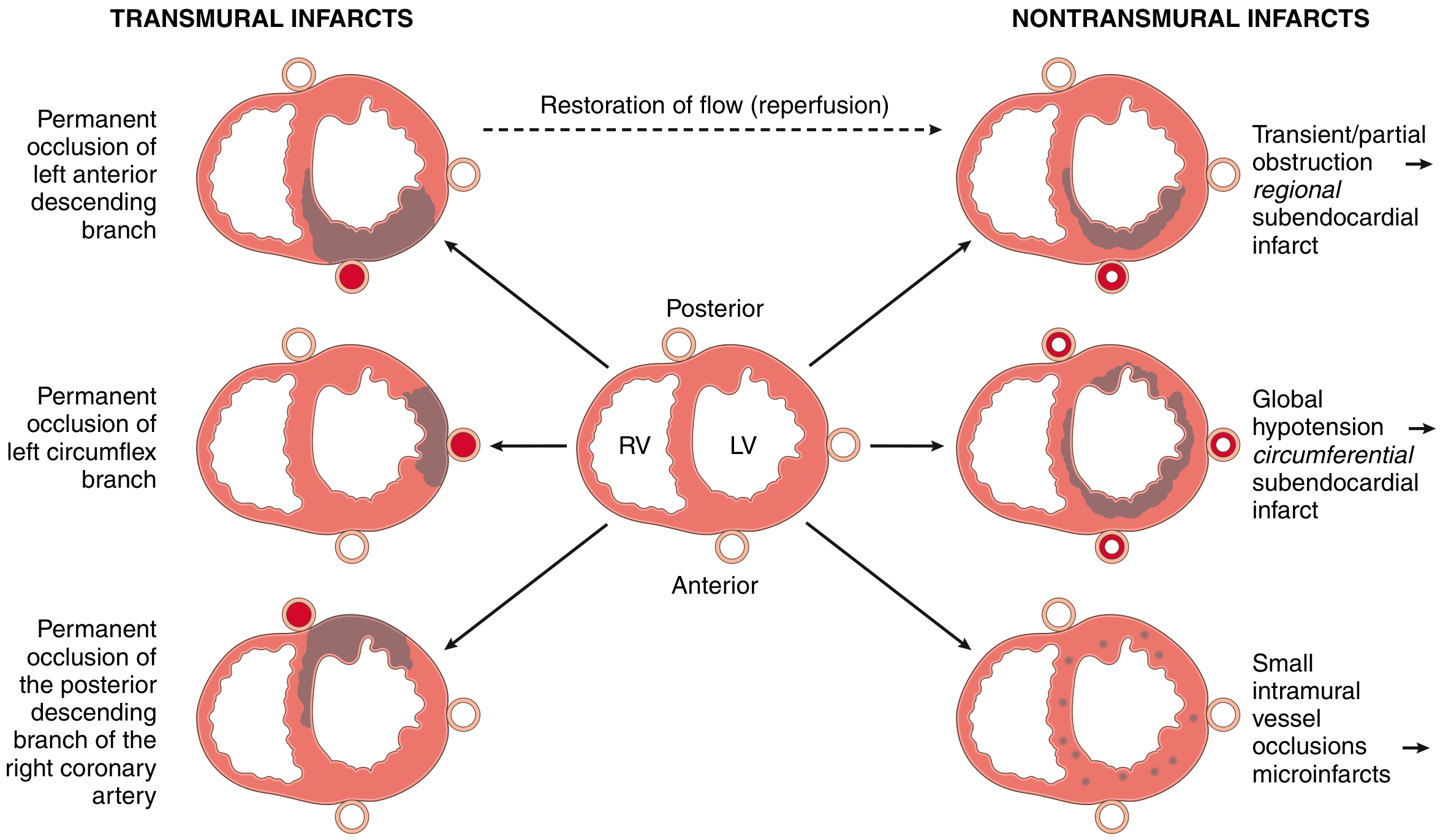
5. TOPOGRAPHIC DISTRIBUTION OF MI BY VESSEL INVOLVED
| Artery Occluded | Territory Infarcted | Frequency |
|---|---|---|
| Proximal LAD | Anterior LV wall, anterior 2/3 of septum, cardiac apex | 40-50% of MIs |
| LCX | Lateral LV wall | 15-20% |
| Proximal RCA | Right ventricle, inferior LV, posterior 1/3 septum (in right-dominant) | 30-40% |
| Posterior descending (PDA) | Posterior LV, posterior septum | depends on dominance |
Right dominance (90% of individuals): PDA arises from RCA. So RCA occlusion = posterior LV + posterior septum involvement.
6. PATHOLOGY OF MYOCARDIAL INFARCTION
6a. Zones of Necrosis
- Transmural infarct: Full-thickness necrosis; caused by complete epicardial artery occlusion; associated with STEMI
- Subendocardial infarct: Limited to inner 1/3 of myocardium; from partial/transient obstruction or global hypotension superimposed on multivessel disease; NSTEMI
- Microinfarcts: From small intramyocardial vessel disease or emboli
The subendocardial region is most vulnerable because it:
- Is the last zone to receive blood delivered via epicardial vessels
- Is subjected to high intramural pressures that impede inflow
6b. Sequential Histological Changes - (HIGH-YIELD)
| Time | Gross Appearance | Light Microscopy | Key Feature |
|---|---|---|---|
| 0-4 h | Normal | Normal (wavy fibers early) | No visible change |
| 4-12 h | Dark mottling begins | Early coagulative necrosis; edema; hemorrhage | Eosinophilic cytoplasm, nuclear pyknosis |
| 12-24 h | Dark mottling | Ongoing coagulative necrosis; contraction bands | Pyknosis, loss of nuclei |
| 1-3 days | Yellow-tan pallor + hyperemic border | Neutrophil infiltration (peak at day 2-3) | Active acute inflammation |
| 3-7 days | Maximal softening, yellow center | Macrophage infiltration; enzymatic lysis of necrotic myocytes | "Gelatinous" soft zone - RUPTURE RISK IS HIGHEST here |
| 1-3 weeks | Pale red-grey borders | Granulation tissue ingrowth; fibroblasts; new vessels | Angiogenesis, early scar |
| >2 months | White fibrous scar | Dense collagen scar | Complete healing |
Coagulative necrosis is the type of necrosis seen in MI - cell outlines preserved but nuclei disappear.
6c. Reperfused Infarction
- Gross: Hemorrhagic (blood leaks into tissue from vascular damage)
- Microscopy: Contraction band necrosis - intense eosinophilic cross-striations of hypercontracted sarcomeres; caused by calcium influx into irreversibly injured cells at the moment of reperfusion; sarcomeres fixed in tetanic state
7. INVESTIGATIONS
7a. Electrocardiography
| Finding | Significance |
|---|---|
| ST elevation ≥1mm in ≥2 contiguous leads | STEMI - full thickness ischemia |
| ST depression, deep T inversion | NSTEMI / UA - subendocardial ischemia |
| New LBBB | Equivalent to STEMI; urgent reperfusion needed |
| Q waves (>0.04 s, >25% of R) | Old/evolving transmural infarct (develop over 12-24 h in STEMI) |
Territory localization on ECG:
- V1-V4: Anterior (LAD)
- I, aVL, V5-V6: Lateral (LCX)
- II, III, aVF: Inferior (RCA)
- V7-V9 (posterior leads): Posterior (RCA/LCX)
- V1, V4R: Right ventricular (RCA)
7b. Cardiac Biomarkers - Detailed
| Marker | Rises | Peaks | Returns to Normal | Key Points |
|---|---|---|---|---|
| hsTroponin I / T | 2-4 h (hs: 1-2 h) | 24-48 h | 7-10 days | Gold standard - highest sensitivity & specificity; used in 0/1 h rule-out algorithm |
| CK-MB | 3-6 h | 24 h | ~72 h | Useful for reinfarction (re-elevation after initial fall); less specific than troponin |
| Myoglobin | 1-3 h | 4-6 h | 24 h | First to rise; NOT cardiac-specific (also in skeletal muscle); useful for early rule-out only |
| LDH (LDH1>LDH2) | 24-48 h | 3-6 days | 8-14 days | Useful if presentation is delayed (>48 h after MI) |
| AST/SGOT | 8-12 h | 18-36 h | 3-4 days | Largely replaced by troponin |
"Troponin" on ECG strips: With reperfusion, both troponin and CK-MB peak earlier due to rapid washout from necrotic tissue - this is a hallmark of successful reperfusion.
Causes of elevated troponin OTHER than MI (important for differential): pulmonary embolism, myocarditis, sepsis, renal failure, stroke, cardiac contusion, Takotsubo cardiomyopathy
7c. Other Investigations
- Echocardiography: Regional wall motion abnormalities (hypokinesia, akinesia, dyskinesia); assess LV function (EF); detect pericardial effusion, VSD, MR
- Coronary angiography: Gold standard to define anatomy; guides PCI or CABG decision
- Stress testing (for stable angina): TMT (treadmill test) - ST depression ≥1mm at submaximal HR indicates significant ischemia; pharmacological stress echo for those who cannot exercise
- Cardiac CT Angiography: Non-invasive; high negative predictive value for ruling out CAD
- Chest X-ray: Pulmonary edema (perihilar haziness, Kerley B lines), cardiomegaly
- CBC, RFT, LFT, lipid profile, blood glucose, HbA1c: Baseline and risk factor assessment
7d. Risk Stratification (for NSTE-ACS)
TIMI Score (0-7 points) and GRACE Score are validated tools:
TIMI Risk Score - high-risk features:
- Age ≥65
- ≥3 CAD risk factors
- Known CAD (stenosis ≥50%)
- Aspirin use in past 7 days (indicates aspirin-resistant platelet activation)
- ≥2 anginal events in 24 h
- Elevated serum cardiac markers
- ST changes ≥0.5 mm
8. COMPLICATIONS OF MYOCARDIAL INFARCTION
Early Complications (hours to days):
1. Arrhythmias (most common complication; occurs in >90% of patients)
- VF - most common cause of early death; occurs within first hour
- VT - often pre-VF
- AF/Atrial flutter - from atrial distension/ischemia
- Heart block/Brady - especially with inferior MI (RCA supplies SA and AV nodes)
- Accelerated idioventricular rhythm (AIVR) - benign reperfusion arrhythmia
2. Cardiogenic Shock
- Occurs when >40% of LV myocardium infarcted
- Features: hypotension, oliguria, pulmonary edema, cold clammy extremities
- Mortality: 50-70% despite treatment
- Management: intra-aortic balloon pump, emergent PCI, vasopressors (dopamine/noradrenaline)
3. Acute Mitral Regurgitation (Papillary Muscle Rupture)
- Day 3-7 post-MI; posteromedial papillary muscle more commonly involved (single RCA supply vs anterolateral which has dual supply)
- Sudden onset of flash pulmonary edema + new loud pansystolic murmur
- Emergent surgical repair required
4. Ventricular Septal Defect (Septal Rupture)
- Day 3-7 post-MI; most common rupture site
- New loud pansystolic murmur + step-up in O2 saturation from RA to RV on catheterization
- Surgical repair + IABP
5. Left Ventricular Free Wall Rupture
- Day 3-7; least common but most lethal rupture
- Causes hemopericardium and acute cardiac tamponade
- Presents with sudden cardiovascular collapse (electromechanical dissociation/PEA)
- Urgent pericardiocentesis + surgery
These three rupture complications are most likely 3-7 days after MI when enzymatic lysis of necrotic myocardium is maximal and the infarct zone has converted to soft friable granulation tissue.
6. Mural Thrombus
- Forms over akinetic endocardium (especially anterior MI with apical involvement)
- Risk of systemic embolization (stroke, renal/mesenteric infarction)
- Anticoagulate with LMWH/warfarin for 3-6 months
7. Right Ventricular Infarction
- Associated with inferior STEMI (RCA occlusion)
- Triad: hypotension + raised JVP + clear lungs (without pulmonary edema)
- ECG: ST elevation in V4R (right-sided lead)
- Management: IV fluids (preload-dependent); avoid nitrates and diuretics
Late Complications (weeks to months):
8. Dressler Syndrome (Post-Pericardiotomy / Post-MI Syndrome)
- Occurs 2-10 weeks after MI
- Autoimmune pericarditis (antibodies against damaged myocardial antigens)
- Features: pleuritic chest pain, fever, pericardial friction rub, pericardial/pleural effusion
- Treatment: NSAIDs, colchicine; steroids for refractory cases
9. Ventricular Aneurysm
- Thinned, scarred, non-contractile LV wall that bulges paradoxically
- ECG: Persistent ST elevation (>2 weeks after MI without evolution)
- Echo: dyskinetic wall segment
- Complications: mural thrombus, arrhythmias, CHF
- Large symptomatic aneurysms: surgical aneurysmectomy
10. Chronic Heart Failure / Ischemic Cardiomyopathy
- Progressive ventricular dilation and remodeling
- Reduced EF, dyspnea, exercise intolerance, recurrent hospitalizations
11. Pericarditis (Early)
- Day 1-3 after transmural MI (fibrinous pericarditis over necrotic epicardium)
- Pleuritic chest pain, friction rub, diffuse ST elevation
- Treatment: aspirin (NSAIDs cautious due to impaired healing)
9. MANAGEMENT
9a. Initial Management of ACS (Universal)
MONA + antiplatelet + anticoagulant (first 30 minutes):
- Morphine: 2-4 mg IV for pain, anxiety, preload reduction (caution - may mask symptoms)
- Oxygen: Only if SpO2 <90% or in respiratory distress; not routine
- Nitrates: Sublingual GTN 0.3-0.6 mg; if not relieved x3 doses → IV nitroglycerin at 5-10 µg/min, titrating up
- Contraindications: Hypotension, RV infarction, recent PDE-5 inhibitor use (sildenafil/vardenafil within 24 h; tadalafil within 48 h), severe aortic stenosis
- Aspirin: 300 mg loading dose (chew); then 75-100 mg daily indefinitely
9b. Antiplatelet Therapy
- Dual Antiplatelet Therapy (DAPT): Aspirin + P2Y12 inhibitor
- P2Y12 options:
- Ticagrelor 180 mg loading, 90 mg BD (preferred - faster onset, not a prodrug)
- Clopidogrel 300-600 mg loading, 75 mg daily (consider if ticagrelor not available; ~30% are poor metabolizers due to CYP2C19 polymorphism)
- Prasugrel 60 mg loading, 10 mg daily (avoid in prior stroke/TIA, age >75, weight <60 kg)
- Duration of DAPT: 12 months for ACS; may extend to >12 months in high thrombotic risk; shorten to 3-6 months if high bleeding risk
9c. Anticoagulation
Four options (parenteral):
- UFH (Unfractionated heparin): Bolus + infusion; easily reversible with protamine
- LMWH (Enoxaparin): SC once/twice daily; preferred for NSTE-ACS; no reversal agent until fondaparinux
- Fondaparinux (factor Xa inhibitor): Once daily SC; less bleeding than enoxaparin; avoid in severe renal failure
- Bivalirudin (direct thrombin inhibitor): IV; used during PCI; less major bleeding
9d. Reperfusion Strategy
For STEMI (time-critical):
| Strategy | Indication | Time Target |
|---|---|---|
| Primary PCI | Preferred if available | Door-to-balloon time <90 min from first medical contact |
| Fibrinolysis (thrombolysis) | If PCI not available within 120 min of diagnosis | Administer within 10 min of STEMI diagnosis |
Fibrinolytic agents:
- Alteplase (tPA): Fibrin-specific; accelerated regimen: 15 mg IV bolus then 0.75 mg/kg over 30 min then 0.5 mg/kg over 60 min
- Streptokinase: Non-fibrin-specific; 1.5 million units IV over 60 min; cheaper; cannot be given twice (antibodies formed)
- Tenecteplase (TNK-tPA): Single weight-based IV bolus; most convenient
Absolute contraindications to fibrinolysis:
- Prior intracranial hemorrhage or hemorrhagic stroke at any time
- Ischemic stroke within 3 months
- Active bleeding (excluding menses)
- Suspected aortic dissection
- Significant head trauma or intracranial neoplasm within 3 months
- Severe uncontrolled hypertension (>180/110 despite treatment)
For NSTEMI/UA:
- Invasive strategy (angiography within 24-72 h) for high-risk patients
- Conservative strategy for low-risk patients initially managed medically
9e. Anti-Ischemic Medical Therapy
Beta-blockers:
- Reduce heart rate and contractility → decreased myocardial O2 demand
- Reduce infarct size, arrhythmias, risk of reinfarction
- Start early (within 24 h) in absence of contraindications
- Contraindications: PR >0.24 s, 2nd/3rd degree AV block, HR <50/min, SBP <90 mmHg, Killip class III/IV heart failure, severe reactive airways disease
Nitrates:
- Venodilation → reduce preload → reduce O2 demand
- Coronary vasodilation
- Sublingual for acute attacks; IV for ongoing ischemia
Calcium Channel Blockers:
- Used when beta-blockers contraindicated
- Non-dihydropyridine (diltiazem, verapamil): slow HR, used for angina; avoid in LV dysfunction or HF
- Dihydropyridine (amlodipine): vasodilation; use with beta-blocker for stable angina; avoid short-acting nifedipine alone
9f. Secondary Prevention (Long-term)
| Drug | Indication | Mechanism / Benefit |
|---|---|---|
| Aspirin | All IHD patients indefinitely | Antiplatelet; reduces reinfarction by ~25% |
| Statin (high-intensity) | All ACS patients | Plaque stabilization, LDL reduction; start regardless of baseline LDL |
| ACE inhibitor / ARB | Post-MI, especially with EF <40%, diabetes, hypertension | Prevents adverse LV remodeling; reduces mortality |
| Beta-blocker | Post-MI; EF <40% | Reduces sudden cardiac death, reinfarction |
| Aldosterone antagonist (eplerenone) | Post-MI with EF <40% + DM or HF | Reduces mortality in high-risk groups |
| SGLT2 inhibitor | Post-ACS with HFrEF or T2DM | Reduces HF hospitalization and CV death |
9g. Surgical - CABG (Coronary Artery Bypass Grafting)
Indications:
- Left main coronary artery disease (≥50% stenosis)
- Three-vessel disease with impaired LV function (EF <35-50%)
- Two-vessel disease involving proximal LAD with impaired EF
- Failed PCI
- Anatomy unsuitable for PCI
Conduits used:
- Left internal mammary artery (LIMA) to LAD - best patency (>90% at 10 years)
- Saphenous vein grafts - lower patency (~50% at 10 years)
10. KILLIP CLASSIFICATION (Clinical severity post-MI)
| Class | Description | Hospital Mortality |
|---|---|---|
| I | No HF (no S3, no rales) | ~6% |
| II | Mild HF (S3, rales <50% lung fields, JVD) | ~17% |
| III | Pulmonary edema (rales >50% lung fields) | ~38% |
| IV | Cardiogenic shock (SBP <90 + signs of hypoperfusion) | ~67-81% |
11. SPECIAL CONCEPTS
Myocardial Stunning
- Transient, reversible post-ischemic dysfunction persisting for hours to days after reperfusion
- Myocyte is alive but non-contractile due to persistent biochemical abnormalities
- Function recovers spontaneously with time
Myocardial Hibernation
- Chronic, persistent reduction in regional myocardial contractility due to chronic ischemia
- A protective "down-regulation" of metabolism to match reduced blood supply
- Reversible with revascularization - important concept for deciding CABG vs medical therapy
- Diagnosed by: viability studies (dobutamine stress echo, PET scan)
Ischemic Preconditioning
- Brief episodes of ischemia followed by reperfusion make the myocardium more resistant to a subsequent prolonged ischemic insult
- Mediated by adenosine, bradykinin, PKC, KATP channels
- Basis of "ischemic preconditioning" phenomenon and research into cardioprotective strategies
12. PROGNOSIS AND MORTALITY
-
Overall in-hospital mortality for MI: 7-8%
-
STEMI mortality: ~10% in-hospital; one-third die out-of-hospital (mostly from VF within 1 hour)
-
NSTEMI mortality: ~6% in-hospital; but cumulative 1-year mortality approaches STEMI
-
Factors worsening prognosis:
- Large infarct size
- Reduced EF (<40%)
- Cardiogenic shock
- Advanced age, female sex (worse outcomes due to treatment delays)
- Diabetes mellitus
- Multivessel disease
- VT/VF on presentation
- Late presentation (>12 h without reperfusion)
-
Mortality has fallen by 50% since 1963 - attributed to:
- Smoking cessation, statin use, BP control
- Aspirin, beta-blockers, ACE inhibitors
- CCU-based monitoring for arrhythmia
- Thrombolysis and primary PCI
- Mechanical circulatory support devices
Summary: Key Differences Table
| Feature | Stable Angina | Unstable Angina | NSTEMI | STEMI | Prinzmetal Angina |
|---|---|---|---|---|---|
| Trigger | Exertion/emotion | Spontaneous/minimal | Spontaneous | Spontaneous | Rest/early morning |
| Mechanism | Fixed stenosis >70% | Plaque rupture + non-occlusive thrombus | Partial occlusion | Complete occlusion | Coronary vasospasm |
| ECG during pain | ST depression | ST depression/normal | ST depression | ST elevation | ST elevation |
| Troponin | Normal | Normal | Elevated | Markedly elevated | Normal |
| Infarct type | None | None | Subendocardial | Transmural | None (usually) |
| Immediate Rx | Nitrates + rest | Admit + heparin + DAPT | PCI within 24-72 h | Primary PCI within 90 min | Ca++ channel blockers |
Sources: Robbins & Kumar Basic Pathology, 10th Ed. | Harrison's Principles of Internal Medicine, 22nd Ed. (2025) | Braunwald's Heart Disease, 12th Ed. | Goldman-Cecil Medicine, International Ed.
This is a shared conversation. Sign in to Orris to start your own chat.