I now have comprehensive, authoritative content from textbooks, clinical guidelines, and research. Let me compile the full protocol.
Lower Limb Exercise Protocol
Pelvic/Limb-Girdle MD (LGMD) | Facioscapulohumeral MD (FSHD) | Becker MD (BMD)
Understanding the Weakness Patterns
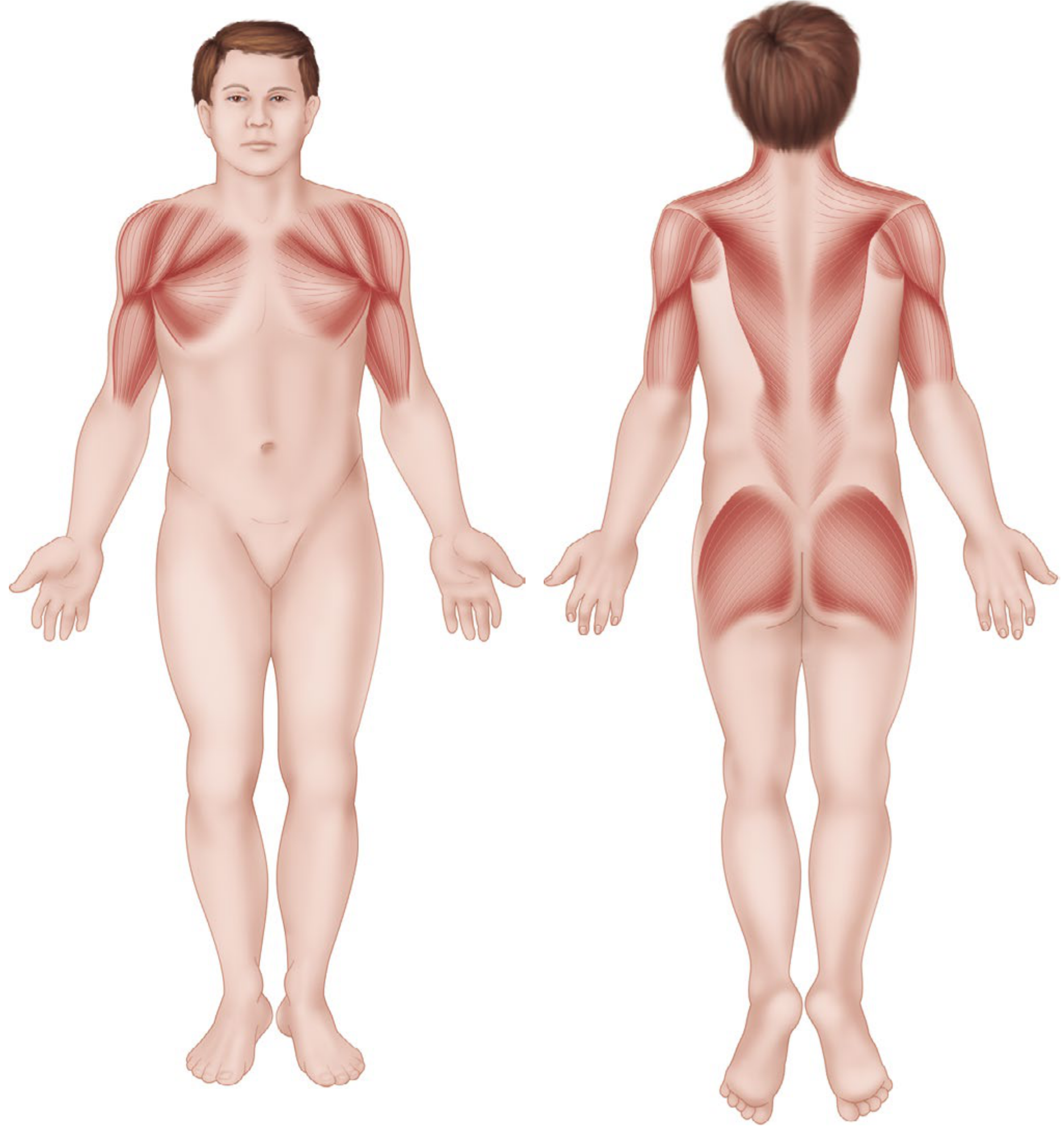
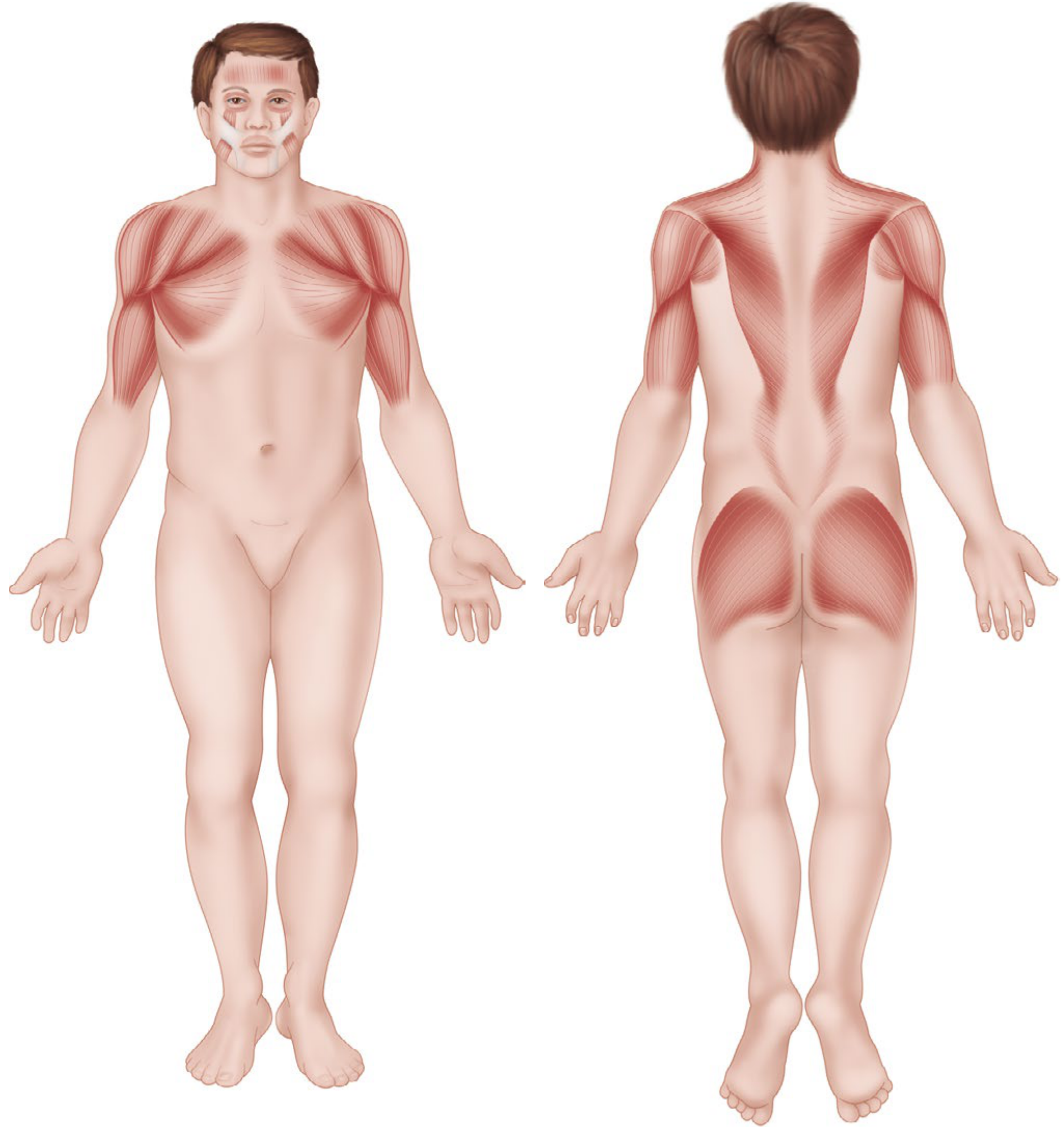
The exercise protocol must be tailored to where each condition causes muscle weakness. The images below from Campbell's Operative Orthopaedics (15th Ed, 2026) show the affected muscle groups:
Limb-Girdle MD - pelvic girdle (hip muscles, gluteals) and shoulder girdle predominantly:
Facioscapulohumeral MD - face, shoulder girdle, and descending to hip girdle, tibialis anterior:
(Campbell's Operative Orthopaedics 15th Ed 2026, Figures 37.16 and 37.17)
Universal Principles for All Three Conditions
These rules apply regardless of diagnosis and must not be violated:
| Principle | Rationale |
|---|
| Submaximal effort only (keep below 30-40% of 1RM for resistance) | Prevents "overwork weakness" - permanent muscle loss from overloading already dystrophic fibers |
| Avoid or minimize eccentric contractions | Eccentric loading causes greatest mechanical and metabolic damage to dystrophic muscle; particularly dangerous in LGMD R2 (dysferlinopathy) |
| Never allow prolonged bed rest | Inactivity accelerates functional decline far faster than the disease itself |
| Monitor for overexertion signs | Dark urine (myoglobinuria), muscle cramps >24 hrs, feeling weaker than baseline = reduce load immediately |
| Prevent obesity | Excess body mass significantly overloads weakened lower limb muscles |
| Preventive > restorative | Contracture prevention, ambulation maintenance, and posture must be started early |
| Cardiac clearance before aerobic training | All three conditions can involve cardiomyopathy, especially BMD |
Adams and Victor's Principles of Neurology, 12th Ed.; PM&R KnowledgeNow - LGMD; FSHD Society PT Guidelines 2025
SECTION 1: Pelvic / Limb-Girdle Muscular Dystrophy (LGMD)
Clinical Profile for Exercise Planning
- Weakness is symmetric and proximal - primarily hip flexors, extensors, abductors, and knee extensors
- Falls and difficulty rising from chairs/floor are the primary functional deficits
- Sarcoglycanopathies (LGMD R3-R6) resemble Duchenne in severity; dysferlinopathy (LGMD R2) - eccentric exercise must be strictly avoided
- Stationary cycling 3x/week for 30 min has been shown to improve functional capacity (sit-to-stand, rise from floor) without elevating CK or worsening muscle morphology (Sveen et al.; Vissing et al., 10-week home ergometer program)
LGMD Stretching Protocol
Frequency: Daily or minimum 4x/week
Each stretch: Hold 10-30 seconds, repeat 2-4 times per muscle group
Best timing: After warmup, after cardio, or after warm bath/hot pack
| Muscle Group | Stretch Technique | Notes |
|---|
| Hip flexors (iliopsoas) | Kneeling lunge or standing lunge with pelvic tilt | Critical - hip flexor tightness worsens lordosis and gait |
| Hamstrings | Supine with towel loop, or long-sit stretch | Active-assistive if hip flexor too weak |
| Hip adductors | Supine butterfly or seated butterfly | Gentle - no forced passive range |
| Gluteals / piriformis | Supine figure-4 (ankle on opposite knee) | Also stretches external hip rotators |
| Quadriceps | Prone or sidelying heel-to-buttock | Use support rail if balance impaired |
| Gastrocnemius / soleus | Standing heel stretch against wall (straight knee, then bent knee) | Important for ankle contracture prevention |
| Tibialis anterior / dorsiflexors | Seated gentle plantar flexion range | Only if hypertonicity develops |
LGMD Strengthening Protocol
Phase 1 - Foundation (Weeks 1-4)
Frequency: 2x/week supervised
Sets x Reps: 2 x 10 per exercise
Rest: 60 seconds between sets
| Exercise | Target Muscles | Technique Notes |
|---|
| Sit-to-stand (from chair) | Quadriceps, gluteals, hip extensors | Use arm support initially; concentric focus only - do NOT train slow lowering phase |
| Side-lying hip abduction | Gluteus medius | Gravity-neutral position reduces load; no ankle weights week 1-4 |
| Supine heel slides (hip flexion) | Hip flexors, iliopsoas | No resistance; gravity-eliminated position |
| Seated knee extension (light band) | Quadriceps | Light resistance band only; avoid end-range locking |
| Standing hip extension at wall | Gluteus maximus | "Donkey kick" with wall support for balance |
| Seated heel raises | Gastrocnemius, soleus | Concentric only; seated reduces body weight demand |
Phase 2 - Progressive Resistance (Weeks 5-12)
Frequency: 2-3x/week
Sets x Reps: Progress to 3 x 10 after week 7
Load adjustment: Increase resistance every 3 weeks if patient can complete 2 extra reps above target
| Exercise | Target Muscles | Progression |
|---|
| Sit-to-stand without arm support | Quadriceps, gluteals | Advance to low seat height to increase demand |
| Partial squats (30-45 degrees ROM) | Quadriceps, gluteals, hip extensors | Bodyweight only initially; wall support available |
| Step-ups (15 cm step) | Quadriceps, hip extensors | Controlled ascent; do NOT train slow descent |
| Side-steps / crab walks with light band | Hip abductors | Light resistance band around ankles or above knees |
| Seated leg press (low load) | Multi-joint lower limb | Preferred over isolated extension - safer loading pattern |
| Prone or standing knee flexion | Hamstrings | Light ankle weight only; progress slowly |
| Standing heel raises with support | Gastrocnemius | Bilateral; progress to unilateral only if well-tolerated |
LGMD Aerobic Protocol
Mode: Stationary cycling (preferred) or aquatic exercise/walking
Frequency: 3x/week
Duration: Start 10-15 min, progress to 30 min
Intensity: <70% maximal aerobic capacity; Borg RPE 11-13 ("light to somewhat hard")
Evidence base: 10-week home ergometer program (3x/week, 30 min) in LGMD R12 improved sit-to-stand performance without CK elevation or worsened muscle morphology (Vissing et al.); similar results in LGMD R9 (Sveen et al.)
SECTION 2: Facioscapulohumeral Muscular Dystrophy (FSHD)
Clinical Profile for Exercise Planning
- Descends craniocaudally: face → shoulder → abdominal/trunk → hip girdle → tibialis anterior (footdrop)
- Increased lumbar lordosis is common (see clinical photo in Campbell's 15th Ed, Fig. 37.18)
- Footdrop from tibialis anterior weakness is a major fall risk - ankle dorsiflexion exercises and AFO assessment are essential
- Approximately 50% of adults remain ambulatory; exercise goals differ significantly between ambulatory and non-ambulatory patients
- HHS guidelines endorsed by FSHD Society: ~150 min/week moderate aerobic exercise; strengthening 2-3 days/week
FSHD Stretching Protocol
Frequency: Daily or minimum 3x/week; stretch after warmup or hot pack
Each stretch: Hold 10-30 seconds, repeat 2-4 times
| Muscle Group | Technique | Priority |
|---|
| Gastrocnemius / soleus | Wall stretch: straight knee then bent knee (Achilles focus) | HIGH - ankle contracture prevention |
| Hip flexors | Standing or kneeling lunge with pelvic tilt | HIGH - compensates for hip girdle weakness |
| Hamstrings | Long-sit or supine towel stretch | HIGH |
| Quadriceps | Prone or sidelying heel-to-buttock | Moderate |
| Hip adductors | Supine butterfly | Moderate |
| Piriformis / lateral hip | Figure-4 supine | Moderate |
| Tibialis anterior | Seated plantar flexion glide | Only if spastic pattern develops |
| Lateral trunk / IT band | Side-lying or standing lateral lean | Common source of pain in FSHD |
FSHD Lower Limb Strengthening Protocol
Frequency: 2-3x/week
Aerobic recommendation: 30 min sessions 5x/week OR 10-min bouts 3x/day
Key rule: High-resistance exercise (>30% 1RM) is contraindicated; eccentric contractions are avoided
| Exercise | Target | Sets x Reps | Notes |
|---|
| Sit-to-stand | Quadriceps, gluteals | 2-3 x 10 | Core FSHD functional goal |
| Marching in place | Hip flexors, tibialis anterior | 2 x 30 sec | Low impact; activates footdrop-prone muscles |
| Toe taps (front, lateral, medial targets) | Tibialis anterior, peroneals | 2 x 10 each direction | Footdrop prevention; do at wall for support |
| Toe raises (dorsiflexion against gravity) | Tibialis anterior | 2 x 15 | Seated; most important exercise for footdrop |
| Heel raises (standing with support) | Gastrocnemius, soleus | 2 x 15 | Bilateral; concentric only |
| Side-walks / crab walks | Hip abductors, gluteus medius | 2 x 10 steps each direction | Light resistance band if tolerated |
| Straight leg raises (supine) | Quadriceps, hip flexors | 2 x 10 | No resistance initially; gravity only |
| Low-intensity partial squats | Quadriceps, gluteals | 2 x 10 | Bodyweight; 30-45 degrees only |
| Step-ups (low step ~15 cm) | Quadriceps, hip extensors | 2 x 10 each leg | Controlled ascent; use hand support |
| Quadruped walking (hands and knees) | Hip extensors, trunk stability | 2 x 15 sec | Activates posterior chain safely |
| Quadruped "superman" (alternate arm/leg) | Gluteals, hamstrings | 2 x 8 each side | Prone posterior chain activation |
| Side-step overs / step-taps | Coordination, balance | 2 x 10 | Visual targets on floor; fall prevention |
| Backward walking | Quadriceps | 2 x 10 m | Only if good balance; wall available |
Modification rule: If a patient cannot complete an exercise through full range of motion due to weakness or body weight, provide: manual assistance from therapist, resistance band assistance, or perform in gravity-neutral/side-lying position.
FSHD Aerobic and Balance Protocol
- Swimming/aquatic exercise: the single best aerobic mode for FSHD - non-weight-bearing, no eccentric loading, whole-body cardiovascular benefit. Kickboard walking, water walking, gentle swimming
- Stationary cycling (light resistance): 15-20 min at Borg RPE 11-13, 3-5x/week
- Balance training: on stable flat surface (avoid unstable surfaces if footdrop present); single-leg stance with wall support; shuffle patterns on floor; stepping over low obstacles
- Yoga/Pilates: gentle, low-load flexibility work is endorsed by FSHD Society; improves lumbar lordosis and hip mobility
- FSHD Society PT Guidelines 2025 (ENMC Standards endorsed)
FSHD Orthotic Consideration
- Ankle-foot orthosis (AFO): should be assessed for all patients with footdrop (tibialis anterior weakness); reduces fall risk and improves gait efficiency
- Night splinting for plantar flexor contracture prevention
SECTION 3: Becker Muscular Dystrophy (BMD)
Clinical Profile for Exercise Planning
- Partial dystrophin function retained; milder and later-onset than Duchenne
- Proximal lower limb weakness (hip flexors, quadriceps, gluteals) is primary
- Exercise intolerance, myalgias, and post-exertional cramps are common even in mild disease - Adams and Victor's, 12th Ed.
- Cardiomyopathy is a major comorbidity and must be evaluated before starting any aerobic program
- Many adults remain ambulatory; isometric contractions are the least damaging and are preferred in early strengthening
BMD Stretching Protocol
Frequency: 4-6x/week; passive stretching 20-30 repetitions per muscle group per session
Hold time: 10-30 seconds; 2-4 repetitions per stretch
| Muscle Group | Technique | Notes |
|---|
| Hip flexors | Kneeling or standing lunge | Tight hip flexors worsen lumbar lordosis and gait |
| Hamstrings | Long-sit or supine towel loop | Active-assistive approach preferred |
| Gastrocnemius / soleus | Wall heel stretch (straight then bent knee) | Night splinting if plantar flexor tightness develops |
| Quadriceps | Prone heel-to-buttock | Support rail for balance |
| Hip adductors | Supine butterfly | Gentle range only |
| Piriformis | Figure-4 supine | Important for hip external rotator tightness |
| Tibialis anterior | Seated plantar flexion range | Mild stretch only |
"Contractures were reduced by passive stretching of the muscles 20 to 30 times a day and by splinting at night." - Adams and Victor's Principles of Neurology, 12th Ed.
BMD Strengthening Protocol
Frequency: 2x/week (supervised sessions recommended)
Core principle: Isometric contractions are the safest; progress to concentric; eccentric loading avoided
| Exercise | Target Muscles | Sets x Reps | Notes |
|---|
| Isometric quadriceps hold (seated, leg extended) | Quadriceps | 3 x 5-10 sec holds | Safest contraction type; no joint movement |
| Isometric gluteal squeeze (supine) | Gluteus maximus | 3 x 5-10 sec | Supine or seated; contract and hold |
| Sit-to-stand | Quadriceps, gluteals, hip extensors | 2 x 10 | Use arm support as needed; increase to 3 x 10 after 3 weeks |
| Step-ups (15-20 cm step) | Quadriceps, hip extensors | 2 x 10 each | Controlled ascent; avoid slow loaded descent |
| Partial squats (bodyweight, 30-45°) | Quadriceps, gluteals | 2 x 10 | Wall or chair support available; no added load |
| Side-lying hip abduction | Gluteus medius | 2 x 12 each | Gravity-neutral; no weight initially |
| Seated knee flexion (light resistance) | Hamstrings | 2 x 10 | Starting in gravity-neutral position |
| Standing calf raises (bilateral, with support) | Gastrocnemius, soleus | 2 x 15 | Concentric only; bilateral |
| Balance exercises (single-leg stance at wall) | Proprioception, stabilizers | 3 x 10-second holds | Near wall; builds stability without muscle overload |
| Seated marching | Hip flexors | 2 x 20 alternating | Gravity-assisted; low load |
Progression rule: Every 3 weeks, if patient can complete 2 extra reps above target with no next-day soreness, increase by one set or small resistance increment.
BMD Aerobic Protocol
Mode priority order: Stationary cycling (no/low resistance) > swimming/aquatic walking > supervised walking
Frequency: 3x/week
Duration: Begin 10-15 min; progress to 30 min over 6-8 weeks
Intensity: Borg RPE 11-13; conversational pace
| Mode | Benefit | Caution |
|---|
| Stationary cycling (zero resistance) | Excellent - minimal eccentric loading; adjustable; cardiovascular benefit | Ensure seat height appropriate; no standing climbs |
| Swimming / kickboard | Best for reducing muscle load; water buoyancy assists weakened limbs | Cardiac clearance mandatory |
| Water walking | Safe cardiovascular training; fall-protected environment | Assess pool depth to patient's comfort |
| Walking (supervised) | Maintains ambulation; ADL-functional | Spotter required; avoid uneven ground; set comfortable distance only |
| Breathing exercises | Pulmonary reserve support; relaxation | Relevant in advancing disease |
| Yoga / gentle stretching | Flexibility and mindfulness | Avoid deep eccentric poses |
iNMD Exercise Guidelines for Becker MD; MDA At-Home PT Exercises 2025
Consolidated Comparison Table
| Feature | LGMD (Pelvic) | FSHD | BMD |
|---|
| Primary lower limb weakness | Hip girdle, proximal thigh | Hip girdle + tibialis anterior | Proximal thigh, hip flexors |
| Footdrop risk | Low | HIGH | Low-moderate |
| Stretching frequency | 4x/week minimum | Daily (minimum 3x/week) | 4-6x/week |
| Strengthening frequency | 2-3x/week | 2-3x/week | 2x/week |
| Best aerobic mode | Stationary cycling / aquatics | Swimming (preferred) | Stationary cycling / aquatics |
| Eccentric exercise | Avoid (especially R2 subtype) | Avoid | Avoid |
| Load limit | <70% max aerobic capacity | <30% 1RM | Isometrics first; then concentric |
| Key functional target | Sit-to-stand, rising from floor | Dorsiflexion, gait, balance | Gait endurance, sit-to-stand |
| Special precaution | CK monitoring; eccentric ban in dysferlinopathy | AFO assessment; footdrop prevention | Cardiac evaluation mandatory pre-program |
| Night splinting | If ankle tightness | Yes (plantar flexors + wrist) | If plantar flexor tightness develops |
Evidence Base
- Bostock et al. (2019, Frontiers in Neurology) - RCT in exactly these three conditions (FSHD n=6, LGMD n=6, BMD n=5): 12-week twice-weekly supervised resistance training produced 13% increase in knee flexor torque and significant improvements in sit-to-stand, stair ascent, and stair descent times (p<0.05). Protocol: 2 sets x 10RM → 3 sets x 10RM at week 3; exercises included seated knee extension/flexion, hip extension, hip abduction, squat, and step-up; 2 sec concentric : 4 sec eccentric tempo; 1 min rest between sets.
- Vissing et al. / Sveen et al. - Stationary cycling ergometer (3x/week, 30 min) in LGMD improved functional capacity and aerobic fitness without CK elevation or muscle damage on biopsy.
- FSHD Society / ENMC Standards (2025 edition) - aerobic 150 min/week moderate intensity; strengthening 2-3x/week; stretching daily; high-resistance and eccentric exercise avoided.
- Adams and Victor's Principles of Neurology, 12th Ed. - "Maximal resistance exercises, if begun early, can strengthen muscles in Duchenne, limb-girdle, and facioscapulohumeral dystrophies... none of the muscles was weaker at the end of a year than at the beginning."
- PMC scoping review 2025 (PMID: PMC11708444) - confirms aerobic exercise at moderate intensity (<70% maximal aerobic capacity) is the most feasible and safe option across LGMD subtypes; eccentric and high-resistance training should be avoided.
Clinical reminder: All exercise programs for these conditions should begin with a baseline assessment of strength (manual muscle testing or dynamometry), functional tasks (timed sit-to-stand, 6-minute walk test), and a daily symptom log. Programs must be individually tailored and monitored by a trained physiotherapist familiar with neuromuscular disease. Persistent post-exercise soreness beyond 24 hours signals overtraining and requires load reduction.