Chronic osteomyelitis treatment
Reading File
Finding Sources
Searching PubMed
"chronic osteomyelitis"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Searching PubMed
"osteomyelitis"[MeSH Terms] AND "anti-bacterial agents"[MeSH Terms]
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive data from multiple authoritative textbooks. Let me compile the full answer.
Chronic Osteomyelitis: Treatment
Overview
Chronic osteomyelitis is defined not simply by duration, but by the presence of bone necrosis (sequestra). Acute osteomyelitis without necrosis can be treated with antibiotics alone; once necrosis develops, antibiotic treatment must be combined with surgical debridement. The most important goal is preventing progression to chronicity through rapid diagnosis and prompt early treatment. — Harrison's Principles of Internal Medicine 22E (2025)
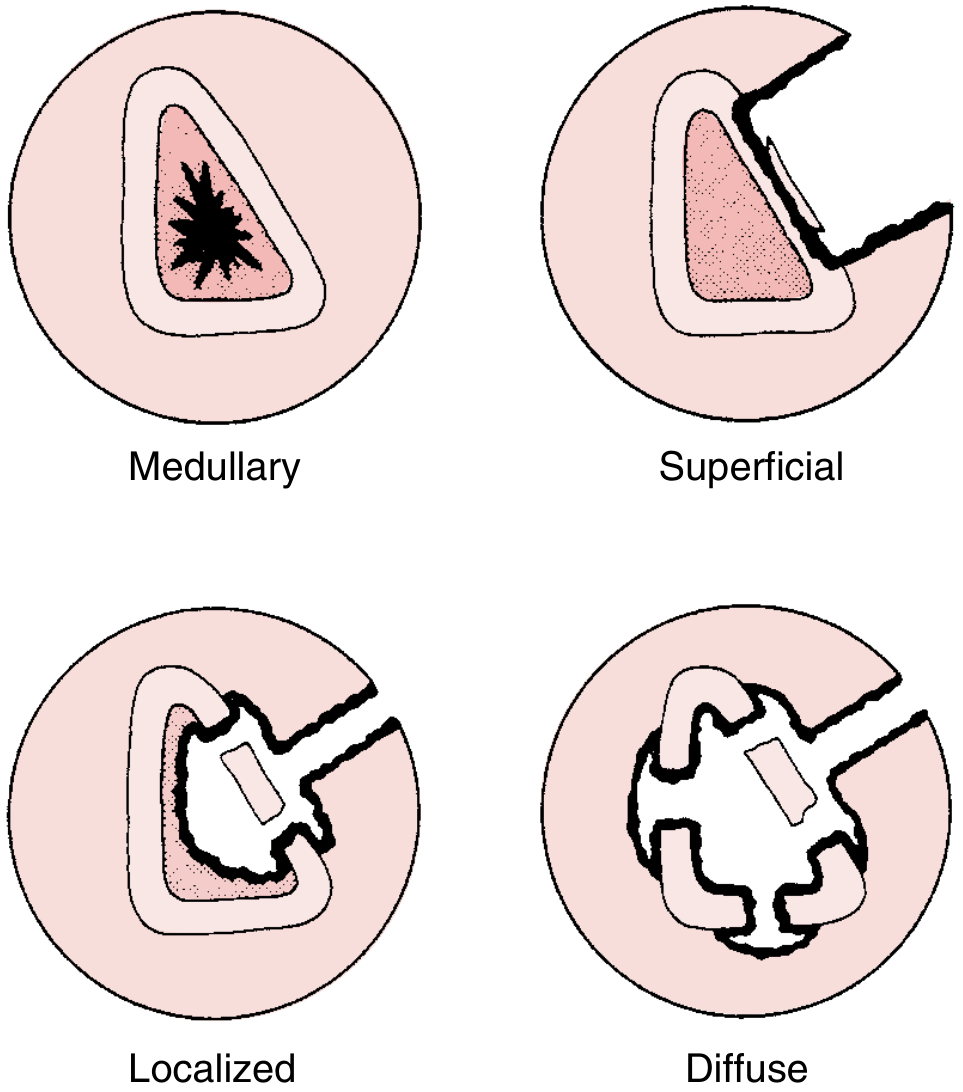
Classification: Cierny-Mader Staging System
Used to guide surgical management:
Anatomic (lesion type):
| Stage | Type | Description | Treatment |
|---|---|---|---|
| I | Medullary | Endosteal nidus (residual hematogenous) | Unroofing |
| II | Superficial | Surface cortical defect | Saucerization |
| III | Localized | Full-thickness cortical lesion (stable) | Debridement + stabilization |
| IV | Diffuse | Through-and-through involvement (unstable) | Extensive debridement ± reconstruction |
Host classification:
| Type | Description | Risk |
|---|---|---|
| A | Normal immune response; nonsmoker | Minimal |
| B | Local (vascular compromise, scarring, radiation) or systemic (DM, malnutrition, ESRD, HIV) | Moderate |
| C | Major nutritional/systemic disorder — morbidity of treatment exceeds disease | High (palliative/amputation) |
Principles of Treatment
The three pillars of chronic osteomyelitis treatment are:
- Radical surgical debridement (most important)
- Dead space management
- Targeted systemic (and local) antibiotic therapy
"The most important clinical predictor of a successful outcome is the adequacy of debridement, as the presence of dead bone, biofilm formation, and a compromised tissue envelope render systemic antibiotic agents ineffective." — Rockwood & Green's Fractures in Adults, 10th Ed. (2025)
1. Surgical Debridement
Goal: Remove all devitalized/dead bone and necrotic soft tissue until punctate cortical bleeding is restored — the "paprika sign" (pin-point bleeding from viable bone). — Miller's Review of Orthopaedics 9th Ed.
Key steps:
- Removal of all infected hardware (if present and unstable)
- Sequestrectomy — excision of avascular dead bone
- Debridement of compromised/necrotic soft tissue
- Consider preoperative sinus tract injection with methylene blue to delineate tracts
- Consider reaming of the intramedullary canal (RIA — Reamer-Irrigator-Aspirator) for medullary involvement
Surgical techniques (Rockwood & Green):
| Technique | Indication |
|---|---|
| Radical debridement | All suitable patients; medullary involvement |
| Intramedullary RIA reaming | Medullary canal disease; lower morbidity than conventional |
| Amputation | Marjolin ulcer, multiple failed treatments, patient preference |
Important notes:
- Multiple/repeat procedures are frequently required
- In patients with severe comorbidities unfit for extensive surgery: long-term suppressive antibiotics ± limited debridement
- Preoperative nutritional optimization is essential
2. Dead Space Management
After radical debridement, large osseous defects ("dead space") must be managed to prevent bacterial proliferation, abscess, and recurrence.
Options:
- Antibiotic-impregnated cement spacers or beads (PMMA) — temporary; eradicate infection before second-stage reconstruction. Vancomycin and tobramycin are commonly loaded. This is the preferred first-stage approach.
- Local flaps (muscle, pedicle myocutaneous, osseous) — promote healing and vascularization
- Vascularized free flaps — most reliable for large defects; minimize recurrence risk
- Primary bone grafting — generally not recommended in acute phase (high resorption rate due to ongoing inflammation)
- Masquelet/induced membrane technique — cement spacer in Stage 1, then bone grafting through the formed membrane in Stage 2
"Antibiotic-impregnated cement spacers or beads are often indicated until infection is eradicated and reconstruction is carried out as a second-stage procedure." — Rockwood & Green's Fractures in Adults, 10th Ed. (2025)
3. Antibiotic Therapy
General Principles
- Antibiotics alone are insufficient for chronic osteomyelitis — surgery is mandatory
- Antibiotic choice should be based on deep intraoperative bone cultures (not sinus tract swabs, which reflect skin contaminants)
- Cultures should ideally be obtained before antibiotic therapy or after a washout period
- Antibiotic stewardship programs improve outcomes
Duration
- Typically 6 weeks of targeted therapy following adequate debridement — Harrison's 22E (2025)
- Emerging evidence: 3 weeks may be as good as 6 weeks after extensive debridement in immunocompetent patients — Goldman-Cecil Medicine
- After amputation: only a short course is required
- Long-term oral suppressive therapy if surgery would cause more harm than the disease
Route
- IV→oral step-down is effective; oral antibiotics achieve adequate bone levels
- Oral ciprofloxacin 750 mg twice daily × 6–12 weeks is acceptable as an alternative to parenteral therapy for chronic osteomyelitis — Goldman-Cecil Medicine
- IV and oral routes achieve similar cure rates when appropriate bioavailable agents are chosen
Organism-Specific Regimens (Harrison's 22E)
| Organism | Preferred | Alternative |
|---|---|---|
| MSSA | Nafcillin/oxacillin 2g IV q6h → Rifampin + levofloxacin PO | Cefuroxime (penicillin allergy) |
| MRSA | Vancomycin 15mg/kg IV q12h or daptomycin 8–10mg/kg IV q24h → Rifampin + levofloxacin | TMP-SMX or fusidic acid |
| Streptococcus | Penicillin G 5MU IV q6h or ceftriaxone 2g IV q24h → rifampin PO | — |
| Enterobacteriaceae (quinolone-susceptible) | Ciprofloxacin 750mg PO q24h | TMP-SMX or fusidic acid |
| P. aeruginosa | Cefepime/ceftazidime 2g q8h + aminoglycoside × 2–4 weeks → ciprofloxacin 750mg PO q12h | Pip-tazo + aminoglycoside |
| Anaerobes | Clindamycin 600mg IV q6–8h → clindamycin 300mg PO q6h | Metronidazole (gram-negative anaerobes) |
Unless otherwise indicated, total duration is generally 6 weeks.
Note on rifampin: Rifampin + fluoroquinolone is active against staphylococcal biofilms — critical in device-related or implant-associated osteomyelitis. In settings with high rifampin resistance, debridement with implant retention has poor cure rates.
Local Antibiotic Delivery
- PMMA antibiotic beads/spacers (non-biodegradable) — provide very high local concentrations
- Biodegradable carriers (calcium sulfate, polytrimethylene carbonate/PTMC) — degrade cleanly without acidic byproducts; PTMC provides constant antibiotic release over time
- Local delivery supplements but does not replace systemic antibiotics
4. Adjunctive Therapies
- Hyperbaric oxygen (HBO): Controversial; not routinely recommended. May have a role in refractory cases with compromised vascularity — Goldman-Cecil Medicine
- Nutritional support: Critical preoperatively; malnutrition is a Type C host factor
- Vascular assessment: Arterial revascularization should be performed when vascular insufficiency is present (especially diabetic foot osteomyelitis) — Goldman-Cecil Medicine
- Negative pressure wound therapy (VAC): May assist wound management between staged procedures
Special Situations
Diabetic Foot Osteomyelitis
- Surgical consultation mandatory
- Medical therapy ± limited débridement for mild-moderate infection
- Surgical resection typically required for severe infection
- Role of adjunctive rifampin is uncertain
- Arterial revascularization essential if vascular supply is compromised
Hardware-Associated Osteomyelitis
- If hardware is stable and fracture unhealed: retain hardware + aggressive debridement + antibiotics
- If hardware is unstable: remove and replace (external fixation may be needed)
- If osteomyelitis in a healed fracture: remove all hardware + necrotic tissue
Vertebral Osteomyelitis
- Typically does not require surgery; treat with 6 weeks IV antibiotics
- Surgery indicated for: neurologic compromise, significant instability, large epidural abscess, intractable pain, or failure of medical treatment
Complications of Untreated/Recurrent Disease
- Septic arthritis from local extension
- Pathologic fracture
- Squamous cell carcinoma arising in a chronic sinus tract (Marjolin's ulcer)
- Secondary amyloidosis (AA amyloid)
- Primary bone malignancy
- — Goldman-Cecil Medicine
Monitoring Response
- CRP is the most reliable marker for monitoring treatment progress (more reliable than ESR)
- Serial imaging (MRI, plain radiographs) to assess healing
- Recurrence suggests inadequate debridement or antimicrobial resistance
Key sources:
- Harrison's Principles of Internal Medicine 22E (2025)
- Rockwood & Green's Fractures in Adults, 10th Ed. (2025)
- Goldman-Cecil Medicine
- Miller's Review of Orthopaedics 9th Ed.
- Schwartz's Principles of Surgery, 11th Ed.
- Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.