hlo
Hey! How can I help you today?
ARF
Reading File
Finding Sources
Searching PubMed
"acute kidney injury" management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Acute Renal Failure (ARF) / Acute Kidney Injury (AKI):
Acute Renal Failure (ARF) / Acute Kidney Injury (AKI)
ARF is the older term; AKI is now the preferred name. It refers to a rapid (hours to days) decline in kidney function, resulting in progressive azotemia and disruption of fluid, electrolyte, and acid-base balance.
Definition
The hallmark of AKI is progressive azotemia - accumulation of nitrogenous waste products (BUN, creatinine). When glomerular filtration abruptly ceases, serum creatinine typically rises by 1-2 mg/dL per day.
Classification (3 Categories)
| Category | Mechanism | Common Causes |
|---|---|---|
| Prerenal | Reduced renal blood flow / perfusion | Heart failure, hepatic failure, dehydration, burns, sepsis, shock |
| Intrinsic (Renal) | Parenchymal damage | ATN, AIN, glomerulonephritis, rhabdomyolysis, contrast nephropathy |
| Postrenal | Obstruction of urine flow | BPH, bilateral ureteric obstruction, bladder outlet obstruction |
Diagnostic Approach
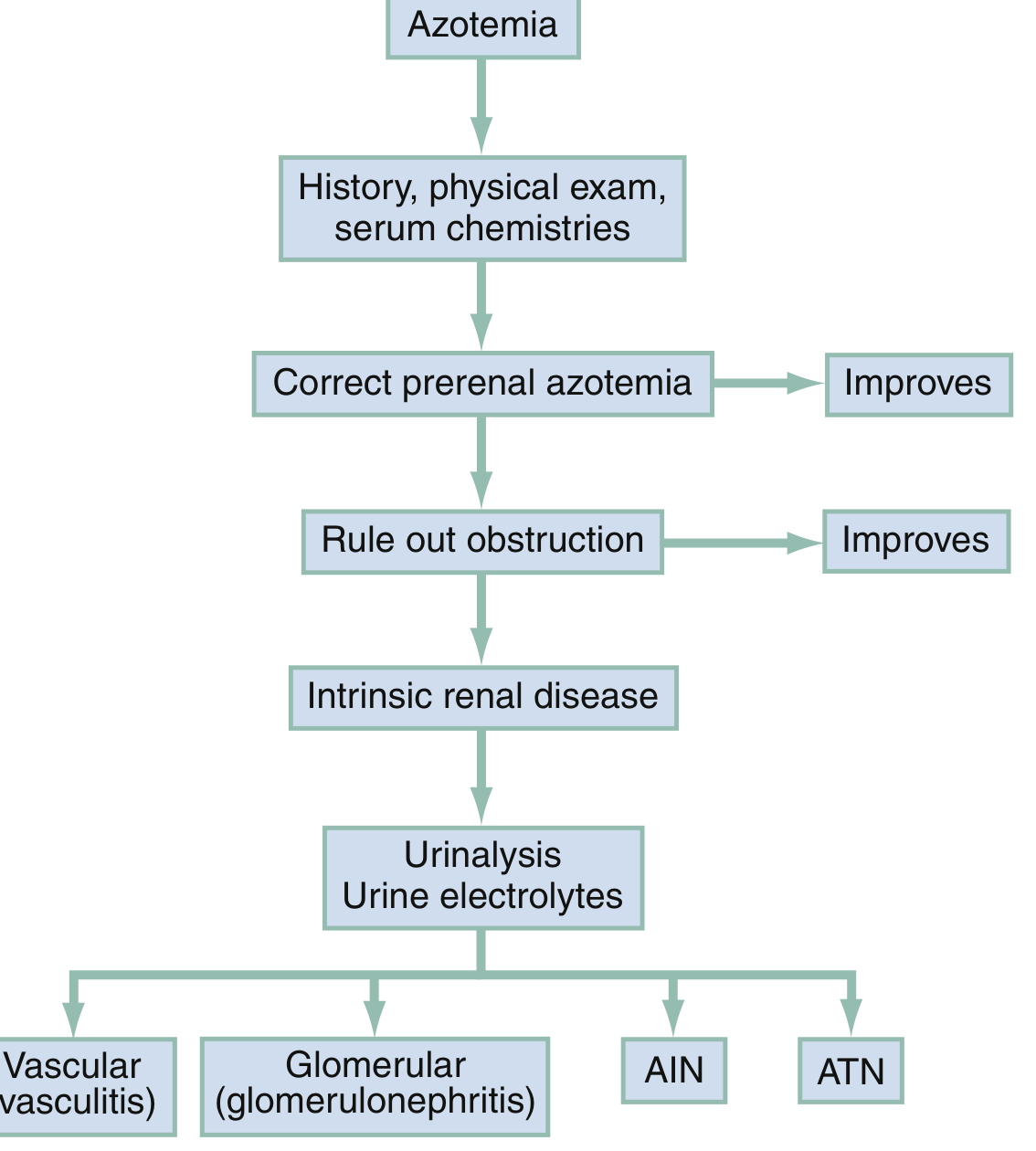
Fig. Evaluation of azotemia - Rosen's Emergency Medicine
Step 1: Rule out prerenal causes (correct volume, improve cardiac output)
Step 2: Rule out postrenal obstruction (ultrasound, bladder scan)
Step 3: If both excluded → intrinsic renal disease → urinalysis + urine electrolytes to distinguish vascular, glomerular, AIN, or ATN
Key Diagnostic Labs
| Parameter | Prerenal | Intrinsic (ATN) | Postrenal |
|---|---|---|---|
| Urine Na | < 20 mEq/L | > 40 mEq/L | Variable |
| FENa | < 1% | > 2% | Variable |
| BUN:Cr ratio | > 20:1 | ~10:1 | Variable |
| Urine specific gravity | High (> 1.020) | Low (~1.010) | Variable |
| Urine casts | Hyaline casts | "Muddy brown" granular casts (ATN) | None |
| Urine output | Oliguria | Oliguric or non-oliguric | Anuria/polyuria |
Clinical Features (Systemic Complications)
- Cardiovascular: Pulmonary edema, hypertension, arrhythmia, pericarditis
- Metabolic: Hyperkalemia, metabolic acidosis, hypocalcemia, hyperphosphatemia, hypermagnesemia
- Neurologic: Asterixis, confusion, seizures, coma
- GI: Nausea/vomiting, GI bleeding (~10% of patients), pancreatitis
- Hematologic: Normocytic anemia, platelet dysfunction/bleeding diathesis
- Infectious: Increased susceptibility - pneumonia, septicemia, UTI
The most rapidly lethal complication of AKI is hyperkalemia.
Most Common Intrinsic Cause: Acute Tubular Necrosis (ATN)
ATN is the most common intrinsic cause. It arises from:
- Ischemia - shock, sepsis, severe prolonged prerenal azotemia
- Nephrotoxins:
- Aminoglycoside antibiotics (gradual onset, typically after 1 week)
- Radiocontrast agents (creatinine rises within 3 days, returns to normal in 10-14 days)
- Myoglobinuria (rhabdomyolysis) - test serum CK, not just urine dipstick
- Hemoglobinuria
Risk factors for contrast nephropathy: Pre-existing renal insufficiency (most important), diabetes, age > 60, volume depletion, multiple myeloma, repeated contrast within 72 hours.
Management Principles
- First priority: Address life-threatening complications - hyperkalemia, pulmonary edema
- Treat the underlying cause (e.g., volume resuscitation for prerenal, relieve obstruction for postrenal)
- Avoid further renal insults - nephrotoxic drugs, contrast, hypotension
- Fluid management - avoid overload; monitor daily weights
- Drug dosing adjustment - many drugs require dose modification in renal failure
Indications for urgent dialysis (mnemonic: AEIOU)
- Acidosis (severe, refractory)
- Electrolyte disturbances (refractory hyperkalemia)
- Intoxication (certain toxins)
- Overload (fluid - pulmonary edema)
- Uremia (symptomatic - pericarditis, encephalopathy, bleeding)
Contrast nephropathy prophylaxis
- IV normal saline: 3 mL/kg over 1 hour before, then 1.5 mL/kg/hr for 4 hours after contrast
- Sodium bicarbonate has no advantage over saline
- N-acetylcysteine is not supported by current evidence
AKI vs CKD Differentiation
| Feature favoring CKD | Notes |
|---|---|
| Small kidneys on imaging | Most reliable |
| Bone changes of 2° hyperparathyroidism | Chronic marker |
Note: Anemia, hypocalcemia, and hyperphosphatemia can develop rapidly in AKI and should not be used alone to confirm CKD.
Sources: Rosen's Emergency Medicine, 9e; Harrison's Principles of Internal Medicine, 22e; Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.