Positive findings & PG level Physiotherapy assessment for brachial plexus injury & explain anatomy ,types & pathology of disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
"brachial plexus injury"[MeSH Terms] AND "physical therapy"[MeSH Terms]
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Searching the Web
physiotherapy assessment brachial plexus injury positive findings outcome measures PG level
I now have excellent material from all sources. Let me compile the comprehensive answer.
Brachial Plexus Injury: Anatomy, Types, Pathology & Physiotherapy Assessment
Part 1: Anatomy of the Brachial Plexus
The brachial plexus is a somatic nerve plexus formed by the anterior rami of C5 to T1 (sometimes with small contributions from C4 above or T2 below). It originates in the neck, passes laterally between the anterior and middle scalene muscles, crosses over the first rib, and enters the axilla. A useful mnemonic for its organization is "Real Texans Drink Cold Beer" (Roots - Trunks - Divisions - Cords - Branches).

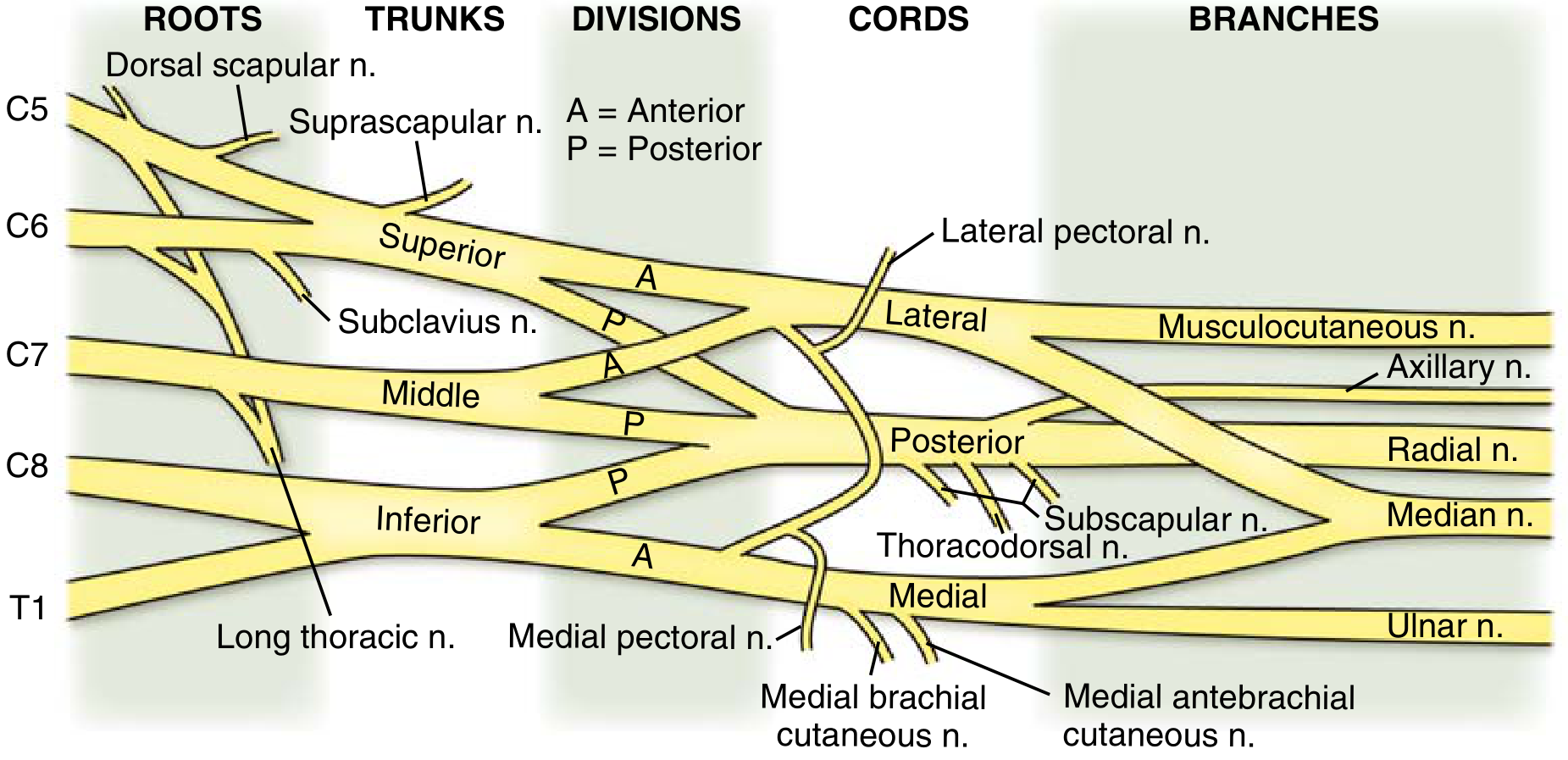
1.1 Roots (C5-T1)
- Anterior rami of C5, C6, C7, C8, T1
- Receive gray rami communicantes from the sympathetic trunk
- Pass between anterior and middle scalene muscles posterior to the subclavian artery
- Branches from the roots: Dorsal scapular nerve (C5) - rhomboids & levator scapulae; Long thoracic nerve (C5-7) - serratus anterior; Contribution to phrenic nerve (C5)
1.2 Trunks
| Trunk | Root Contributions |
|---|---|
| Superior | C5 + C6 |
| Middle | C7 (continuation) |
| Inferior | C8 + T1 |
- Branch from superior trunk: Suprascapular nerve (supraspinatus, infraspinatus), Nerve to subclavius
- The inferior trunk lies on rib I posterior to the subclavian artery
1.3 Divisions
Each trunk divides into anterior and posterior divisions (6 total):
- Anterior divisions supply flexor (anterior) compartments
- Posterior divisions supply extensor (posterior) compartments
- No peripheral nerves arise directly from the divisions
1.4 Cords (named by relationship to axillary artery)
| Cord | Formation | Root Values | Major Branches |
|---|---|---|---|
| Lateral | Anterior divisions of superior + middle trunks | C5-C7 | Lateral pectoral n., Musculocutaneous n., Lateral root of median n. |
| Medial | Continuation of anterior division of inferior trunk | C8-T1 | Medial pectoral n., Medial brachial cutaneous n., Medial antebrachial cutaneous n., Ulnar n., Medial root of median n. |
| Posterior | All 3 posterior divisions | C5-T1 | Upper/lower subscapular n., Thoracodorsal n., Axillary n., Radial n. |
1.5 Major Terminal Branches
- Musculocutaneous nerve (C5-7) - biceps, brachialis, coracobrachialis; lateral cutaneous forearm
- Median nerve (C5-T1) - flexors of wrist/fingers, thenar muscles; sensory over radial 3.5 fingers
- Ulnar nerve (C8-T1) - intrinsic hand muscles; sensory over ulnar 1.5 fingers
- Radial nerve (C5-T1) - extensors of wrist/fingers; posterior arm/forearm sensation
- Axillary nerve (C5-6) - deltoid, teres minor; lateral arm sensation
Part 2: Types and Classification of Brachial Plexus Injury
2.1 Seddon & Sunderland Classification (Pathological Basis)
| Seddon | Sunderland | Pathology | Recovery |
|---|---|---|---|
| Neuropraxia | Grade I | Focal demyelination. Axon intact. Conduction block | Full; weeks to 3 months |
| Axonotmesis | Grade II | Axon disrupted; endoneurium, perineurium, epineurium intact | Slow; by Wallerian regeneration ~1 mm/day |
| Axonotmesis | Grade III | Axon + endoneurium disrupted; perineurium + epineurium intact | Partial; misdirected regrowth possible |
| Axonotmesis | Grade IV | Axon + endoneurium + perineurium disrupted; epineurium intact | Poor without surgery |
| Neurotmesis | Grade V | Complete disruption of all nerve structures | No spontaneous recovery; requires surgery |
| - | Grade VI | Mixed injury - combination of grades | Variable |
- Neuropraxia - most common after mild traction or compression (e.g., "stinger" in sport)
- Axonotmesis - crush, traction injuries; Wallerian degeneration occurs distal to injury site
- Neurotmesis - complete transection; surgical repair required
Key: Fibrillations and fasciculations on EMG appear at 14+ days after injury (not before). Order EMG at 3 weeks post-closed injury to distinguish neuropraxia from more severe injuries. - Sabiston Textbook of Surgery
2.2 Anatomical / Level Classification
A. By Level of Injury
| Level | Description | Key Feature |
|---|---|---|
| Preganglionic (avulsion) | Root avulsion from spinal cord, proximal to dorsal root ganglion | No spontaneous recovery; Horner syndrome if C8-T1; pseudomeningocele on MRI |
| Postganglionic | Distal to dorsal root ganglion | May recover; nerve grafting possible |
B. By Clinical Pattern (Nerve Root Level)
Upper Plexus Palsy - Erb's Palsy (C5-C6, sometimes C7)
- Most common - birth trauma with excessive lateral neck-shoulder traction; motorcycle accidents
- Motor loss: shoulder abduction (deltoid), external rotation, elbow flexion (biceps), supination, wrist extension
- Classic posture: "Waiter's tip" - arm adducted & internally rotated, elbow extended, wrist flexed, forearm pronated
- Sensory loss: lateral arm, lateral forearm (musculocutaneous), thumb
- Reflexes: absent biceps (C5) and brachioradialis (C6)
- Sensation: C5-C6 dermatomes
Lower Plexus Palsy - Klumpke's Palsy (C8-T1)
- Rare; excessive arm abduction (traction injury with arm overhead)
- Motor loss: intrinsic hand muscles (interossei, hypothenar, thenar), wrist flexors
- Sensory loss: medial forearm, ulnar hand and digits
- Associated: Horner syndrome (ptosis, miosis, anhidrosis, enophthalmos) if T1 preganglionic injured → sympathetic chain disruption
- Reflexes: absent finger flexor reflex
Total (Pan) Plexus Palsy (C5-T1)
- Complete flail limb with global sensory loss
- Worst prognosis
- Often associated with avulsion injuries; Horner syndrome common
Middle Trunk Palsy (C7)
- Isolated C7: weakness of elbow extension (triceps), wrist extension, finger extension; less common in isolation
Part 3: Pathology and Mechanisms
3.1 Etiology
- Traction/stretch - most common; motorcycle accidents, fall on shoulder (downward traction), shoulder dystocia in obstetric injury (Erb's palsy)
- Compression - tumors (e.g., Pancoast tumor), hematoma, post-irradiation
- Direct trauma - stab wounds, gunshot injuries, clavicle fractures, shoulder dislocation
- Obstetric injury - large-for-dates baby, shoulder dystocia, instrumental delivery
- "Stinger/Burner" - sports injury, transient unilateral neuropraxia; burning pain radiating down the arm
3.2 Pathological Changes
After axon disruption (axonotmesis/neurotmesis):
- Wallerian degeneration occurs distal to the injury site within 48-72 hours
- Schwann cells proliferate and form Bands of Büngner to guide regenerating axons
- Axonal regeneration proceeds at approximately 1-4 mm/day
- Prolonged denervation leads to irreversible muscle fibrosis (>12-18 months)
- Fibrillations/fasciculations appear on EMG at ~14 days post-injury
3.3 Preganglionic vs Postganglionic Distinctions
| Feature | Preganglionic (Avulsion) | Postganglionic |
|---|---|---|
| Horner Syndrome | Present (if C8-T1) | Absent |
| Pseudomeningocele | Present on MRI | Absent |
| Histamine test | Axon flare present (DRG intact) | Absent flare |
| Tinel sign | Absent (no regeneration) | Present if regenerating |
| Surgical repair | Nerve transfer only (no graft) | Nerve graft/repair possible |
| Sensory nerve action potential (SNAP) | Preserved (DRG intact) despite clinical loss | Absent |
Part 4: Physiotherapy Assessment (PG-Level - Comprehensive)
A systematic physiotherapy assessment follows the SOAP/ICF framework covering impairment, activity limitation, and participation restriction.
4.1 Subjective Assessment (History)
Chief Complaint & History of Present Illness:
- Mechanism of injury (traction, compression, penetrating, birth)
- Time since injury (acute <3 weeks vs. subacute/chronic)
- Onset: sudden vs. gradual (tumor compression is gradual)
- Dominant hand
- Occupation and functional demands
- Presence and character of pain: burning/neuropathic, shooting, constant vs. episodic
- Numbness, tingling (paraesthesia), hypersensitivity
- Prior treatments, surgeries
Red Flags to Screen:
- Signs of spinal cord involvement (bilateral symptoms, bladder/bowel changes)
- Horner syndrome symptoms (ptosis, unequal pupils)
- Signs of vascular injury
4.2 Objective Assessment - Positive Findings & Tests
A. Observation / Inspection
| Finding | Significance |
|---|---|
| Waiter's tip posture | Upper plexus (C5-C6) lesion - Erb's palsy |
| Claw hand | Lower plexus (C8-T1) - Klumpke's; intrinsic minus hand |
| Flail limb | Total plexus palsy |
| Ptosis + miosis (Horner's) | Preganglionic T1 root avulsion |
| Winging of scapula | Long thoracic nerve (C5-7) injury - serratus anterior paralysis |
| Muscle wasting | Chronic denervation atrophy; deltoid wasting = axillary nerve injury |
| Skin changes | Anhydrosis, trophic changes indicate sympathetic involvement |
| Scars / deformities | History of trauma, previous surgery |
B. Anthropometric / Girth Measurement
- Circumferential measurements of arm and forearm (bilaterally) to quantify atrophy
C. Range of Motion (ROM) Assessment
- Passive ROM (PROM) and Active ROM (AROM) measured by goniometry at:
- Shoulder: flexion, abduction, ER/IR, horizontal adduction
- Elbow: flexion/extension, supination/pronation
- Wrist: flexion/extension, radial/ulnar deviation
- Fingers and thumb: all joints
- Compare bilaterally; document contractures
D. Manual Muscle Testing (MMT) - Oxford/MRC Scale
| Grade | Description |
|---|---|
| 0 | No contraction |
| 1 | Trace contraction - visible/palpable |
| 2 | Movement with gravity eliminated |
| 3 | Movement against gravity |
| 4 | Movement against gravity with some resistance |
| 5 | Normal strength |
Key muscles tested by root level:
| Root | Muscle | Action |
|---|---|---|
| C5 | Deltoid, Supraspinatus | Shoulder abduction |
| C5-6 | Biceps | Elbow flexion, supination |
| C6 | Wrist extensors (ECRL, ECRB) | Wrist extension |
| C7 | Triceps, wrist flexors, finger extensors | Elbow/wrist/finger extension |
| C8 | FDP, FDS | Finger flexion |
| T1 | Intrinsic hand muscles (interossei) | Finger abduction/adduction |
Positive Findings in Specific Palsies:
- Erb's (C5-C6): Grade 0-1 deltoid, biceps; Grade 0-1 supraspinatus; wrist/hand muscles relatively spared
- Klumpke's (C8-T1): Intrinsic hand paralysis; positive Froment's sign (thumb IP flexion during lateral pinch); clawing of ring and little fingers
- Pan-plexus: All muscles Grade 0-2
E. Sensory Assessment
| Test | Positive Finding | Significance |
|---|---|---|
| Light touch (cotton wool) | Absent/reduced over C5-T1 dermatomes | Sensory root affected |
| Pain (pinprick) | Absent/reduced | Spinothalamic disruption |
| Two-point discrimination (2PD) | >6 mm static 2PD on fingertips | Loss of median/ulnar nerve function |
| Semmes-Weinstein Monofilaments | Threshold elevated | Quantifies sensory impairment severity |
| Temperature discrimination | Impaired | Sympathetic/sensory fiber involvement |
| Proprioception/vibration | Reduced | Posterior column/large fiber involvement |
Dermatome Map (Key Areas):
- C5: Lateral arm (over deltoid)
- C6: Lateral forearm, thumb, index finger
- C7: Middle finger
- C8: Ring/little finger, medial forearm
- T1: Medial arm
F. Reflex Testing
| Reflex | Root | Positive Finding (Absence/Reduction) |
|---|---|---|
| Biceps reflex | C5-C6 | Absent in upper plexus palsy |
| Brachioradialis reflex | C5-C6 | Absent in upper plexus palsy |
| Triceps reflex | C7-C8 | Absent in C7 injury |
| Finger flexor reflex | C8-T1 | Absent in lower plexus palsy |
G. Special Clinical Tests
| Test | Technique | Positive Finding | Significance |
|---|---|---|---|
| Tinel's Sign | Percussion over the nerve course from distal to proximal | Tingling/electric shock in nerve distribution | Indicates disrupted axons; advancing Tinel indicates regeneration |
| Spurling's Test | Ipsilateral lateral flexion + axial compression | Reproduction of radicular symptoms | Cervical root compression (distinguish from plexus) |
| Roos Stress Test (EAST) | Arms abducted 90°, elbows 90°, repeated opening-closing of fist for 3 min | Arm fatigue, pain, tingling within 3 min | Thoracic outlet syndrome / proximal compression |
| Adson's Test | Deep breath, neck extension + rotation to affected side; radial pulse monitored | Diminished radial pulse | Subclavian artery compression in scalene triangle |
| Allen Test | Head turned away, radial pulse assessment | Obliteration of pulse | Costoclavicular compression |
| Elbow flexion test | Fully flex elbow for 5 min | Tingling in ulnar distribution | Cubital tunnel syndrome (differential) |
| Napkin ring sign | Pinching between thumb and index finger | Patient uses FPL instead of FPB (positive Froment's) | Ulnar nerve injury (intrinsic loss) |
| Wartenberg's sign | Little finger abducted at rest | Unable to adduct | Ulnar nerve injury |
| Wright's hyperabduction test | Shoulder passively abducted and externally rotated | Diminished pulse or symptoms | Subcoracoid compression |
| Abduction sign (Horner's) | Inspect eye on affected side | Ptosis + miosis + enophthalmos | Preganglionic T1 avulsion |
H. Functional Assessment Tests & Outcome Measures
| Scale | What It Measures | Use |
|---|---|---|
| Mallet Scale (modified) | Shoulder function in OBPP - 5 domains (abduction, ER, hand-to-mouth, hand-to-neck, hand-to-spine) graded I-V | Gold standard for obstetric BPI |
| Active Movement Scale (AMS) | 15 movements scored 0-7; gravity eliminated (0-3) vs. against gravity (4-7) | Neonatal/pediatric OBPP |
| MRC Scale (0-5) | Muscle strength grading | Universal motor assessment |
| Brachial Plexus Outcome Measure (BPOM) | 11 activity tasks; Functional Movement Scale 1-5; + self-evaluation VAS for hand/arm function | School-age OBPP children |
| DASH / QuickDASH | Disabilities of Arm, Shoulder and Hand - 30 items | Adult traumatic BPI |
| VAS / NRS | Pain intensity 0-10 | Pain assessment at all stages |
| Semmes-Weinstein Monofilament Test | Sensory threshold mapping | Quantitative sensory assessment |
| Grip and Pinch Dynamometry | Hand strength (kg) | Functional outcome |
| Nine-Hole Peg Test | Fine motor dexterity - time to complete | Adult BPI functional assessment |
I. Electrodiagnostic Studies (Ordered/Interpreted by Physiotherapist in collaboration)
| Test | Timing | Positive Finding | Significance |
|---|---|---|---|
| EMG | ≥3 weeks post-injury | Fibrillations, positive sharp waves, absence of motor unit potentials | Active denervation |
| Nerve Conduction Studies (NCS) | ≥3-4 days for CMAP | Absent CMAP distal to lesion; preserved SNAP in avulsion | Localization; preganglionic vs. postganglionic |
| SNAP (Sensory nerve action potential) | Acute | Present despite sensory deficit = preganglionic avulsion | Critical for surgical decision-making |
J. Imaging (Relevant to Physiotherapy Assessment)
| Modality | Positive Findings |
|---|---|
| MRI (MR Neurography) | Pseudomeningocele = root avulsion; nerve thickening/edema; post-surgery nerve graft assessment |
| High-resolution Ultrasound | Nerve discontinuity, thickening, loss of fascicular pattern; neuroma formation |
| X-ray | Clavicle fracture, first rib fracture, shoulder dislocation associated with BPI |
4.3 Physiotherapy Findings Summary by Injury Level
| Level | Motor Loss | Sensory Loss | Reflexes Lost | Special Sign |
|---|---|---|---|---|
| C5-C6 (Erb's) | Deltoid, Biceps, Supraspinatus, Brachioradialis | Lateral arm, lateral forearm, thumb | Biceps, Brachioradialis | Waiter's tip posture |
| C7 | Triceps, wrist extensors, finger extensors | Middle finger | Triceps | Wrist drop |
| C8-T1 (Klumpke's) | Intrinsic hand, wrist/finger flexors | Medial forearm, ulnar hand | Finger flexors | Claw hand + Horner's |
| C5-T1 (Pan-plexus) | Complete upper limb | Complete C5-T1 | All | Flail limb + Horner's |
4.4 Assessment of Specific Functional Deficits
Pain Assessment:
- Neuropathic pain is common even with avulsion injuries - burning, allodynia, hyperalgesia
- Use VAS/NRS for intensity; DN4 questionnaire for neuropathic character
Oedema/Swelling:
- Volumetric measurement or figure-of-8 taping technique
- Dependent oedema from flail limb
Postural Assessment:
- Scoliosis, cervical posture (C-spine involvement)
- Shoulder girdle position
- Winging of scapula (long thoracic nerve)
Gait (if bilateral or associated spinal cord injury):
- Antalgic posture, arm swing asymmetry
4.5 Differential Diagnosis (Assessment Considerations)
| Condition | Key Differentiating Feature |
|---|---|
| Cervical radiculopathy | Positive Spurling's; neck pain dominant; bilateral rare |
| Thoracic Outlet Syndrome | Postural; vascular tests positive (Adson's, Roos) |
| Pancoast tumor | Gradual onset; Horner's; chest X-ray/CT shows apical mass |
| Shoulder pathology (RC tear) | Normal sensation; MRI shoulder positive; no neurological deficit |
| Carpal tunnel syndrome | Median nerve distribution only; Phalen's, Tinel's at wrist |
Part 5: Rehabilitation Goals (PG-Level Framework)
Acute Phase (<6 weeks):
- Pain management (TENS, splinting, gentle positioning)
- Prevent contractures - PROM exercises
- Sensory re-education begins
- Oedema management
Subacute Phase (6 weeks - 6 months):
- Progressive active-assisted ROM as innervation returns
- Splinting (dynamic/static to prevent deformity - e.g., cock-up splint for wrist drop)
- EMG biofeedback for motor re-education
- Proprioceptive neuromuscular facilitation (PNF) techniques
- Sensory re-education
Chronic/Functional Phase (>6 months):
- Task-specific functional training
- Strengthening (progressive resistance)
- Compensatory strategies
- Vocational rehabilitation
- Outcome measures re-administered (DASH, VAS, grip strength)
Sources: Gray's Anatomy for Students (p. 858-859); Miller's Review of Orthopaedics 9th Ed (p. 155-156); Sabiston Textbook of Surgery (p. 807); Bradley and Daroff's Neurology in Clinical Practice (p. 2870); Campbell's Operative Orthopaedics 15th Ed 2026; Frontiers in Neurology - Review of Rehabilitation Protocols for BPI (2023)
Physiotherapy management
Finding Sources
Finding Sources
Searching the Web
physiotherapy management brachial plexus injury rehabilitation protocol phases exercises splinting PNF
Searching PubMed
"brachial plexus injury" AND rehabilitation
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC10150106
Finding Sources
Finding Sources
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.