Juvenile diabetes mellitus
Reading File
Finding Sources
Finding Sources
Searching PubMed
"type 1 diabetes mellitus"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Searching PubMed
"type 1 diabetes"[MeSH Terms] AND treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive material. Let me compile the full answer.
Juvenile Diabetes Mellitus (Type 1 Diabetes Mellitus - T1DM)
Definition and Terminology
Juvenile diabetes mellitus - now formally called Type 1 Diabetes Mellitus (T1DM) - is an autoimmune disease characterized by immunologically mediated destruction of pancreatic beta (β) cells, resulting in absolute insulin deficiency and chronic hyperglycemia. The term "juvenile" reflects its predominance in childhood and adolescence, though the older names "insulin-dependent diabetes" and "juvenile-onset diabetes" are no longer preferred because they are not pathognomonic. T1DM accounts for 5-10% of all diabetes cases and is the most common type diagnosed in patients younger than 20 years.
- Fischer's Mastery of Surgery 8e; Robbins & Kumar Basic Pathology
Stages of Development
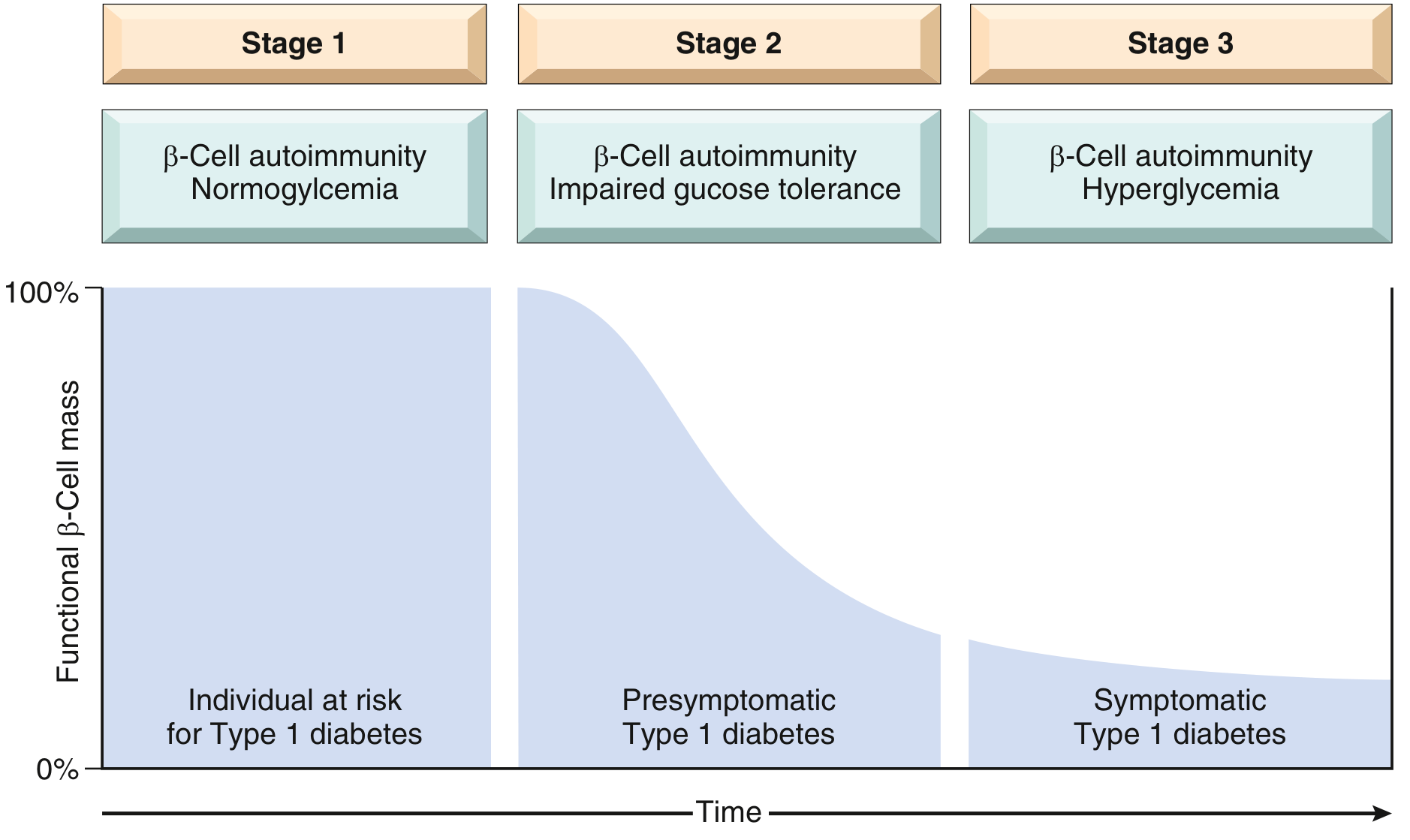
The autoimmune attack begins years before clinical symptoms, and classic manifestations appear only after >90% of β cells have been destroyed. Three recognized stages are shown below:
| Stage | Features |
|---|---|
| Stage 1 | β-cell autoimmunity present; normoglycemia; individual "at risk" |
| Stage 2 | β-cell autoimmunity + impaired glucose tolerance; presymptomatic T1DM |
| Stage 3 | β-cell autoimmunity + overt hyperglycemia; symptomatic T1DM |
- Robbins & Kumar Basic Pathology
Pathogenesis
Genetic Susceptibility
- Over 20 susceptibility loci identified by genome-wide association studies
- Strongest association: MHC class II HLA-DR genes - 90-95% of European-descent T1DM patients carry HLA-DR3 and/or DR4 (vs. ~40% of unaffected subjects); 40-50% of patients are DR3/DR4 heterozygotes vs. only 5% of unaffected individuals
- Additional susceptibility: polymorphisms in CTLA4, PTPN22 (both inhibit T-cell responses - loss-of-function alleles promote excessive T-cell activation), and the insulin gene (VNTR polymorphisms reduce thymic insulin expression, impairing elimination of autoreactive T cells)
Immune Mechanism
- Fundamental defect: failure of self-tolerance in T cells specific for β-cell antigens
- Mechanism: defective deletion of self-reactive T cells in thymus (central tolerance) + abnormal regulatory T cells (peripheral tolerance)
- Destruction mediated by cytotoxic T cells (CD8+) reacting against β-cell antigens (Type IV hypersensitivity)
- Autoantibodies detected against: insulin, glutamic acid decarboxylase (GAD65), tyrosine phosphatases IA-2 and IA-2β, and ZnT8 - found in 85-90% of patients; these are markers but not the primary effectors of damage
- Histology: "insulitis" - lymphocytic infiltration (T cells and macrophages) with β-cell necrosis
Environmental Triggers
-
Viral infections (notably coxsackievirus) have been implicated
-
Microbiome changes may play a role
-
Their exact mechanisms remain unclear
-
Robbins & Kumar Basic Pathology; Symptom to Diagnosis 4e
Comparison: T1DM vs T2DM
| Feature | Type 1 DM | Type 2 DM |
|---|---|---|
| Onset | Usually childhood/adolescence | Usually adulthood (increasing in youth) |
| Body habitus | Nonobese; may lose weight before diagnosis | 80% obese |
| Insulin levels | Progressive decrease (absolute deficiency) | Increased early; decreased late |
| Autoantibodies | Present (anti-GAD65, anti-IA2, anti-ZnT8) | Absent |
| Acute crisis | Diabetic ketoacidosis (DKA) | Nonketotic hyperosmolar coma |
| HLA linkage | MHC class II (HLA-DR3/DR4); CTLA4; PTPN22 | No HLA linkage; TCF7L2, PPARG, FTO |
| Pathology | Insulitis; β-cell depletion and islet atrophy | Amyloid deposition; mild β-cell depletion |
| Pathogenesis | T-cell autoimmunity against islet antigens | Insulin resistance + β-cell dysfunction |
- Robbins Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology
Risk Factors and Genetics
-
General population risk: 0.4%
-
Siblings/children of affected: 5-6%
-
Monozygotic twins: ~30-50% concordance (demonstrating both genetic and environmental contributions)
-
First-degree relatives: up to 10% chance of development
-
Associated autoimmune conditions: autoimmune thyroid disease, Addison disease, vitiligo, celiac disease, autoimmune hepatitis, myasthenia gravis, pernicious anemia
-
Symptom to Diagnosis 4e; Thompson & Thompson Genetics 9e
Clinical Presentation
Classic triad (from beta-cell destruction leading to hyperglycemia):
- Polyuria - osmotic diuresis from glucosuria
- Polydipsia - compensatory thirst
- Weight loss - despite polyphagia; due to loss of glucose in urine and catabolism
Diabetic Ketoacidosis (DKA) - the acute presentation in many children:
- Caused by the marked rise in the glucagon-to-insulin ratio with elevated cortisol
- Activates hormone-sensitive lipase → free fatty acid release → ketone body accumulation → metabolic acidosis
- Symptoms: excessive thirst, polyuria, nausea, vomiting, abdominal pain, weakness, altered consciousness (Kussmaul breathing, fruity breath)
Diagnosis
The diagnosis of diabetes is made by any one of the following (confirmed on a separate day except for classic hyperglycemic symptoms):
| Test | Diabetic Threshold |
|---|---|
| Fasting plasma glucose | ≥126 mg/dL |
| 2-hr plasma glucose (OGTT) | ≥200 mg/dL |
| Random plasma glucose with symptoms | ≥200 mg/dL |
| HbA1c | ≥6.5% |
-
T1DM-specific workup: positive islet autoantibodies (anti-GAD65, anti-IA2, anti-ZnT8), low/absent C-peptide
-
HLA typing in selected cases
-
Robbins & Kumar Basic Pathology
Treatment
Insulin Therapy (Always Required in T1DM)
T1DM requires lifelong insulin - there is no alternative. The standard regimen is a basal-bolus approach:
- Basal insulin (once or twice daily): long-acting insulins (glargine, detemir, degludec) - provides background coverage
- Bolus/prandial insulin (before meals): rapid-acting insulins (lispro, aspart, glulisine) - controls postmeal glucose spikes
- Total daily dose: typically 0.6-1.0 units/kg/day, divided between basal (~50%) and bolus (~50%)
Insulin delivery technologies:
- Insulin pumps (CSII - Continuous Subcutaneous Insulin Infusion): deliver programmed basal rates + patient-triggered boluses; reduce hypoglycemia and HbA1c
- Continuous Glucose Monitors (CGM): provide real-time glucose readings with alerts; when combined with pumps = "closed-loop" or "artificial pancreas" systems
- In 2021, the FDA approved commercial pancreatic islet transplantation (CellTrans) for highly select individuals with severe hypoglycemia unawareness
Glycemic Targets
-
HbA1c target: generally <7% (ADA) in adults; <7.5% in pediatric populations
-
The landmark Diabetes Control and Complications Trial (DCCT) demonstrated that tight glycemic control significantly reduces risk of microvascular complications (microalbuminuria, retinopathy, neuropathy)
-
Current Surgical Therapy 14e; Washington Manual of Medical Therapeutics; Rosen's Emergency Medicine
Chronic Complications
Microvascular (specific to diabetes; directly related to hyperglycemia)
| Complication | Key Features |
|---|---|
| Diabetic Retinopathy (DR) | Leading cause of blindness; preproliferative (microaneurysms, cotton-wool spots, hemorrhages) → proliferative (neovascularization). Screen T1DM patients 3-5 years after diagnosis, then annually. Treat with anti-VEGF agents or laser photocoagulation |
| Diabetic Nephropathy | Leading cause of ESRD in the US; affects 20-40% of T1DM patients. Microalbuminuria is the earliest marker. ACE inhibitors/ARBs are nephroprotective |
| Diabetic Neuropathy | Peripheral sensory neuropathy (glove-and-stocking pattern), autonomic neuropathy (gastroparesis, orthostatic hypotension, erectile dysfunction), mononeuropathy |
Macrovascular
-
Accelerated atherosclerosis: coronary artery disease, stroke, peripheral arterial disease, heart failure
-
T1DM patients have significantly elevated cardiovascular mortality
-
Washington Manual of Medical Therapeutics; Rosen's Emergency Medicine; Harrison's Principles 22e
Pancreas and Islet Transplantation
For carefully selected T1DM patients (especially those with severe hypoglycemia unawareness):
-
Whole-organ pancreas transplant: established therapy; most commonly performed simultaneously with kidney transplant (SPK) in patients with T1DM and ESRD; can achieve insulin independence
-
Islet cell transplantation: FDA-approved since 2021 as a commercial product (CellTrans) for select patients; less invasive but less durable than whole-organ transplant; limited to a few academic centers
-
Current Surgical Therapy 14e
Key Summary Points
- T1DM = autoimmune beta-cell destruction → absolute insulin deficiency
- Pathogenesis: HLA-DR3/DR4 genetic susceptibility + environmental triggers → loss of T-cell self-tolerance → insulitis → beta-cell destruction
- Autoantibodies (anti-GAD65, anti-IA2) are diagnostic markers; T-cell cytotoxicity is the effector
- Presents in childhood/adolescence with polyuria, polydipsia, weight loss; acute crisis is DKA
- Insulin replacement is lifelong and non-negotiable
- Tight glycemic control (HbA1c <7%) reduces microvascular complications (proven by DCCT)
- Associated with other autoimmune diseases (thyroid, adrenal, celiac)
- Twin concordance ~30-50% confirms both genetic and environmental contributions
I am a bsc nursing student so please according to pediatric nursing
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
juvenile diabetes type 1 pediatric nursing assessment interventions BSc nursing
Reading Web Page
https://www.mayoclinic.org/diseases-conditions/type-1-diabet…
Finding Sources
I now have all the content needed to write a thorough, BSc Nursing-focused pediatric response. Let me compile it now.
Juvenile Diabetes Mellitus - Pediatric Nursing (BSc Nursing)
1. Definition
Juvenile Diabetes Mellitus (Type 1 Diabetes Mellitus - T1DM) is a chronic autoimmune endocrine disorder in which the body's own immune system destroys the insulin-producing beta (β) cells of the pancreatic islets of Langerhans, resulting in absolute insulin deficiency and persistent hyperglycemia.
From a nursing perspective, T1DM is a lifelong condition requiring 24-hour management involving insulin therapy, blood glucose monitoring, diet, activity, and extensive patient/family education.
2. Epidemiology (Nursing Relevance)
- Accounts for 5-10% of all diabetes cases
- Most common type in persons under 20 years of age
- Can occur at any age but peaks at 5-7 years and during puberty (10-14 years)
- Incidence is rising worldwide
- Affects boys and girls equally
- Risk in siblings of affected children: 5-6%; monozygotic twins: ~30-50%
3. Etiology (Causes)
| Factor | Details |
|---|---|
| Genetic | HLA-DR3 and HLA-DR4 genes strongly linked; CTLA4 and PTPN22 polymorphisms |
| Autoimmune | T-lymphocytes attack β cells; autoantibodies (anti-GAD65, anti-IA2) in 85-90% of cases |
| Environmental triggers | Viral infections (coxsackievirus, enterovirus), early cow's milk exposure, gut microbiome changes |
| Family history | 1st-degree relatives at higher risk |
4. Pathophysiology (Simplified for Nursing)
Genetic susceptibility + Environmental trigger
↓
Autoimmune T-cell attack on β cells (INSULITIS)
↓
Progressive destruction of β cells (takes months to years)
↓
>90% β cells destroyed → Absolute insulin deficiency
↓
Glucose cannot enter cells → HYPERGLYCEMIA
↓
Body breaks down fat → KETONE production → DIABETIC KETOACIDOSIS (DKA)
The stages (as the nurse must understand the progression):
-
Stage 1: β-cell autoimmunity present, blood sugar still normal
-
Stage 2: β-cell autoimmunity + impaired glucose tolerance (presymptomatic)
-
Stage 3: Overt hyperglycemia + symptoms appear
-
Robbins & Kumar Basic Pathology
5. Clinical Manifestations in Children
A. Classic Triad ("Three Polys")
| Symptom | Mechanism |
|---|---|
| Polyuria (excessive urination) | Osmotic diuresis - glucose spills into urine, dragging water with it |
| Polydipsia (excessive thirst) | Loss of fluid causes thirst |
| Polyphagia (excessive hunger) | Cells starved of glucose signal hunger; yet child loses weight |
B. Other Common Symptoms in Children
- Unexplained weight loss despite eating well
- Fatigue and weakness
- Blurred vision (osmotic changes in lens)
- Enuresis (bedwetting) - new onset in previously dry child is a red flag
- Recurrent infections (fungal infections, skin infections)
- Irritability, mood changes, poor school performance
C. Diabetic Ketoacidosis (DKA) - Emergency Presentation
Many children present for the first time in DKA. Key signs:
| System | Signs/Symptoms |
|---|---|
| GI | Nausea, vomiting, abdominal pain |
| Respiratory | Kussmaul breathing (deep, rapid breathing); fruity/acetone breath |
| CNS | Headache, confusion, drowsiness, coma |
| Skin | Flushed, dry, warm skin; dry mucous membranes |
| CVS | Tachycardia, hypotension (if severe dehydration) |
| Urine | Glucosuria + ketonuria |
Nursing Alert: Any child presenting with vomiting + abdominal pain + rapid breathing - ALWAYS check blood glucose and urine ketones. DKA is life-threatening.
6. Nursing Assessment (Head-to-Toe)
History Collection
- Onset and duration of symptoms (polydipsia, polyuria, weight loss)
- Family history of diabetes or autoimmune disease
- Recent viral illness
- Dietary habits, growth chart, developmental milestones
- Previous health history, immunization status
Physical Assessment
| System | What to Assess |
|---|---|
| Vital signs | Tachycardia, hypotension, respiratory pattern (Kussmaul in DKA) |
| Weight/Height | Unexplained weight loss; compare to growth percentile charts |
| Skin | Turgor, dryness, injection site condition (if already on insulin) |
| Eyes | Visual acuity (blurred vision with hyperglycemia) |
| Mouth | Dry mucous membranes, fruity odor (acetone breath in DKA) |
| Abdomen | Tenderness (DKA), hepatomegaly |
| Neurological | Level of consciousness, irritability, confusion |
| Genitalia | Candidal rash/vaginitis (common with uncontrolled glucose) |
Diagnostic Assessment
| Test | Normal/Diabetic Value | Nursing Role |
|---|---|---|
| Fasting blood glucose | ≥126 mg/dL = diabetes | Collect fasting sample; explain procedure to child and parent |
| Random blood glucose | ≥200 mg/dL + symptoms = diabetes | - |
| HbA1c | ≥6.5% = diabetes; target <7.5% in children | Explain it reflects 3-month average |
| Urine ketones | Positive in DKA | Teach parents dipstick testing |
| Urine glucose | Glucosuria | - |
| C-peptide | Low/absent in T1DM | Distinguishes from T2DM |
| Autoantibodies (GAD65, IA-2) | Positive in T1DM | Confirm autoimmune cause |
| ABG/electrolytes | Metabolic acidosis in DKA | Monitor pH, bicarbonate, K+ closely |
7. Nursing Diagnoses (NANDA)
- Deficient Fluid Volume related to osmotic diuresis and vomiting (DKA)
- Imbalanced Nutrition: Less Than Body Requirements related to lack of insulin and cellular glucose starvation
- Risk for Unstable Blood Glucose Level related to inadequate insulin, diet non-compliance, illness
- Risk for Infection related to hyperglycemia impairing immune function
- Deficient Knowledge (child and family) related to new diagnosis and insulin management
- Anxiety/Fear (child and parents) related to new diagnosis and lifelong management
- Non-compliance (Risk for) related to child's developmental stage and lifestyle factors
- Risk for Injury related to hypoglycemia episodes
8. Nursing Interventions
A. Insulin Administration (Most Critical Nursing Action)
Children with T1DM always require insulin - no oral medications replace it.
Types of Insulin (must know for exams):
| Type | Onset | Peak | Duration | Examples | Use |
|---|---|---|---|---|---|
| Rapid-acting | 10-15 min | 1-2 hr | 3-5 hr | Lispro (Humalog), Aspart (NovoLog) | Given just before meals |
| Short-acting (Regular) | 30-60 min | 2-4 hr | 6-8 hr | Humulin R | Given 30 min before meals |
| Intermediate-acting | 1-2 hr | 4-12 hr | 12-18 hr | NPH (Humulin N) | Twice daily coverage |
| Long-acting (Basal) | 1-2 hr | Peakless | 20-24 hr | Glargine (Lantus), Detemir (Levemir), Degludec | Once daily; background coverage |
Basal-Bolus Regimen (standard in children):
- Basal insulin once daily (long-acting) = background coverage
- Bolus insulin before each meal (rapid-acting) = controls post-meal spikes
Nursing Points for Insulin Administration in Children:
- Rotate injection sites (abdomen, outer thigh, upper arm, buttocks) - document site rotation
- Injection sites in children: outer thigh and buttocks preferred (more subcutaneous fat)
- Inject at 90° angle (if adequate fat); at 45° in thin children
- Never massage injection site (alters absorption rate)
- Keep insulin vials at room temperature (in use); store extra in refrigerator (never freeze)
- Check insulin appearance: clear for regular/long-acting; cloudy for NPH (roll gently, never shake)
- Two-nurse verification recommended before giving insulin
B. Blood Glucose Monitoring
- Teach children and parents to perform self-monitoring of blood glucose (SMBG)
- Typical frequency: 4-6 times/day (before meals, 2 hours after meals, at bedtime, overnight)
- Target glucose ranges for children:
| Time | Target (mg/dL) |
|---|---|
| Before meals | 90-130 |
| 2 hours after meals | < 180 |
| Bedtime | 90-150 |
| HbA1c | < 7.5% (children) |
- Continuous Glucose Monitor (CGM): teach parents how to use; alerts for high/low glucose
- Document all readings in a glucose log
C. Management of Hypoglycemia (Low Blood Sugar)
Most common acute complication in children on insulin. Must be recognized and treated immediately.
Causes in children: skipped/delayed meals, excess insulin, increased activity, illness with vomiting
Signs and Symptoms:
| Mild-Moderate | Severe |
|---|---|
| Shakiness, tremors | Seizures |
| Sweating, pallor | Loss of consciousness |
| Hunger | Unresponsiveness |
| Irritability, mood change | - |
| Headache, dizziness | - |
| Confusion, difficulty concentrating | - |
The "15-15 Rule" (Nursing Standard):
- Give 15 grams of fast-acting carbohydrate (4 oz juice, 3-4 glucose tablets, 1 tbsp sugar)
- Wait 15 minutes, recheck blood glucose
- If still < 70 mg/dL, repeat
- Once glucose normalizes, give a small snack (complex carb + protein)
- Never give food/liquid to unconscious child - give IV Dextrose (D25W or D50W) or IM Glucagon
Nursing Alert: Keep glucagon emergency kit available at all times. Teach parents and school nurse how to administer it.
D. Management of DKA (Emergency Care)
DKA is a medical emergency. Nursing priorities:
- Establish IV access - large-bore cannula
- IV fluid resuscitation: Normal saline (0.9% NaCl) - correct dehydration cautiously in children (risk of cerebral edema)
- Insulin infusion: Regular insulin IV infusion at 0.05-0.1 units/kg/hr (never give bolus in DKA)
- Monitor electrolytes: K+ levels carefully - insulin shifts K+ into cells, causing hypokalemia; replace potassium as needed
- ABG monitoring: Watch pH and bicarbonate levels
- Hourly vital signs + neuro checks: Watch for cerebral edema (headache, change in consciousness) - give mannitol if suspected
- Urine output monitoring: Insert catheter; target > 1 mL/kg/hr
- When blood glucose reaches 200-250 mg/dL: Add dextrose to IV fluids (to prevent hypoglycemia while continuing insulin)
- Transition to subcutaneous insulin once child is eating and ketones are cleared
E. Nutritional Management
- Diet planned by a registered dietitian with carbohydrate counting
- Carbohydrate counting is the key skill - insulin dose is matched to carbohydrate intake
- Regular meal schedule - no skipping meals; consistent carbohydrate intake
- Encourage fiber-rich foods, whole grains, lean protein
- Limit simple sugars, sweetened beverages
- Adjust diet for physical activity (additional snacks before exercise)
- No food should be completely forbidden - teach moderation and balance
- School meals: coordinate with school nurse; ensure child has snacks available
F. Exercise and Activity
- Exercise is beneficial and encouraged
- Monitor blood glucose before, during, and after exercise
- If glucose < 100 mg/dL before exercise - give carbohydrate snack first
- Carry fast-acting sugar (glucose tablets/juice) during exercise
- Reduce insulin dose before planned vigorous exercise (as per physician orders)
- Avoid strenuous exercise during ketoacidosis
9. Patient and Family Education (Priority Nursing Responsibility)
This is the most important long-term nursing intervention in pediatric T1DM.
Topics to Teach:
For Parents:
- How to measure blood glucose (glucometer use, CGM)
- How to draw and inject insulin correctly
- Recognition and treatment of hypoglycemia and hyperglycemia
- Sick-day rules (never stop insulin; check glucose/ketones more frequently when ill)
- When to call the doctor/go to hospital
- Carbohydrate counting and meal planning
- Foot and skin care (long-term)
- Importance of wearing medical ID bracelet/tag
For the Child (age-appropriate teaching):
- Toddler/Preschool (1-5 years): Parents handle all management; child should be able to say "I have diabetes" and "I need sugar"
- School age (6-12 years): Teach child to recognize symptoms of hypoglycemia; can assist with glucose testing; gradually learn insulin injection with supervision
- Adolescent (13-18 years): Can independently manage glucose monitoring and insulin; teach impact of puberty (hormones raise insulin requirements), alcohol risks, peer pressure, sexual health
- Encourage independence gradually while maintaining parental oversight
School Coordination:
- Provide school nurse with a Diabetes Medical Management Plan (DMMP)
- Ensure teachers know symptoms of low/high blood sugar
- Child should be allowed to check blood sugar and take insulin at school
- Keep emergency glucagon kit at school
10. Complications - Nursing Monitoring
Acute Complications
| Complication | Key Feature | Nursing Action |
|---|---|---|
| Hypoglycemia | BG < 70 mg/dL; shakiness, sweating, confusion | 15-15 rule; glucagon for severe; prevent with regular meals |
| Diabetic Ketoacidosis (DKA) | BG > 250 + ketones + acidosis; Kussmaul breathing | IV fluids, insulin infusion, electrolyte monitoring |
| Hyperglycemic Hyperosmolar State | Rare in T1DM | Monitor glucose; hydrate |
Chronic Complications (Long-term Monitoring)
| Complication | Monitoring Frequency | Nursing Role |
|---|---|---|
| Diabetic Retinopathy | Annual eye exam (ophthalmologist) starting 3-5 yrs after diagnosis or at puberty | Reinforce importance of eye checks |
| Diabetic Nephropathy | Annual urine microalbumin + serum creatinine | Monitor urine output; reinforce good glucose control |
| Peripheral Neuropathy | Annual foot exam | Teach foot care; proper footwear |
| Cardiovascular disease | Annual BP, lipids | Lifestyle education |
| Celiac disease / thyroid disease | Periodic screening (associated autoimmune conditions) | Monitor growth, symptoms |
Tight glycemic control (HbA1c < 7.5%) is proven to delay and reduce all microvascular complications - reinforce this to families at every visit (DCCT trial evidence).
11. Psychological and Developmental Considerations
- Diabetes is a psychosocial burden for both child and family
- Children may feel different from peers, leading to poor self-esteem, depression
- Diabetes burnout is common in adolescents - non-compliance with insulin/monitoring
- Screen for depression and anxiety at every visit
- Encourage age-appropriate independence and normal social activities
- Diabetic camps: strongly recommended - children socialize with peers who have T1DM
- Refer to counselor or psychologist if needed
- Siblings may feel neglected due to attention on the diabetic child - address family dynamics
12. Special Situations in Pediatric Nursing
| Situation | Nursing Consideration |
|---|---|
| Illness/Fever | Never stop insulin; glucose rises with stress hormones; check ketones every 3-4 hrs; increase fluids |
| Growth spurts/Puberty | Insulin requirements increase significantly; HbA1c may worsen during puberty |
| Sports/PE class | Extra carbohydrate snack before; reduce insulin; carry glucose |
| Examinations/Stress | Cortisol raises blood glucose; may need insulin adjustment |
| Overnight hypoglycemia | Check 2-3 AM glucose; consider bedtime snack; adjust basal insulin |
| Picky eating (toddlers) | Never give insulin until child finishes meal; use rapid-acting insulin after meal |
13. Quick Summary Table for Exams
| Topic | Key Point |
|---|---|
| Type | Autoimmune; absolute insulin deficiency |
| Age | Children and adolescents (any age) |
| Classic symptoms | Polyuria, polydipsia, polyphagia + weight loss |
| Acute emergency | DKA - Kussmaul breathing, fruity breath, acidosis |
| Treatment | Insulin (always required); basal-bolus regimen |
| Monitoring | SMBG 4-6x/day; HbA1c every 3 months |
| Hypoglycemia Rx | 15-15 rule; glucagon for severe/unconscious |
| DKA Rx | IV Normal Saline + IV Regular Insulin + K+ replacement |
| Nursing priority | Patient/family education + insulin administration |
| HbA1c target | < 7.5% in children |
| Long-term complications | Retinopathy, nephropathy, neuropathy, CVD |
Important Nursing Principle: The nurse is not just a care-giver in T1DM - the nurse is an educator, coordinator, and advocate. Teaching the child and family to self-manage safely is the foundation of pediatric diabetic nursing care.
This is a shared conversation. Sign in to Orris to start your own chat.