Menopause and related problems. Replacement hormonal therapy Genital prolapse.
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
menopause hormone replacement therapy
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed. Here is a comprehensive, structured review:
Menopause, Hormone Replacement Therapy & Genital Prolapse
PART I: MENOPAUSE
Definition & Epidemiology
Menopause is the permanent cessation of menses, representing the culmination of reproductive aging. It is diagnosed retrospectively after 12 consecutive months of amenorrhea in the absence of other physiological or pathological causes. The median age is 52.5 years (range typically 45–55 years).
Menopause is a universal phenomenon in women, but the timing is influenced by several factors:
| Factor | Direction | Magnitude |
|---|---|---|
| Smoking | Earlier | 1–2 years |
| Low socioeconomic status | Earlier | 1–2 years |
| African American / Hispanic ethnicity | Earlier | ~2 years |
| High altitude / EDC exposure | Earlier | 1–4 years |
| Oral contraceptive use | Later | ~6 months |
| Higher parity | Later | Variable |
| Asian ethnicity | Later | 1–2 years |
| Fragile X / Mosaic Turner syndrome | Earlier | Variable |
EDCs = endocrine-disrupting chemicals. — Goldman-Cecil Medicine, Ch. 222
Pathophysiology
Throughout reproductive life, about 400 primordial follicles mature and ovulate; hundreds of thousands degenerate. By ~age 45, primordial follicle numbers approach zero. As follicles are depleted:
- Estrogen and progesterone production fall
- The negative feedback on the hypothalamic-pituitary axis is lost
- FSH and LH rise markedly (mainly FSH) — a hallmark of menopause
- Circulating estrogen falls to near zero
The perimenopause is the variable period (months to years) of irregular cycles before and around the final menstrual period.
Antimüllerian hormone (AMH) — synthesized by granulosa cells — is the most reliable proxy of ovarian reserve and can help approximate the timing of the final menstrual period. FSH and inhibin levels fluctuate too much to be reliably used for this purpose.
Clinical Features — Menopausal Symptoms
| Domain | Symptoms |
|---|---|
| Vasomotor | Hot flashes (flushes), night sweats, palpitations |
| Neurological/mood | Irritability, fatigue, anxiety, depression, cognitive fog |
| Genitourinary | Vaginal dryness, itching, burning, dyspareunia, urinary frequency, recurrent UTIs — collectively: Genitourinary Syndrome of Menopause (GSM) |
| Skeletal | Accelerated bone loss → osteoporosis |
| Metabolic | Increased cardiovascular risk, dyslipidemia |
| Sleep | Insomnia, night awakening (often driven by vasomotor symptoms) |
GSM, unlike hot flashes, does not resolve spontaneously over time — long-term treatment is often required.
Diagnosis
Menopause is a clinical diagnosis (12 months amenorrhea ≥40 years, no other cause). Investigations may include:
- Serum FSH (elevated, typically >40 IU/L) — confirms but is not required if clinical picture is clear
- Estradiol (low)
- AMH — useful for predicting timing in perimenopause
- Rule out pregnancy, thyroid disease, hyperprolactinaemia, premature ovarian insufficiency if age <40
PART II: HORMONE REPLACEMENT THERAPY (HRT)
Indications
HRT is indicated primarily for:
- Bothersome vasomotor symptoms (hot flashes, night sweats) — most common indication
- Genitourinary syndrome of menopause (local or systemic)
- Prevention of osteoporosis in women at high risk who cannot use other agents
- Premature ovarian insufficiency (POI) — until the natural age of menopause (~51 years)
Current guidelines state that only symptomatic treatment, as needed, is indicated for this normal life transition. Approximately 15% of women have symptoms severe enough to warrant treatment.
HRT Formulations
Estrogens (systemic):
- Oral: estradiol, conjugated equine estrogen (CEE)
- Transdermal: patches, gels, sprays (lower thromboembolic risk than oral)
- Vaginal (local/systemic): creams, rings, tablets, capsules
Progestogens (required for women with an intact uterus to protect endometrium):
- Medroxyprogesterone acetate (MPA), norethindrone, micronized progesterone
- Given cyclically (sequential) or continuously combined
Women without a uterus: estrogen-only therapy (ET); Women with a uterus: combined estrogen-progestogen therapy (EPT)
Other agents:
- Ospemifene — a SERM with estrogen receptor-β agonism; oral, for dyspareunia
- Dehydroepiandrosterone (DHEA) — intravaginal, for dyspareunia
- Tibolone — synthetic steroid with oestrogenic, progestogenic, androgenic activity (not available in all countries)
The "Timing Hypothesis" (Window of Opportunity)
This is a critical concept:
"Current evidence suggests that if hormone therapy is started before age 60, or within 10 years after menopause begins, the overall benefits of estrogen replacement therapy may outweigh the risks, especially for women who have a low risk for cardiovascular disease and breast cancer." — Guyton & Hall, Textbook of Medical Physiology
Evidence from the Women's Health Initiative (WHI) and subsequent re-analyses:
- HRT started early in menopause (within 10 years / before age 60) → net benefit likely
- HRT started late (>10 years post-menopause, age >60) in older women with subclinical atherosclerosis → potential cardiovascular harm
Benefits of HRT
| Benefit | Evidence |
|---|---|
| Relief of vasomotor symptoms | Best-established; ~80–90% reduction in hot flash frequency |
| Treatment of GSM | Very effective; local estrogen preferred for isolated vaginal symptoms |
| Prevention of osteoporosis / fracture | Well-established |
| Possible reduction in new-onset type 2 diabetes | Observational data |
| Possible cognitive / dementia benefit | If started near menopause (timing-dependent) |
| Relief of sleep and mood symptoms secondary to hot flashes | Effective |
Risks of HRT
| Risk | Agent | Comment |
|---|---|---|
| Breast cancer | EPT > ET | Slight increase with combined HRT; risk lower with micronized progesterone vs. synthetic progestins |
| Venous thromboembolism (VTE) | Oral estrogen > transdermal | Transdermal route largely avoids first-pass effect → lower VTE risk |
| Stroke | Oral estrogen | Transdermal has lower risk |
| Endometrial cancer | Estrogen alone (in intact uterus) | Prevented by adding progestogen |
| Cardiovascular disease | EPT (WHI): slight increase in MI risk | Mainly in older women; no increased risk when started early |
| Gallbladder disease | Oral estrogen | — |
Non-Hormonal Treatments for Vasomotor Symptoms
For women with contraindications to HRT or who prefer non-hormonal options:
| Drug | Mechanism | Notes |
|---|---|---|
| Fezolinetant | Neurokinin-3 receptor antagonist | FDA-approved; comparable efficacy to estrogen |
| Paroxetine mesylate (7.5 mg) | SSRI | Only FDA-approved non-hormonal for hot flashes |
| Venlafaxine, desvenlafaxine | SNRI | Good evidence; useful if depression coexists |
| Gabapentin | — | Moderate evidence |
| Clonidine | α₂-agonist | Modest benefit; side effects common |
| Cognitive-behavioural therapy (CBT) | — | ~50% reduction; recommended for all |
Yoga, exercise, black cohosh, and omega-3 fatty acids have been demonstrated ineffective in randomized trials. — Goldman-Cecil Medicine, Ch. 222
Contraindications to Systemic HRT
- History of breast cancer or estrogen-dependent cancer
- Unexplained vaginal bleeding
- Active or recent thromboembolic disease (DVT, PE)
- Active liver disease
- Uncontrolled hypertension
- Cardiovascular disease (use with caution; start only if early menopause)
- Pregnancy
Note: Local (vaginal) estrogen has minimal systemic absorption and is generally considered safe even in many women with relative contraindications to systemic HRT.
Cardiovascular Prevention & Osteoporosis
- Postmenopausal women carry cardiovascular risk equivalent to men ~10 years older; screening for hypertension and hyperlipidaemia is important
- HRT is not recommended to reduce cardiovascular risk as a primary indication
- For osteoporosis, bisphosphonates (alendronate, risedronate, zoledronic acid) are first-line alternatives if HRT is not appropriate
PART III: GENITAL (PELVIC ORGAN) PROLAPSE
Definition
Pelvic organ prolapse (POP) refers to the downward displacement of pelvic organs resulting in protrusion of the uterus and/or different vaginal compartments and surrounding organs (bladder, rectum, bowel). It results from loss of support of one or more compartments of the vagina.
Classification by Compartment
| Compartment | Prolapse | Old term |
|---|---|---|
| Anterior | Descent of anterior vaginal wall / bladder | Cystocele |
| Apical | Descent of uterus/cervix or vaginal cuff (post-hysterectomy) | Uterine prolapse / vault prolapse |
| Posterior | Descent of posterior vaginal wall / rectum | Rectocele |
| Apical + small bowel | Small intestine in rectovaginal space | Enterocele |
| Complete eversion | Total vaginal eversion + uterine prolapse | Procidentia |
The anterior compartment is the most commonly affected.
Risk Factors
- Vaginal delivery (especially instrumental/prolonged)
- Multiparity / high parity
- Increasing age
- Menopause / oestrogen deficiency (loss of collagen support)
- Obesity
- Chronic raised intra-abdominal pressure (chronic cough, constipation, heavy lifting)
- Prior pelvic surgery
- Connective tissue disorders (Marfan, Ehlers-Danlos)
- Family history
Symptoms
- Vaginal bulge felt or seen by the patient — the most specific symptom
- Pelvic pressure or discomfort
- Vaginal discharge
- Splinting (manual reduction of prolapse to void/defecate)
- Low backache
- Urinary symptoms: frequency, nocturia, incomplete emptying, voiding dysfunction
- Bowel symptoms: constipation, incomplete evacuation, straining
- Sexual dysfunction, dyspareunia
Important: There is poor correlation between symptom severity and prolapse stage. Many urinary/bowel symptoms are due to co-existing bladder or anorectal dysfunction rather than prolapse itself.
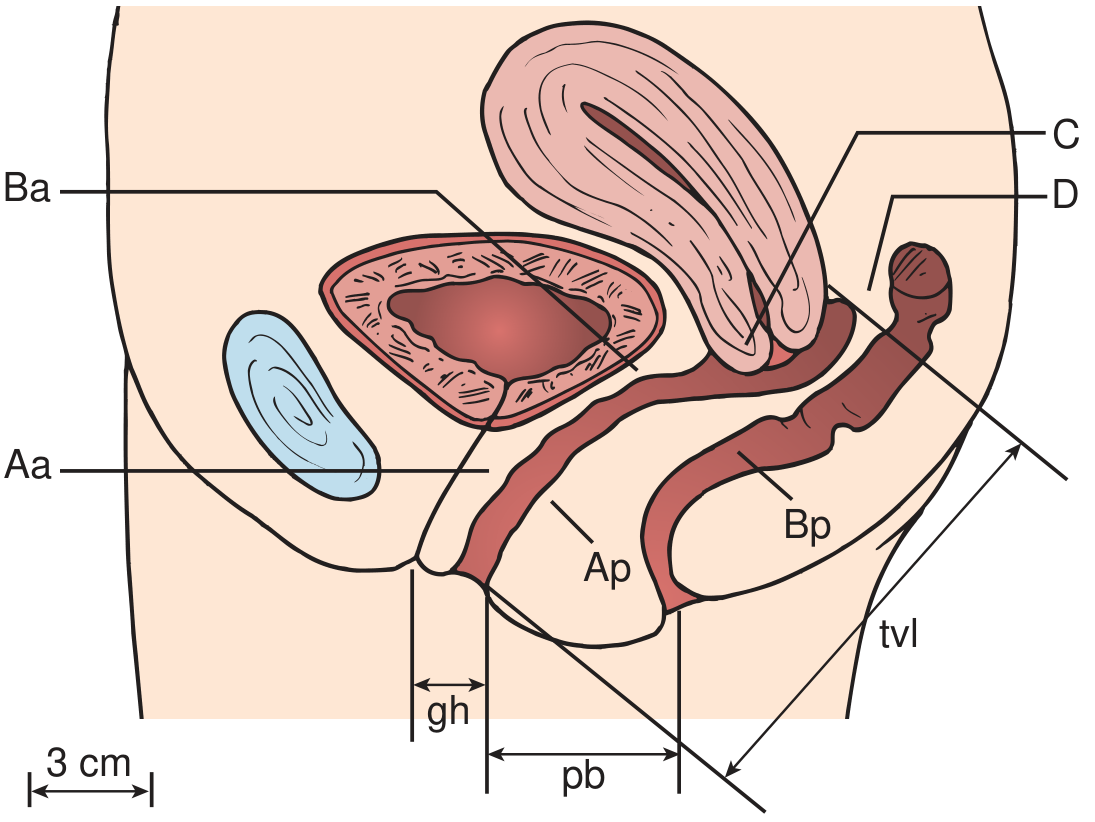
Staging: POP-Q System
The Pelvic Organ Prolapse Quantification (POPQ) system is the recommended objective staging method. All measurements are in centimetres relative to the hymenal ring (zero point). Negative values = inside the introitus; positive = prolapse beyond hymen.
| Stage | Criteria |
|---|---|
| 0 | No prolapse (all reference points within normal range) |
| I | Most distal portion >1 cm above hymen |
| II | Within 1 cm above or below hymen |
| III | >1 cm below hymen but ≤ 2 cm less than tvl |
| IV | Complete eversion (≥ tvl − 2 cm) |
Management
Conservative (Non-Surgical)
-
Lifestyle modification
- Weight loss, treat chronic cough, avoid heavy lifting
- Manage constipation (high-fibre diet, laxatives)
-
Pelvic floor muscle training (PFMT / Kegel exercises)
- First-line for mild to moderate prolapse
- Improves symptoms and may reduce prolapse stage
-
Vaginal pessary
- Mechanical support device inserted into vagina
- Suitable for women who prefer non-surgical management, poor surgical candidates, or pending surgery
- Ring pessary most commonly used; Gellhorn for more severe prolapse
- Requires follow-up every 3–6 months; local oestrogen helps vaginal health around pessary
- Trial of pessary also useful diagnostically: if symptoms improve, prolapse is likely the cause
-
Local (vaginal) oestrogen
- Improves vaginal mucosal health, may reduce severity and improve surgical outcomes
Surgical
Surgery is indicated for symptomatic prolapse that fails conservative management. Principles:
| Approach | Procedure | Target |
|---|---|---|
| Vaginal | Anterior/posterior colporrhaphy (native tissue repair) | Cystocele, rectocele |
| Vaginal | Sacrospinous ligament fixation (SSLF) | Apical (vault) prolapse |
| Vaginal | Manchester repair (amputation of cervix + pelvic floor repair) | Uterine prolapse |
| Abdominal/laparoscopic | Sacrocolpopexy (mesh) | Apical prolapse; low recurrence |
| Vaginal mesh | Mesh-augmented repair | Selected cases; mesh complications well-documented |
| Obliterative | Colpocleisis (LeFort) | Elderly women no longer sexually active |
Concurrent procedures: women with prolapse undergoing surgery should be assessed for occult stress urinary incontinence (SUI) — up to 25% of women with advanced prolapse have occult SUI, which may be "unmasked" after prolapse repair. Urodynamics with prolapse reduction helps guide this decision.
Prolapse & Urinary Symptoms
-
50% of women with stress urinary incontinence (SUI) also have POP
- Anterior compartment repair can significantly reduce overactive bladder (OAB) symptoms (frequency reduced ~33%, urgency incontinence reduced ~49%)
- Cystocele can create urethral kinking → obstructed voiding → detrusor overactivity
- Failure to recognise and repair POP at the time of incontinence surgery increases the need for subsequent prolapse surgery
Recent Evidence (2024–2026)
- A 2024 systematic review (PMID 39250810, Annals of Internal Medicine) confirmed hormonal treatments and vaginal moisturizers are effective for genitourinary syndrome of menopause.
- A 2025 Cochrane review (PMID 41307293) on long-term hormone therapy in peri/postmenopausal women provides updated benefit/risk analysis.
- A 2025 systematic review (PMID 40488293) specifically examined safety of menopause HT in women at higher VTE risk, providing guidance for this challenging patient group.
Summary
| Topic | Key Points |
|---|---|
| Menopause | Median age 52.5; FSH ↑, estrogen ↓; diagnose after 12 months amenorrhea |
| Symptoms | Hot flashes, GSM (persistent), mood/sleep disturbance, osteoporosis |
| HRT indications | Bothersome vasomotor symptoms, GSM, POI, osteoporosis prevention |
| HRT timing | Start within 10 years of menopause / before age 60 for best benefit-to-risk ratio |
| HRT risks | Breast cancer (EPT), VTE (oral > transdermal), endometrial cancer (ET without progestogen) |
| Non-hormonal | Fezolinetant (NK3R antagonist), paroxetine, venlafaxine, CBT |
| Genital prolapse | Downward displacement of pelvic organs; most common: anterior (cystocele) |
| Prolapse staging | POPQ system; Stage 0–IV relative to hymenal ring |
| Conservative Rx | PFMT, pessary, lifestyle, vaginal oestrogen |
| Surgical Rx | Colporrhaphy, sacrocolpopexy, SSLF; assess for occult SUI pre-operatively |
Sources: Goldman-Cecil Medicine International Edition, 2 vol. set (Ch. 222); Guyton & Hall Textbook of Medical Physiology; Campbell-Walsh-Wein Urology, 3-vol. set (Ch. 115); Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.