Explain effect of different anesthetic agent on cerebral autoregulation
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cerebral autoregulation" AND "anesthetic agents"
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I have sufficient data to compile a comprehensive answer. Let me now produce it:
Effect of Anesthetic Agents on Cerebral Autoregulation
Background: What Is Cerebral Autoregulation?
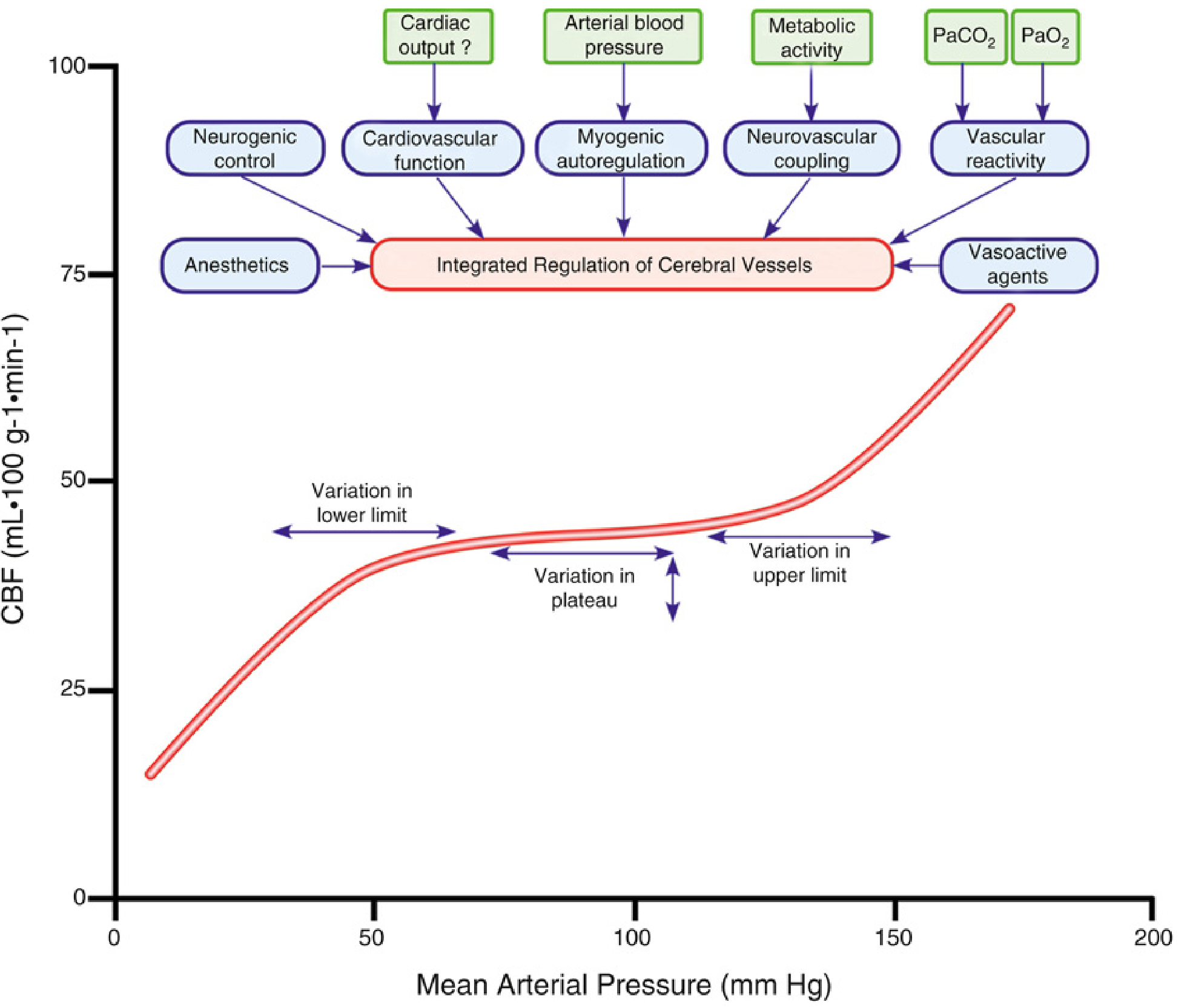
Cerebral autoregulation (CA) is the intrinsic capacity of the cerebral vasculature to maintain a relatively constant cerebral blood flow (CBF) across a range of mean arterial pressures (MAP) — classically ~50–150 mmHg. It is a dynamic process influenced by myogenic tone, neurovascular coupling, arterial CO₂/O₂ tensions, autonomic activity, and cardiovascular function. When CA is intact, the autoregulatory plateau keeps CBF independent of MAP; when impaired, CBF becomes pressure-passive.
Anesthetic agents affect CA at multiple levels:
- Suppression of cerebral metabolic rate (CMRO₂)
- Direct cerebral vasodilation
- Alteration of arterial blood gases
- Suppression of autonomic activity
- Modulation of cardiovascular function
— Miller's Anesthesia, 10e (Fig. 10.10)
I. Intravenous Anesthetic Agents
General Principle
IV sedative-hypnotics (propofol, barbiturates, etomidate, benzodiazepines) reduce CBF indirectly — by decreasing CMRO₂ first, then through flow-metabolism coupling, CBF falls secondarily. Autoregulation and CO₂ reactivity are preserved with these agents. — Barash Clinical Anesthesia, 9e
1. Propofol
- Reduces CBF by 53–79% and whole-brain metabolic rate by 48–58% vs. awake state
- Both CO₂ reactivity and cerebral autoregulation are fully preserved, even at doses producing EEG burst suppression
- Compared with volatile anesthetics, propofol-fentanyl reduces subdural pressure and AVDO₂ in neurosurgical patients
- Clinically preferred for neuroanesthesia due to preserved autoregulation and ICP control
— Miller's Anesthesia, 10e, p. 991–992
2. Barbiturates (Thiopental, Pentobarbital)
- Parallel, dose-dependent reductions in CMR and CBF
- Cause EEG burst suppression at high doses (maximal CMR suppression occurs at this point)
- Autoregulation and CO₂ responsiveness are maintained, even during deep pentobarbital anesthesia
- Note: Tolerance develops quickly — doses needed for burst suppression increase within 24–72 hours in head-injured patients
— Miller's Anesthesia, 10e, p. 991
3. Etomidate
- Produces roughly parallel reductions in CBF (~34%) and CMR (~45%)
- EEG suppression pattern similar to barbiturates; CMR suppression is regionally variable — predominantly forebrain
- CO₂ reactivity is preserved; autoregulation has not been formally evaluated but is presumed preserved given the flow-metabolism coupling mechanism
- Reduces ICP without lowering CPP — useful for induction in neurosurgical patients
- Caveat: adrenocortical suppression limits use beyond episodic application
— Miller's Anesthesia, 10e, p. 992–993
4. Benzodiazepines
- Modest, dose-dependent reductions in CBF and CMR via flow-metabolism coupling
- Autoregulation and CO₂ reactivity are preserved
- Ceiling effect on CMR suppression (unlike barbiturates/propofol, they cannot produce complete EEG suppression)
5. Ketamine — The Exception
Ketamine is the outlier among IV agents:
- Increases CBF and CMRO₂ — unlike all other IV anesthetics
- CBF increases by cerebral vasodilation and heightened neuronal activation (glutamate system)
- Little effect on autoregulation or CO₂ reactivity — racemic ketamine does not abolish cerebrovascular autoregulation
- Can increase ICP; best avoided as the sole agent in patients with impaired intracranial compliance
- May be cautiously used with concurrent sedatives (e.g., propofol, benzodiazepines), which blunt its ICP-raising effects
— Barash Clinical Anesthesia, 9e; Miller's Anesthesia, 10e, p. 1002
6. Opioids (Morphine, Fentanyl, Remifentanil)
- Have relatively little intrinsic effect on CBF, CMRO₂, autoregulation, or CO₂ responsiveness
- Modest reductions in CBF and CMR observed at high doses (partly nonspecific — attributable to reduction in arousal)
- Morphine (2 mg/kg + 70% N₂O): autoregulation intact between MAP 60–120 mmHg
- Fentanyl: CO₂ responsiveness and autoregulation unaffected; hyperemic CBF response to hypoxia remains intact
- Histamine-releasing opioids (e.g., morphine at high doses) can cause cerebral vasodilation via histamine
— Miller's Anesthesia, 10e, p. 993–994
7. Dexmedetomidine
- α₂-adrenergic agonist — reduces CBF through sympatholytic and CMRO₂-suppressive effects
- Autoregulation is generally preserved
- CO₂ reactivity intact
- Useful adjunct in neurocritical care and awake craniotomy
II. Inhaled Anesthetic Agents
General Principle
Volatile agents have a fundamentally different profile from IV agents:
- All are direct cerebral vasodilators (act on vascular smooth muscle)
- Also suppress CMRO₂ in a dose-dependent manner
- Net CBF = balance between metabolic suppression (↓CBF) vs. direct vasodilation (↑CBF)
- Autoregulation is impaired in a dose-dependent fashion — at high doses, CBF becomes fully pressure-passive
— Miller's Anesthesia, 10e, p. 1004; Barash Clinical Anesthesia, 9e
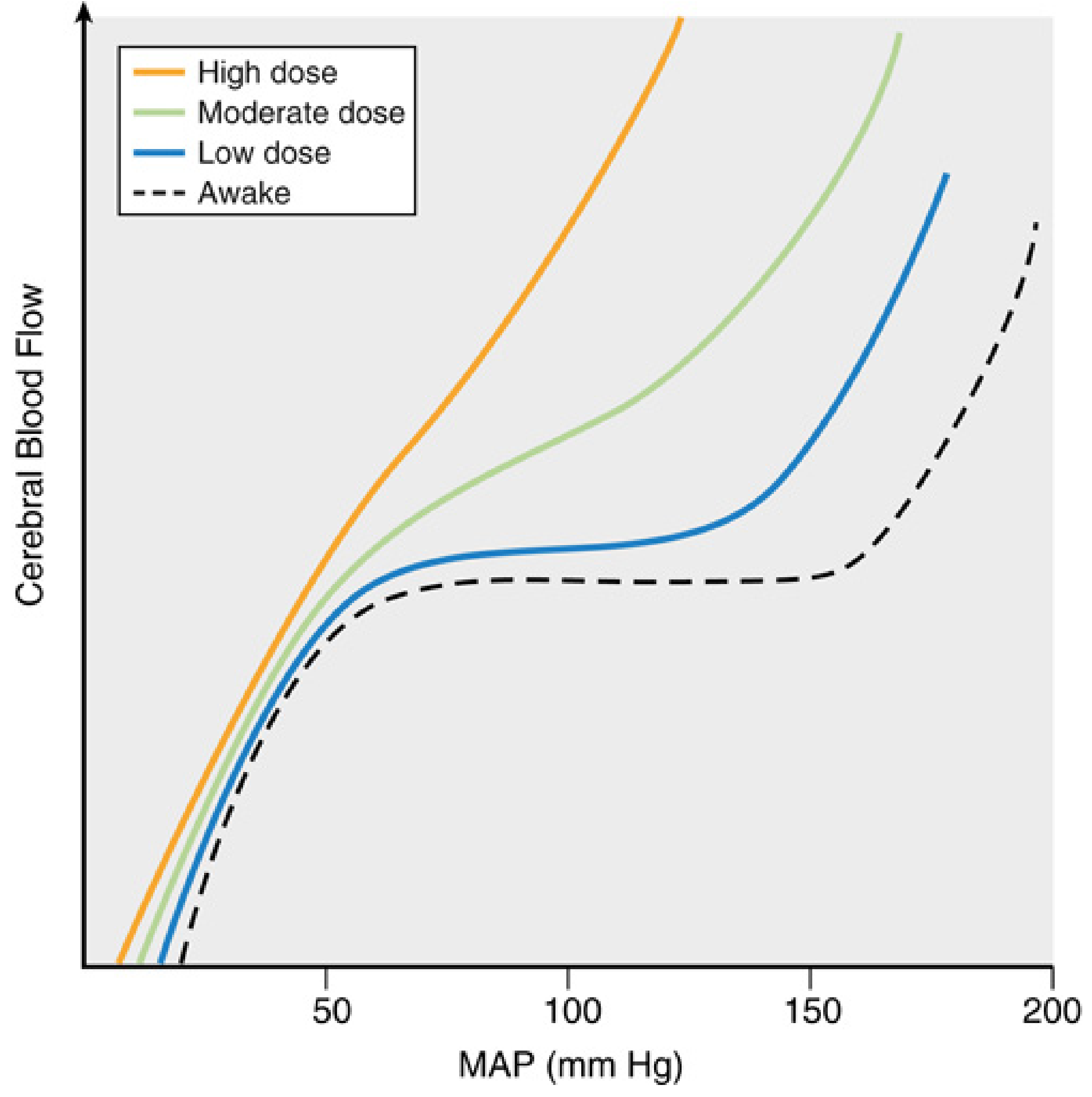
MAC-Dose Relationship for CBF (all modern agents):
| MAC Dose | Net CBF Effect | Autoregulation Status |
|---|---|---|
| 0.5 MAC | ↓ CBF (metabolic suppression dominates) | Preserved |
| 1.0 MAC | Unchanged (effects balanced) | Mildly impaired |
| >1.0 MAC | ↑ CBF (vasodilation dominates) | Progressively impaired |
| High doses | CBF pressure-passive | Abolished |
1. Isoflurane
- At 1.1 MAC: CBF ↑ ~19%, CMR ↓ ~45%
- Reduces autoregulation in a dose-dependent manner
- Minimal ICP increase in most patients; blunted or blocked by hyperventilation or barbiturate co-administration
- Better profile than halothane for cerebral vasodilation at equivalent MAC
2. Sevoflurane
- At 1 MAC: Preserves autoregulation (most favorable among volatile agents)
- At 1.5 MAC: Dynamic CA is better preserved than isoflurane at equivalent dose — likely due to lesser direct vasodilatory potency
- PET studies: ~50% reduction in CBF and CMRO₂ at 1 MAC
- Preferred volatile agent for neuroanesthesia due to relatively preserved CA up to 1 MAC
- Mild ICP increase at >1 MAC; less airway irritation than desflurane (lower bucking/coughing risk → less ICP transient)
— Barash Clinical Anesthesia, 9e; Miller's Anesthesia, 10e
3. Desflurane
- Dose-dependent reduction in autoregulation, similar to isoflurane
- Dynamic CA reduced in a dose-dependent manner; similar to isoflurane profile
- Greater pungency/airway irritation → higher risk of coughing/bucking → ICP transients
- At 1 MAC: CBF ↓ 22%, CMR ↓ 35% vs. awake (slightly less metabolic suppression than sevoflurane)
4. Halothane (Historical)
- Most potent cerebral vasodilator among volatile anesthetics
- At 1.1 MAC: CBF ↑ up to 191% with simultaneous modest CMR decrease (~10%)
- Greatest impairment of autoregulation among volatile agents
- No longer widely used; largely replaced by sevoflurane/desflurane
5. Nitrous Oxide (N₂O)
- Direct cerebral vasodilator; minimal effect on CMRO₂
- Effect on autoregulation is context-dependent:
- When used with propofol: autoregulation preserved
- When added to sevoflurane: CA further impaired
- Caution in neurosurgical patients — may augment the vasodilatory effects of volatile agents
— Barash Clinical Anesthesia, 9e
III. Adjuvant Agents
Lidocaine
- IV lidocaine (5 mg/kg) reduces CBF (~24%) and CMR (~20%)
- Useful adjunct for acute ICP control (e.g., during intubation, suctioning, pin placement)
- Does not impair autoregulation at clinical doses
— Miller's Anesthesia, 10e, p. 1002
Summary Table
| Agent | CBF Effect | CMRO₂ | Autoregulation | CO₂ Reactivity | ICP |
|---|---|---|---|---|---|
| Propofol | ↓↓ | ↓↓ | Preserved | Preserved | ↓ |
| Thiopental | ↓↓ | ↓↓ | Preserved | Preserved | ↓ |
| Etomidate | ↓ | ↓↓ | Presumed preserved | Preserved | ↓ |
| Midazolam | ↓ | ↓ | Preserved | Preserved | ↓ |
| Ketamine | ↑↑ | ↑ | Little effect | Preserved | ↑ |
| Opioids | Minimal ↓ | Minimal ↓ | Preserved | Preserved | Minimal |
| Dexmedetomidine | ↓ | ↓ | Preserved | Preserved | ↓ |
| Isoflurane | ↑ (dose-dep.) | ↓↓ | Dose-dependent impairment | Preserved | ↑ mild |
| Sevoflurane | ↑ (>1 MAC) | ↓↓ | Preserved ≤1 MAC; impaired >1 MAC | Preserved | ↑ mild |
| Desflurane | ↑ (dose-dep.) | ↓↓ | Dose-dependent impairment | Preserved | ↑ mild |
| Halothane | ↑↑↑ | ↓ | Markedly impaired | Preserved | ↑↑ |
| Nitrous Oxide | ↑ | Minimal ↓ | Context-dependent | Preserved | ↑ variable |
| Lidocaine | ↓ | ↓ | Preserved | Preserved | ↓ |
Key Clinical Points
-
Total IV anesthesia (TIVA) with propofol is the preferred technique for patients with impaired intracranial compliance or disrupted autoregulation — it reduces CBF, lowers ICP, and preserves CA.
-
Sevoflurane ≤1 MAC is the safest volatile agent for neuroanesthesia — autoregulation is maintained; above 1 MAC, impairment begins.
-
Volatile agents impair CA in a MAC-dependent manner — at high doses all become cerebral vasodilators and CBF becomes pressure-passive. CO₂ reactivity remains intact even when autoregulation is abolished.
-
Ketamine is the only IV agent that increases CBF and ICP; use cautiously (with sedative co-administration) in neuroanesthesia.
-
N₂O should be used cautiously in neurosurgery — its vasodilatory effect is additive with volatile agents and can further impair CA.
-
Autoregulation is not binary — there is inter-individual variability in the lower limit of autoregulation (LLA), and all anesthetic agents shift the autoregulatory curve rather than abolishing it abruptly.
Sources: Miller's Anesthesia, 10e (Ch. 10); Barash, Cullen & Stoelting's Clinical Anesthesia, 9e (Ch. 18, 37); Morgan & Mikhail's Clinical Anesthesiology, 7e
This is a shared conversation. Sign in to Orris to start your own chat.