Anatomy of liver
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive answer. Let me compile it.
Anatomy of the Liver
Overview
The liver is the largest solid organ and the heaviest gland in the body, weighing approximately 1500 g in adults. It is reddish-brown, resides in the right upper quadrant beneath the diaphragm, and is protected by the lower rib cage. The entire organ is surrounded by a fibrous sheath called Glisson's capsule.
Ligaments and Peritoneal Attachments
The liver is held in position by several ligaments derived from peritoneum:
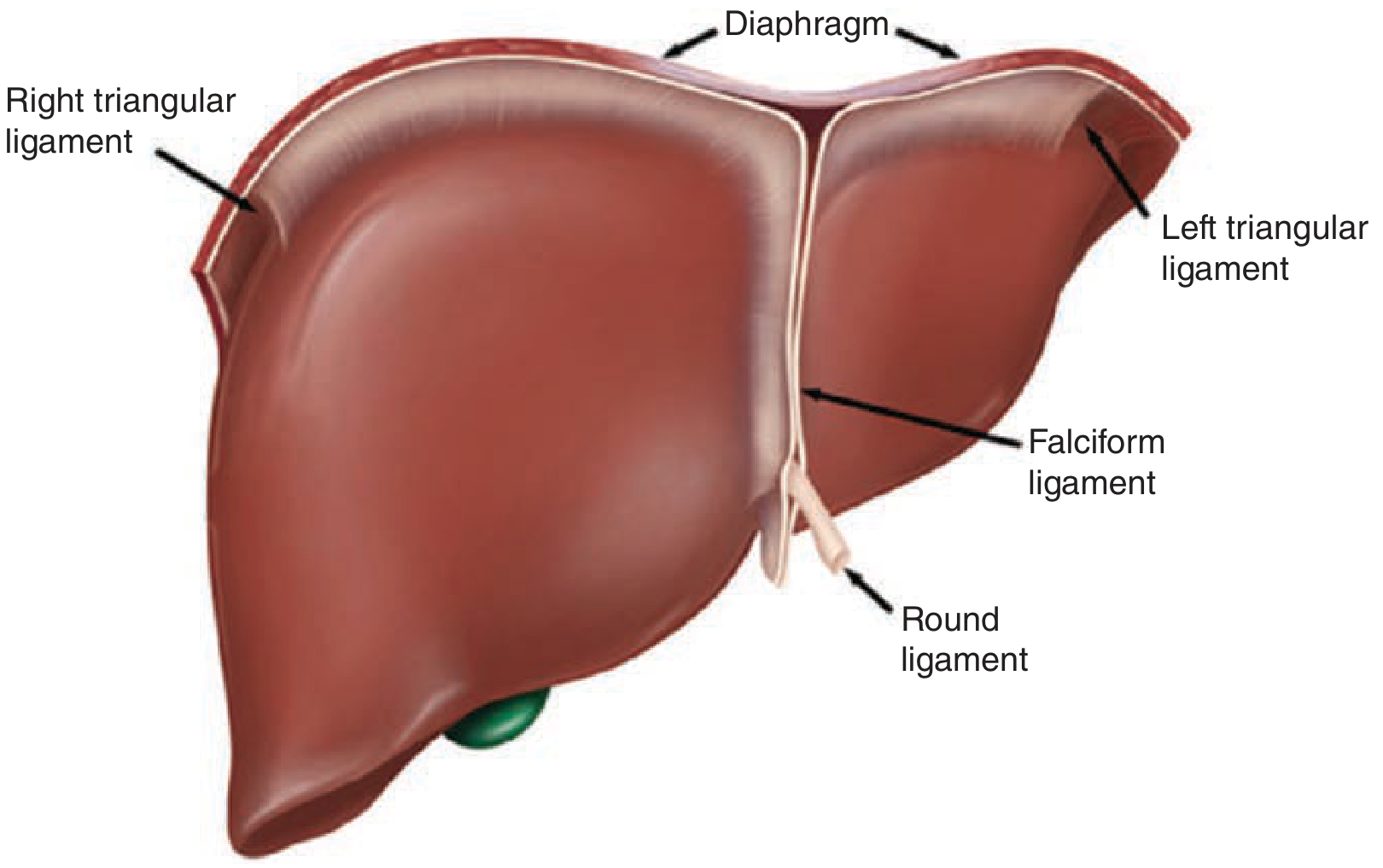
| Ligament | Description |
|---|---|
| Falciform ligament | Connects liver to anterior abdominal wall; separates the left lateral segment from the left medial segment along the umbilical fissure |
| Round ligament (ligamentum teres) | Remnant of the obliterated umbilical vein; runs along the inferior edge of the falciform ligament into the left liver hilum |
| Ligamentum venosum (Arantius' ligament) | Obliterated ductus venosus; lies deep in the plane between caudate lobe and left lateral segment |
| Left & right triangular ligaments | Secure the two sides of the liver to the diaphragm |
| Coronary ligaments | Extend anteriorly from the triangular ligaments; the right coronary also anchors the liver to the right retroperitoneum overlying the right kidney |
| Hepatoduodenal ligament (porta hepatis) | Connects liver to superior duodenum; contains the common bile duct, hepatic artery, and portal vein |
| Gastrohepatic ligament | Connects liver to lesser curvature of stomach |
The foramen of Winslow (epiploic foramen) lies posterior to the porta hepatis and connects to the lesser sac - it allows complete vascular inflow control by clamping the hepatoduodenal ligament (the Pringle maneuver).
Lobes - Anatomical vs. Functional
Anatomical (Surface) Lobes
Grossly, the liver has four anatomical lobes:
- Right lobe - the largest
- Left lobe - separated from the right by the falciform ligament
- Caudate lobe - on the posterior-inferior surface
- Quadrate lobe - on the inferior surface, between the gallbladder fossa and the round ligament
Functional (Surgical) Division
The true functional division is defined by Cantlie's line - an imaginary plane running from the gallbladder fossa to the inferior vena cava (IVC). The middle hepatic vein runs in this plane. The right functional lobe accounts for ~60-70% of the liver mass, while the left lobe (plus caudate) makes up the remainder. The falciform ligament does not separate the right and left functional lobes.
Segmental Anatomy (Couinaud's Segments)
The most important advance in understanding liver anatomy came from the cast-work studies of the French surgeon Couinaud in the early 1950s. He divided the liver into 8 segments, numbered in a clockwise direction with the caudate lobe as segment I.
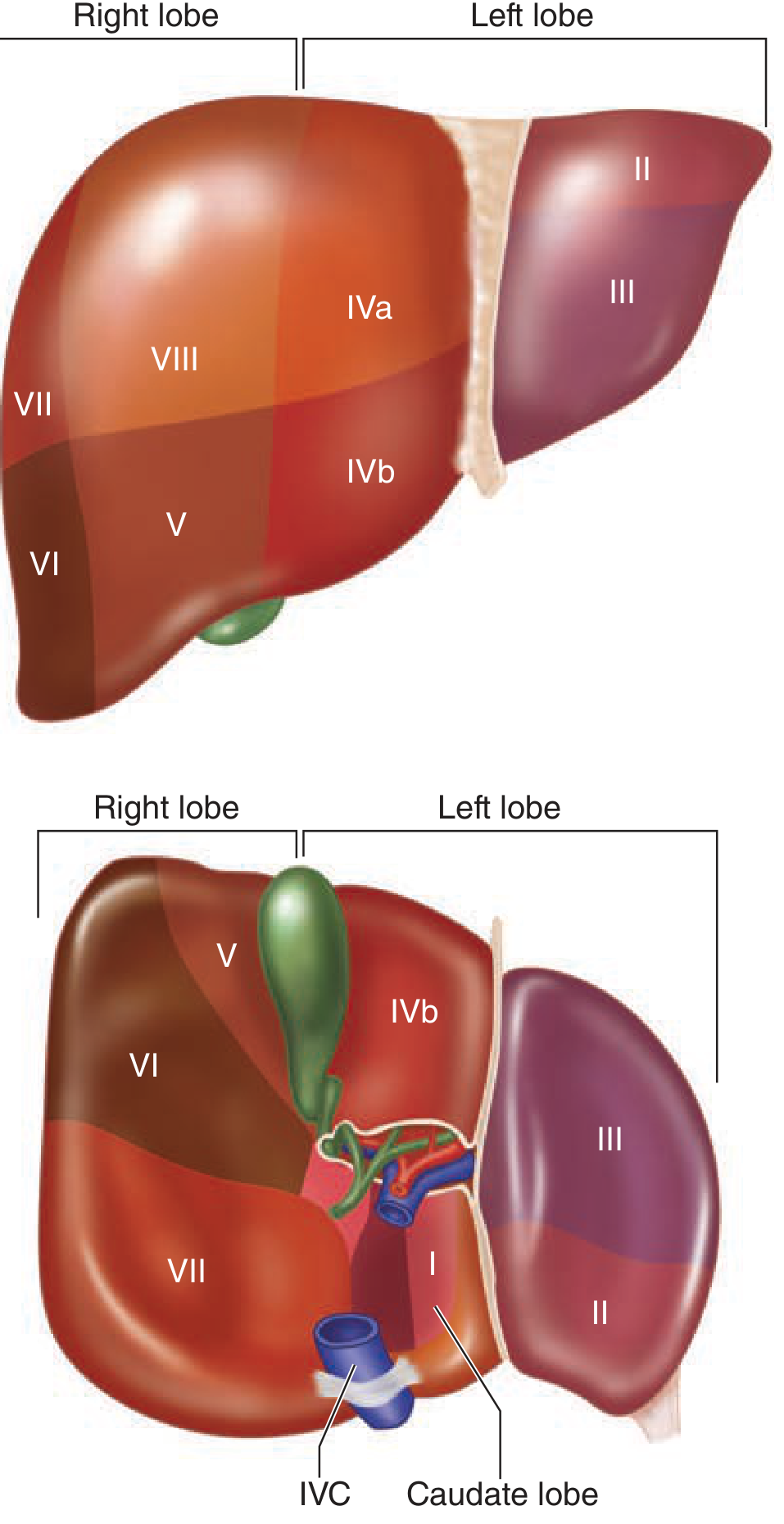
| Segment | Location | Notes |
|---|---|---|
| I | Caudate lobe | Unique - drains directly into IVC |
| II & III | Left lateral segment | Left lobe, lateral portion |
| IV (IVa & IVb) | Left medial segment | IVa is cephalad (near MHV); IVb is caudad (quadrate lobe) |
| V & VIII | Right anterior lobe | V is inferior; VIII is superior |
| VI & VII | Right posterior lobe | VI is inferior; VII is superior |
- Left lobe = segments II, III, IV
- Right lobe = segments V, VI, VII, VIII
- A right hepatectomy removes segments V-VIII; a left hepatectomy removes segments II-IV
Bismuth further described four sectors based on hepatic vein distribution, each running in a fissura (fissure): right hepatic vein divides right posterolateral from right anterolateral sector; middle hepatic vein separates right and left livers; left hepatic vein separates left posterior from left anterior sectors.
Blood Supply
The liver has a dual blood supply:
| Source | Contribution | Origin |
|---|---|---|
| Portal vein | ~75% of blood supply | Confluence of splenic vein + superior mesenteric vein (SMV) |
| Hepatic artery | ~25% of blood supply | Celiac axis (trunk) |
Hepatic Artery
The celiac trunk gives off the left gastric, splenic, and common hepatic arteries. The common hepatic artery divides into:
- Gastroduodenal artery
- Hepatic artery proper → divides into right and left hepatic arteries
The "classic" anatomy is present in only ~76% of cases. Important variants:
- Replaced/accessory right hepatic artery from SMA: 10-15% of cases
- Replaced/accessory left hepatic artery from left gastric artery: 3-10%
- Both replaced right + left: ~1-2%
- Completely replaced common hepatic from SMA: ~1-2%
The cystic artery (to gallbladder) typically arises from the right hepatic artery within Calot's triangle. The right hepatic artery passes posterior to the common bile duct ~88% of the time.
Portal Vein
The main portal vein travels within the porta hepatis before dividing into left and right branches. The left portal vein has a characteristic transverse portion followed by a 90° turn at the umbilical fissure to become the umbilical portion. The caudate lobe receives portal branches from both right and left main portal veins. Portal vein trifurcation or aberrant branching occurs in 20-35% of individuals.
Venous Drainage
Three hepatic veins drain blood into the suprahepatic IVC:
| Vein | Drains |
|---|---|
| Right hepatic vein | Segments V, VI, VII, VIII |
| Middle hepatic vein | Segment IV + portions of V and VIII |
| Left hepatic vein | Segments II and III |
The caudate lobe (segment I) drains directly via its own small veins directly into the IVC - this is what makes it unique.
The left and middle hepatic veins form a common trunk ~95% of the time before entering the IVC; the right hepatic vein inserts separately. A large inferior accessory right hepatic vein is present in 15-20% of cases.
Biliary System
Within the liver, bile flows from:
Bile canaliculi (between hepatocytes) → bile ducts → right and left hepatic ducts → common hepatic duct
The common hepatic duct is joined by the cystic duct from the gallbladder to form the bile duct (common bile duct). The common bile duct lies anteriorly and to the right within the hepatoduodenal ligament. It descends posterior to the superior duodenum and joins the pancreatic duct to enter the descending duodenum at the major duodenal papilla (of Vater).
The gallbladder sits adherent to hepatic segments IVb and V. Biliary duct variants exist in 30-40% of cases.
Microanatomy - The Hepatic Lobule and Acinus
The liver is composed of 50,000-100,000 discrete anatomic units called lobules.
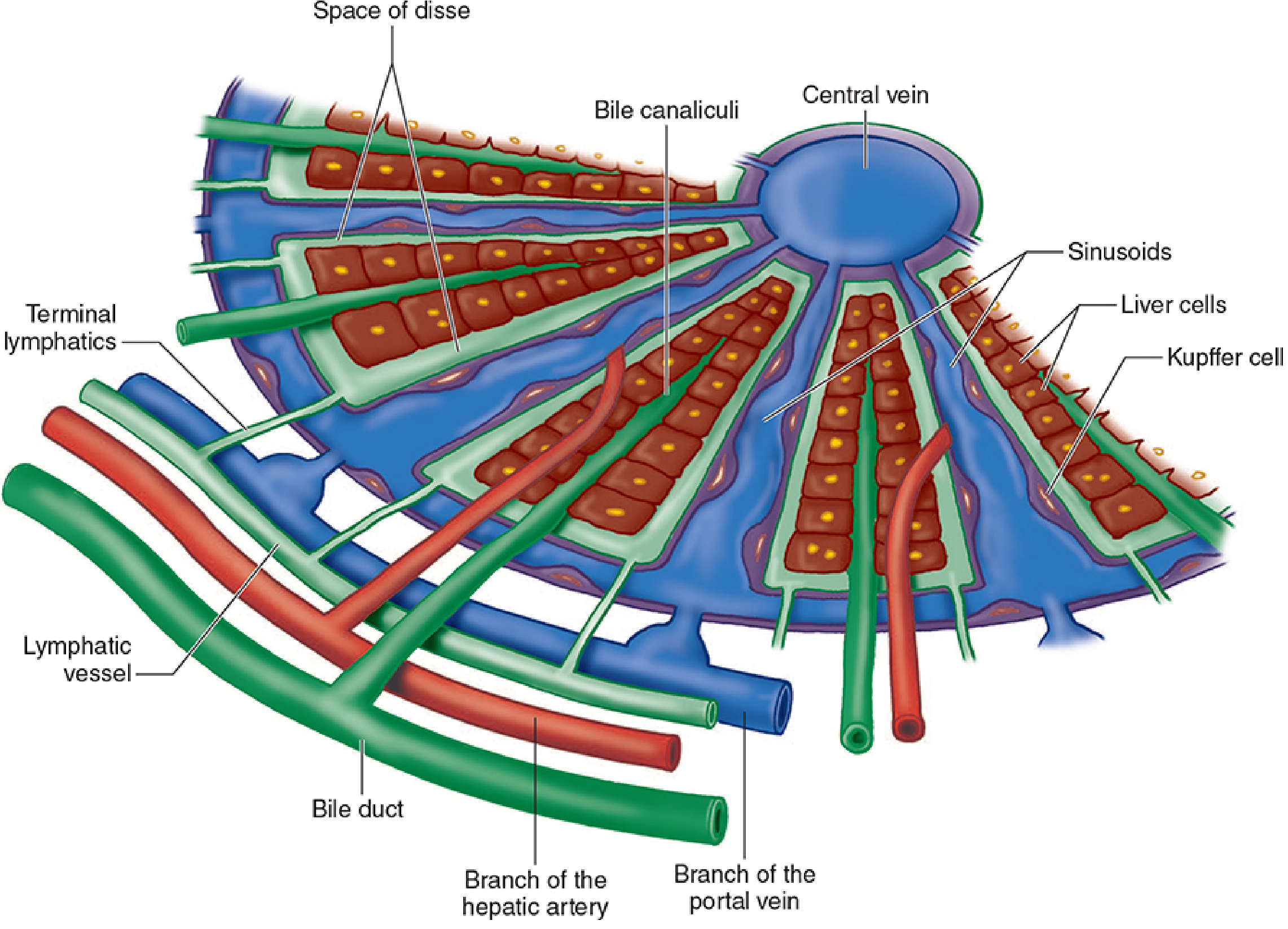
Hepatic Lobule
- Hepatocytes are arranged in plates radiating cylindrically around a central centrilobular vein
- 4-5 portal tracts surround each lobule, each containing: hepatic arteriole, portal venule, bile ductule, lymphatics, and nerves (collectively the portal triad)
- Blood flows inward from portal tracts → through sinusoids → to the central vein
Hepatic Acinus (Functional Unit)
The acinus (not the lobule) is considered the true functional unit:
- A portal tract sits at the center; centrilobular veins are at the periphery
- Zone 1 (periportal) - cells closest to portal tract; best oxygenated; first to regenerate after injury
- Zone 2 (midzonal)
- Zone 3 (centrilobular) - farthest from portal tract; least oxygenated; most susceptible to ischemic injury and toxic drug injury (e.g., acetaminophen toxicity)
Sinusoids
- Lie between hepatocyte plates
- Lined by endothelial cells and Kupffer cells (resident hepatic macrophages)
- Kupffer cells remove bacterial endotoxins, viruses, proteins, and particulate matter
- The space of Disse lies between sinusoidal capillaries and hepatocytes - this is where hepatic lymph forms
Innervation and Lymphatics
- Sympathetic: T6-T11 fibers
- Parasympathetic: Left vagus (anterior hepatic branch) and right vagus (posterior hepatic branch)
- Right phrenic nerve also contributes (explains referred shoulder pain with liver pathology)
- Lymphatics: An extensive network forms within hepatocyte plates, communicating directly with the space of Disse; hepatic lymph drains to the celiac lymph nodes
Summary Table
| Feature | Details |
|---|---|
| Weight | ~1500 g |
| Anatomical lobes | Right, Left, Caudate, Quadrate |
| Functional segments | 8 (Couinaud) |
| Arterial supply | Hepatic artery (25%) + Portal vein (75%) |
| Venous drainage | Right, Middle, Left hepatic veins → IVC |
| Functional unit | Hepatic acinus (3 zones) |
| Structural unit | Hepatic lobule (50,000-100,000) |
| Phagocytic cells | Kupffer cells (sinusoid lining) |
| Capsule | Glisson's capsule |
| Key surgical landmark | Cantlie's line (gallbladder fossa → IVC) |
Sources:
- Schwartz's Principles of Surgery, 11th Edition, Chapter 31
- Morgan & Mikhail's Clinical Anesthesiology, 7th Edition, Chapter 33
- Gray's Anatomy for Students, Chapter 4
- Yamada's Textbook of Gastroenterology, 7th Edition, Chapter 10
- Bailey and Love's Short Practice of Surgery, 28th Edition
This is a shared conversation. Sign in to Orris to start your own chat.